

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Fluoroscopy is a machine that generates X-ray images and presents them continuously as visible images during a diagnostic or interventional procedure [1]. C-arm fluoroscopy is frequently utilized and absolutely necessary in modern pain medicine [2]. Although fluoroscopy enhances the patients' safety and increases the accuracy, it also exposes clinicians to the cumulative doses of ionizing radiation [3]. The adverse effects of ionizing radiation on human bodies include skin diseases, thyroid cancer, brain tumors, cataracts and so on [4]. Such effects are largely divided into two types. The "early effects" are acute radiation lethality, local tissue damage on the skin or gonads, hematologic effects, and cytogenetic effects, and the "late effects" are radiation-induced malignancies such as leukemia and other forms of cancer, deleterious local tissue effects, chromosomal toxicity, and/or cataract formation [5]. Therefore, for the safety of the patients and clinicians it is essential and mandatory to reduce the radiation exposure as far as possible. Available patient dose reduction technologies include low fluoroscopy dose rate settings, low frame rate pulsed fluoroscopy, spectral beam filtration, and use of increased X-ray beam energy [6]. Although pulsed and low-dose fluoroscopy has the potential to greatly reduce the radiation exposure of clinicians involved in interventional procedures, few studies have quantified the reduction in radiation-absorbed doses (RADs) according to the C-arm modes. The purpose of this study is to compare how much the RADs are reduced when using fluoroscopy in the C-arm modes.
MATERIALS AND METHODS
We measured the cumulative exposure time, RADs, peak X-ray energy (kVp), current (mA) in the C-arm fluoroscopic modes including the 'conventional mode', 'pulsed mode', 'low-dose mode', and 'pulsed + low-dose mode'. A pulsed fluoroscopic mode of 15 frames per second was used. The C-arm fluoroscopy was the OEC® fluoroscopic unit (9800 Plus, Salt LakeCity, Utah) and the automatic brightness control (ABC) that manipulates the peak X-ray energy and the current of the fluoroscopic X-ray beam that provides the appropriate image contrast and brightness on the viewing monitor were used in the study. Clinical imaging conditions that are typical in interventional procedures were simulated using a 0.85 mm lead equivalent thick apron instead of a patient. According to each mode, one experimenter radiographed the lead apron, which was on the table, 5 times consecutively on the anteroposterior view and tried to press the X-ray on switch for the same time intervals (Fig. 1). We regarded this as one set and a total 10 sets were done according to each mode. The cumulative exposure time, RADs, peak X-ray energy, and current that were viewed on the monitor were recorded. Data were analyzed by one-way ANOVA followed by Turkey's test for multiple comparisons. Analytical results were considered statistically significant if the P value was less than 0.05.
RESULTS
The mean cumulative exposure time, RADs, peak X-ray energy, and current according to the C-arm modes are presented in Table 1.
2. RADs and RADs/Time
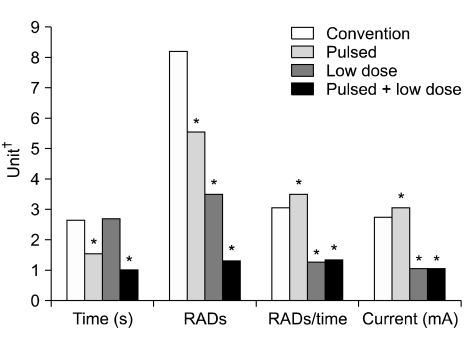
The mean RADs was significantly lower in the pulsed (5.6 ± 1.8), low-dose (3.5 ± 0.2), and pulsed + low-dose modes (1.4 ± 0.3) than in the conventional mode (8.2 ± 0.4). The mean RADs/Time was significantly lower in the low-dose (1.2) and pulsed + low-dose modes (1.4) than in the conventional mode (3.1). The mean RADs/Time in pulsed mode (3.5) was similar to that of the conventional mode (3.1) (Table 1, Fig. 2).
3. Peak X-ray energy and Current
All modes were pretty much the same for the peak X-ray energy. However, the mean peak X-ray energy was higher in the pulsed + low-dose mode (83.9 ± 0.3) than in any other modes and the mean peak X-ray energy was lower in the conventional mode (80.0) than in any of the other modes. The mean current was significantly lower in the low-dose (1.1) and pulsed + low-dose modes (1.1) than in the conventional mode (2.8 ± 0.4). The mean current in the pulsed mode (3.1 ± 0.1) was similar to that of the conventional mode (2.8 ± 0.4) (Table 1, Fig. 2, and 3).
DISCUSSION
Modern fluoroscopes typically offer two modes of fluoroscopy: either the X-ray beam is continuously on, or the X-ray beam is pulsed on for only a few strobe-like pulses of X-rays each second [7]. Manufacturers commonly offer clinicians a choice of several different fluoroscopic pulse rates ranging from a minimum of 2 or 3 frames/s, to a maximum of 30 frames/s (usually called continuous fluoroscopy by most manufacturers) [8].
Pulsed fluoroscopy can always decrease the radiation dose. In this study, the 15 frames per second pulsed mode showed a significantly decreased exposure time by 41% and decreased RADs by 32% compared to the conventional mode. The reason for this is that manufacturers increase the duration or the amplitude or power of each fluoroscopic radiation pulse as the fluoroscopic pulse rate is decreased. They do this to retain at least reasonable image quality [9]. With the low-dose mode, the exposure is reduced through the adjustment of the peak X-ray energy and current to create the X-ray beam [3]. In this study, the low-dose mode showed a significantly decreased current by 60% and decreased RADs by 57% and slightly increased peak X-ray energy by 4% compared to the conventional mode. The pulsed + low-dose mode showed significantly decreased RADs by 83% and decreased exposure time by 63% compared to the conventional mode. Conclusively, using the pulsed mode and low-dose modes together showed significantly decreased RADs than in any other mode.
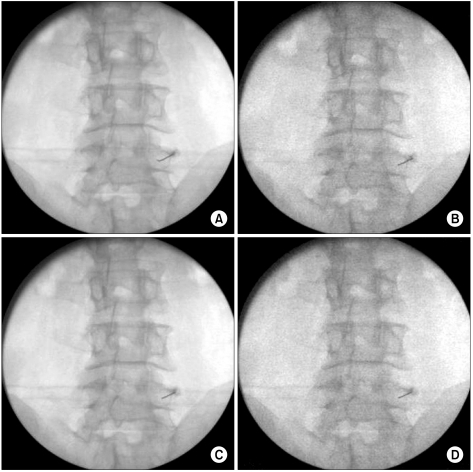
Pulsed fluoroscopy has 2 disadvantages. On a real-time fluoroscopic image, as the pulse rate is lowered, the cumulative radiation dose decreases, and the real-time fluoroscopic image becomes more noisy or grainy [9]. According to the C-arm modes, four fluoroscopic images blocking the lumbar medial branch nerves were shown in Fig. 4. The fluoroscopic image was darker and grainier in the pulsed mode (B) than in the conventional mode (A) because the increased current applied to the X-ray tube produces more X-rays, and the more X-rays that strike the image intensifier, the darker the image is [10]. The fluoroscopic image was brighter with less contrast between the different tissues in the low-dose mode (C) than in the conventional mode (A), thereby reducing the image detail. In our experience, generally, a low-dose fluoroscopic image is a slightly better detailed image than the 15 frames per second pulsed fluoroscopic image. However, the X-ray dose and image quality are interrelated and the image may differ due to the patients weight, fluoroscopic pulse rate, peak X-ray energy, current and X-ray tube-patient-image intensifier distance [11,12]. A trade-off between image quality and radiation exposure is inevitable, however, supportive techniques are considered to provide optimal image quality while reducing radiation exposure to a level as low as reasonably achievable.
Collimation is helpful in optimizing the image quality because the ABC mode attempts to optimize the image quality by taking into account the exposure needed across the entire field of exposure. Useful application of collimation can exclude areas of greatly varying radiodensity to improve the image quality by reducing the range of densities included in the field [6]. The clarity of small structures, or image detail, can be improved by lowering the peak X-ray energy and by reducing the distance between the patient and the image intensifier [10].
Second, with very slow pulse rates, motion such as swallowing or peristalsis becomes jerky [9]. However, continuous fluoroscopy is not the only alternative. The human visual system requires a certain of amount of time (0.2 s) to "integrate" an image. This integration time suggests that there may be little image-quality reward from continuous fluoroscopy, because the human visual system will produce strobelike images for interpretation, regardless if the X-ray beam is on continuously or not [13]. Pulsed fluoroscopy can also provide better temporal resolution for moving objects than continuous fluoroscopy since pulsed fluoroscopy provides strobelike "stop-motion" images at a variable number of pulses per second [14].
This study has limitations such as not measuring the biological effects of the RADs (BERADs) and only measuring the RADs itself. However, since RAD is proportional to BERAD, we can predict the BERADs on the body according to the C-arm fluoroscopic modes.
In conclusion, the use of the pulsed and low-dose modes together significantly reduced the RADs compared to the conventional mode. Therefore, the proper use of the fluoroscopy and its C-arm modes will reduce the radiation exposure of patients and clinicians. Because of the reduced image quality with the pulsed and low-dose settings, however, an ideal way to reduce the RADs would be to use these modes intermittently during a procedure. When the clinicians do not need detailed image quality such as a medial branch block, they can use the pulsed and low-dose modes together. If clinicians need images with more details, using the low-dose mode is another alternative. Supportive techniques such as collimation, lowering the peak X-ray energy, reducing the distance between the patient and the image intensifier are considered to provide the optimal image quality. Continuous or conventional modes can be used during image setup for a procedure using distance and shielding to protect against radiation exposure.


 XML Download
XML Download