

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Chronic pain is a common complaint among patients with spinal cord injury (SCI) [1,2,3,4,5]. It affects several aspects of their life, mostly the quality of life (QoL) [6,7]. Therefore, it has received increasing attention among researchers within the last several years.
Recent studies have attempted to define or categorize various types of pain following SCI, which have led to significant advances in understanding and managing pain [2,8,9,10,11]. Most classifications were based on the source or site of pathology, etiology, mechanism and the severity of pain. However, the quality of pain and the location of pain have also been considered. Among different methods of SCI pain classification, the preferred one categorizes pain into 4 major divisions: musculoskeletal (nociceptive), visceral, neuropathic (at-level and below-level) and other types of pain not meeting the criteria of any group [10]. Among these, nociceptive pain refers to the pain that arises from musculoskeletal structures and is assumed to be present at any region where there is some preserved sensation above, at or below the spinal lesion [10]. According to the nature of this type of pain, it is believed it can be effectively managed by traditional therapies, compared to the other types of SCI pain [12,13]. Besides, in patients with SCI, it seems that the lumbar, cervical and shoulder are the most common sites of musculoskeletal pain, and their effect on patients' daily living is clear.
Previous studies have evaluated the predictors of pain and the impact of pain on the QoL of patients with SCI, which have resulted in the belief that pain is one of the most significant consequences of SCI, causing inability in both fields of physical and psychological functioning [7,14,15]. However, there is not much known about the characteristics and correlates of musculoskeletal pain in patients with SCI.
This study aimed to evaluate lumbar, cervical and shoulder pain (the most disabling types of musculoskeletal pain), their correlates and their effects on patients' day-to-day life in a population of war veterans with SCI, in order to help designing more effective programs for the rehabilitation of these patients.
MATERIALS AND METHODS
A cross-sectional study was performed at Khatam-Al-Anbia hospital during May and August 2011, including male veterans suffering from spinal cord injury admitted to our center for regular follow-up. Data was gathered using a self-reported questionnaire distributed to the participants. Each questionnaire was accompanied with an introductory statement explaining the purpose of the study and the patient's privacy. This information served as the informed consent statement, as required by the Institutional Ethics Committee.
A general questionnaire was developed consisting of three parts of patients' basic information, QoL and pain related questions. A number of questions were designed to assess the patients' demographic and SCI related information such as age, years since injury, age at SCI, weight, height, body mass index (BMI), educational level, cause of injury and level of injury. Patients' weight was measured using a wheelchair balance scale by subtracting the wheelchair weight from the patient and wheelchair total weight, and for abled patients by standing on the same scale. Height was measured using a wall mounted stadiometer for patients able to stand erect and by a supine stadiometer for those unable to stand. BMI was calculated using the [weight / (height)*2] formula. The level of injury and the presence of pressure ulcer were confirmed by a neurosurgeon.
To evaluate the patients' QoL and subjective quantitative health status, EuroQoL [16] was used, consisting of EuroQoL 5-Dimensions 3-levels (EQ-5D-3L) and EuroQoL Visual Analogue Scale (EQ-VAS) in 5 dimensions of mobility, self-care, usual activity, pain/discomfort and anxiety/depression. General Health Questionnaire (GHQ) 12 [17] was applied to assess the patients' self-reported health status during the last several weeks as well. Using the conventional scoring for GHQ, the method of (0-0-1-1) with the max score of 12 was used to estimate the patients' mental health problems; so the higher the score, the greater the severity of the problem. The survey also included a number of questions covering sleep disorders, underlying diseases (UD) and lifestyle, including exercise and smoking habits.
The questionnaire contained questions of pain itself in three regions of lumbar, cervical and shoulder pain. Each part was designed to assess the quality of pain, severity of pain and the influence of pain on daily life consisting of activities such as shopping, self-care and usual house work, working abilities and participating in social activities. Pain severity included 3 questions about the pain at the time of admission, the most severe pain experienced by the patient during the last 6 months and mean pain severity during the last 6 months. Answers for pain severity and the influence of pain on daily life were in the range of 0-10 (0 the min and 10 the max) reported by the responders. The patients were also asked to report the number of days that pain had influenced their daily activities, such as personal and routine activities, during the last 6 months.
SPSS software version 16.00 (SPSS Inc., Chicago, IL) was applied for statistical analysis. To compare quantitative values, student's t test or correlate binary test and to compare the proportions the chi-square test or Fisher's exact test were used. Level of statistical significance was set as P < 0.05.
RESULTS
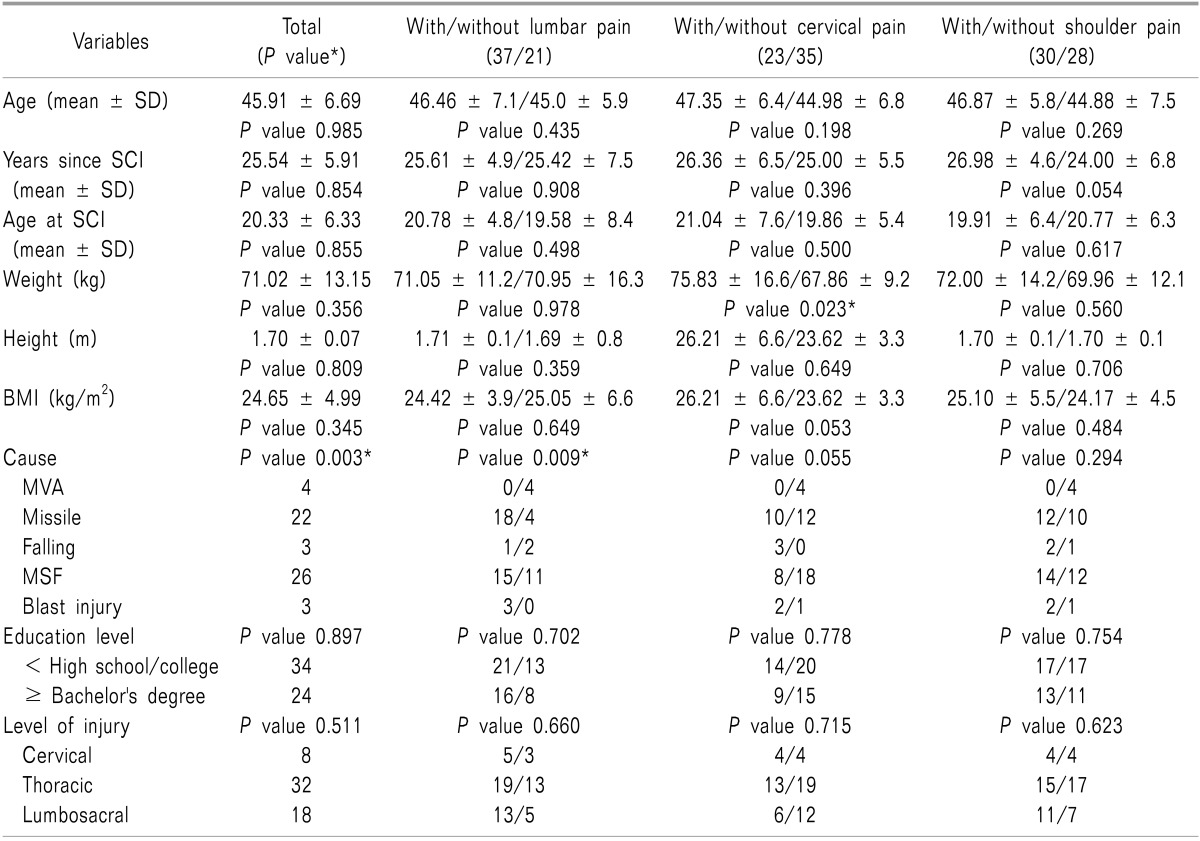
During the study, a total of 134 patients with SCI were admitted to Khatam-Al-Anbia hospital. However 62 patients were either not able or not willing to participate in the study which led to the response rate of 53.74%. Furthermore, a total of 14 patients refused to answer the musculoskeletal part or partially completed the questionnaire remaining 58 responders for final assessment. The demographic and SCI-related descriptive information of the 58 participants and their association with the presence of pain are presented in Table 1 regarding the pain site. The results showed that patients with cervical pain were significantly much more obese than patients without cervical pain. Additionally, patients with lumbar pain were more likely to be injured by missiles, metal shrapnel fragment and blast injury compared to the patients without lumbar pain, among whom motor vehicle accidents and falling were the most likely causes of injury in these patients.
Patients' mean age was 45.91 ± 6.69 years (20-66 years) and the mean injury time was 25.54 ± 5.91 years (1-47 years). A total of 44 patients (75.9%) reported pain in at least one region including lumbar, cervical or shoulder pain; however, 14 patients (24.1%) had no complaints of pain. The prevalence of lumbar, cervical and shoulder pain was respectively 63.8% (37 patients), 39.7% (23 patients) and 51.7% (30 patients).
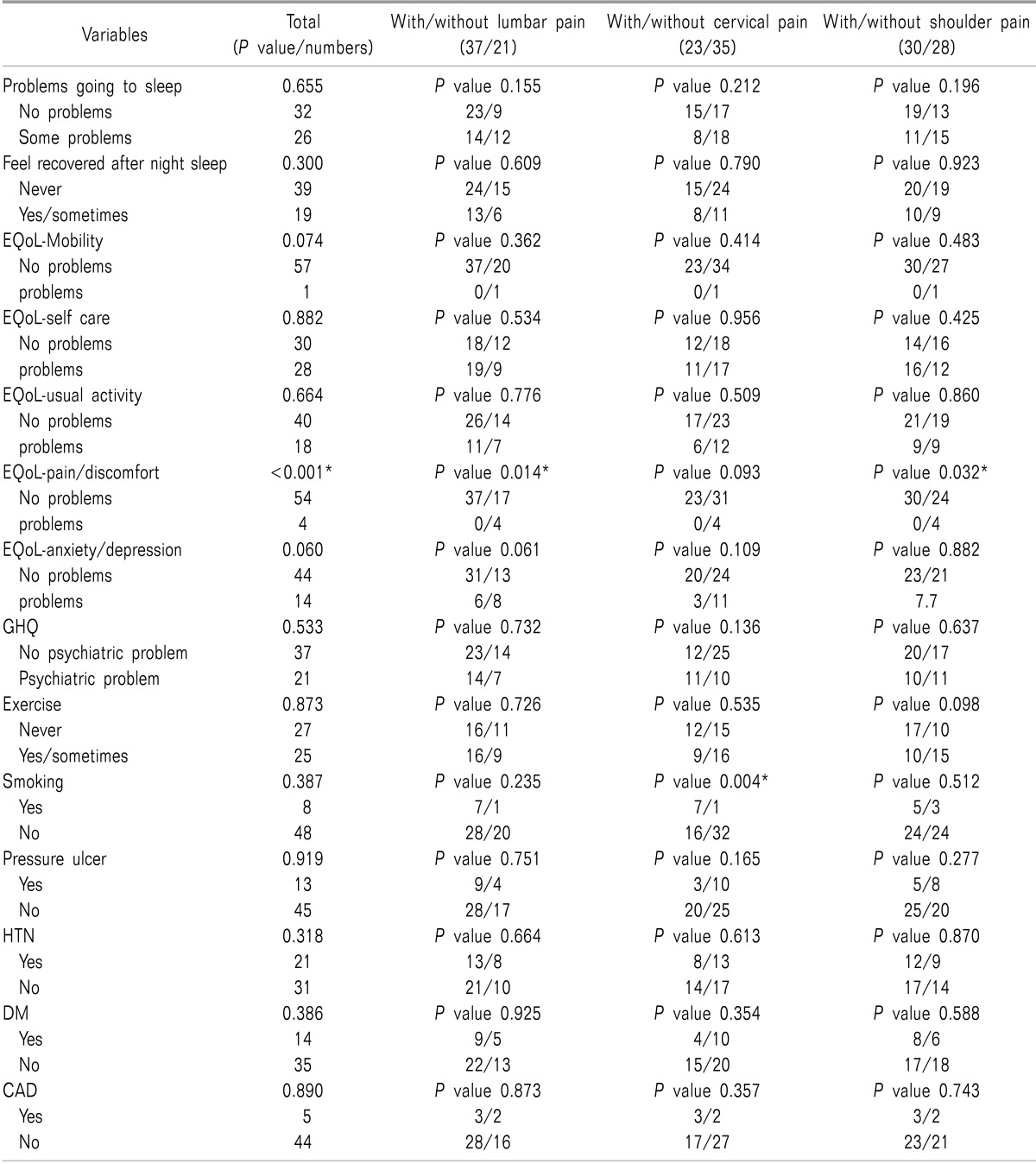
The association between factors related to QoL including EQoL parameters, GHQ score, UD and exercise and smoking habits with the presence of pain in each region individually are presented in Table 2. The results defined that patients with overall pain reported more discomfort compared to those without pain. This was clear for patients with lumbar and cervical pain. Furthermore, the smoking rate was significantly higher in patients with cervical pain compared to those without cervical pain.
At the time of admission, the most severe pain experienced by a patient during the last 6 months and the mean pain severity in the last 6 months are shown in Table 3. Report of pain severity at the time of admission was higher among the patients with lumbar pain compared to the patients with cervical and shoulder pain. The mean days of pain influencing patients daily activities during the last 6 months was 10 (0-180) days for lumbar pain, 17 (0-90) days for cervical pain and 17.5 (0-90) days for shoulder pain.
Patients' report of the influence of pain on daily activities, participating in social activities and working abilities is presented in Table 4 regarding the pain site. The overall influence of pain in daily life was higher in patients with lumbar pain.
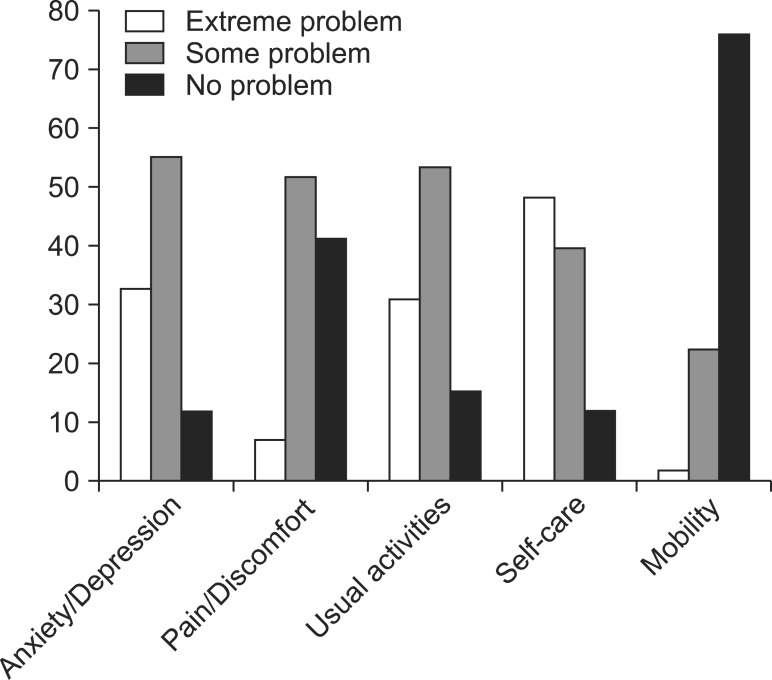
The demographics of the patients' QoL are presented in Fig. 1. A total of 37 patients had general health problems. The highest and the lowest rate of extreme problems reported by the patients were in the fields of mobility (75.9%) and self-care (12.1%).
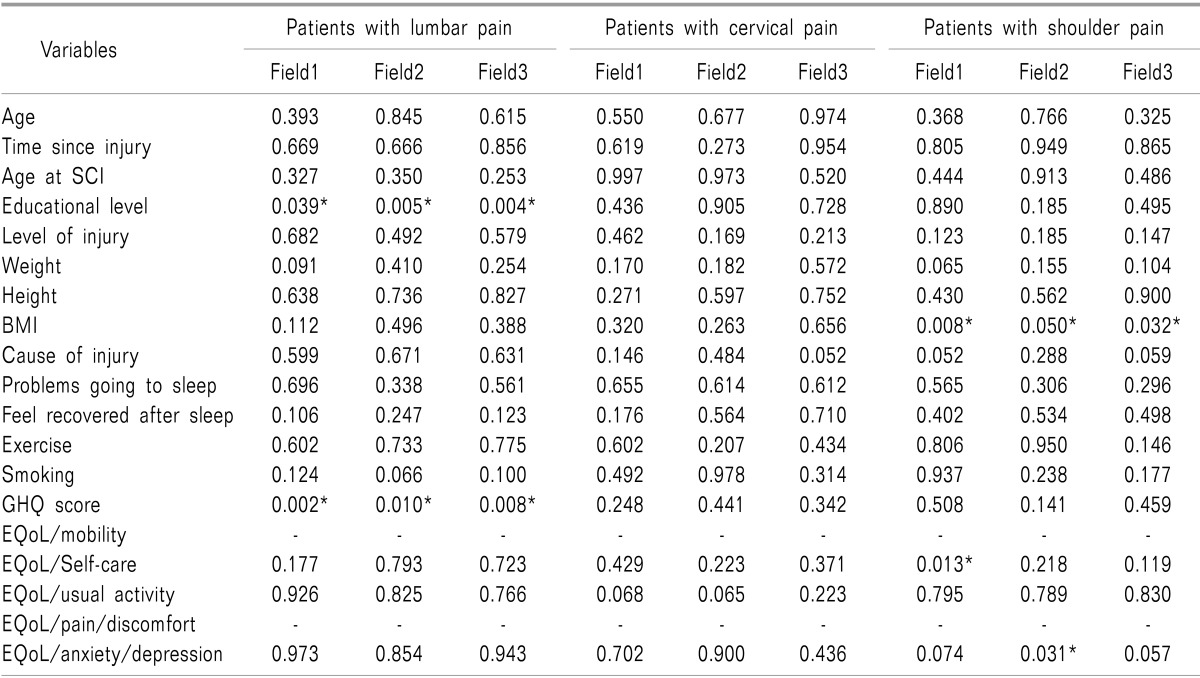
We selected the patients with lumbar, cervical and shoulder pain each time separately to assess the association between predictive factors with the patients' report of the influence of pain on 3 parts of daily life in each group. The results are presented in Table 5. Lower educational level and lower GHQ score in patients with lumbar pain and higher BMI, presence of self-care problems and anxiety/depressive disorder in patients with shoulder pain were associated with a greater influence of pain on patients' daily living.
DISCUSSION
Pain is a major problem among patients with SCI, imposing several limitations to the patients. A previous study in England reported that 11% of patients with SCI consider pain rather than mobility disorder as a deterrent in their daily activities [18]. Another study reported 37% of patients with high level lesions and 23% of patients with low level lesions were willing to exchange loss of reacquired physiologic functions for pain relief [19]. Hence, it is important to look for possible predictors of pain and try to reduce them in patients with SCI. This study was performed to evaluate the prevalence of pain and its correlates in a population of war veterans with SCI and to assess the impact of pain in patients' daily life.
In our study, 75.9% of patients with SCI reported pain in at least one region including lumbar, cervical or shoulder pain and the prevalence of lumbar pain (63%) was higher compared to shoulder pain (51%) and cervical pain (39%). The reports of the prevalence of pain in patients with SCI were different in previous studies. The condensation of 10 studies during last decade, showed that pain was present in 69% of patients with SCI and almost one third of patients reported severe pain, which was consistent with two other studies that had reported pain in 66% of patients with SCI [20,21]. In a longitudinal study, the prevalence of pain, 6 months after the injury was 64% and 12 months after patients' discharge from hospital was 63% [22]. However, other studies have reported pain in 34% to 90% of patients with SCI and the prevalence of severe pain was in a range of 12% to 30% in different studies [23,24].
Despite the high prevalence of pain in patients with SCI, there is not a clear understanding of its predictive factors. The association between age and the presence of pain is controversial in previous findings [3,25]. The results of our study showed that there is not a significant association between age and pain. Besides, our results were consistent with previous findings that had reported no association between injury duration and age at SCI with the presence of pain [26,27]. Factors such as level of injury and cause of injury have been considered as predictive factors of pain in previous findings [4,21,28]. The results of our study showed that there is a significant association between cause of injury and the presence of pain, mostly lumbar pain; however, no association was found between the level of injury and pain.
Previous studies have shown the negative impact of pain on the QoL of patients with SCI [7,14,15,29]. Chronic pain is also reported to be associated with anxiety/depressive disorder [26]. The results of our study showed that pain, especially lumbar and shoulder pain, are accompanied by feelings of discomfort in patients with SCI. Sleep is another major problem in patients with SCI [30]. Despite a previous study that has reported pain as a primary reason for poor quality of sleep [31], we did not find any association between pain and sleep disorders. This difference may be because of other factors affecting patients' sleep quality. Patients with SCI and chronic pain are supposed to have increased risk of coronary artery disease (CAD), diabetes mellitus (DM), hypertension (HTN) and pressure ulcer due to their low activity lifestyle. However, in our study there was not a significant association between these factors and the presence of pain in any region. Smoking and obesity are also considered as accompanying factors of pain in general population [32,33]. In our study, obesity and smoking were associated with the presence of cervical pain. Other factors related to QoL were not significantly different between patients with and without pain.
Previous studies reported frequent interference of pain with daily activities in patients with SCI [34,35,36]. The interference was even present in a number of important basic activities of daily living [37]. In our study, patients with lumbar pain reported a greater effect of pain on 3 fields of daily life, including usual activities, working abilities and participating in social activities, rather that patients with cervical and shoulder pain. The results showed that in patients with lumbar pain, educational level and GHQ score were associated with the interference of pain with daily activities. In patients with shoulder pain, high BMI was directly associated with a greater influence of pain on daily activities; however, in these group, patients with self-care problems reported a greater effect of pain on routine activities and patients with anxiety/depressive disorder had more problems in social activities.
Our study's sample size was quite small and the investigation was restricted to men in order to obtain a homogenous sample. However, we failed to gather complete data in some fields, such as completeness of injury. These factors may impose limits to our results.
In conclusion, the results of our study showed the high prevalence of musculoskeletal pain, notably lumbar pain among patients with SCI. Patients with lumbar and shoulder pain rather than cervical pain suffer from feelings of discomfort and the impact of pain on a patient's daily living is significantly higher than those with lumbar pain. Hence, it is important to set priorities and design effective programs in the management of pain and the improvement of QoL in patients with SCI.


 XML Download
XML Download