

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes can lead to many complications in the long term, including retinopathy, neuropathy, and renal diseases [1]. According to the Korea National Health and Nutritional Examination Survey 2016, 15.8% of men and 13.0% of women aged 30 years or older were diagnosed as having diabetes [2]. Diabetes mellitus is diagnosed based on symptoms, fasting plasma glucose concentration, oral glucose tolerance test, and glycated Hb (HbA1c) measurement. Among these, HbA1c reflects blood glucose status over the three prior months and is widely used because it plays an important role in predicting the prognosis of the therapeutic effect as well as in diagnosis and follow-up [34]. As HbA1c test results have become more important and the demand for the test has increased, fast and accurate reporting of HbA1c test results has become one of the main challenges. HbA1c can be measured by several methods: ion-exchange HPLC, boronate affinity HPLC, enzymatic assay, immunoassay, or electrophoresis [5]. The International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) reference methods for measuring HbA1c concentration are HPLC-mass spectrometry (MS) and capillary electrophoresis (CE) [5], but the use of these assays is limited because of cost-effectiveness issues and turnaround time. Many Korean laboratories preferentially use HPLC to measure HbA1c concentration because of its stability and the possibility to directly identify Hb variants from the chromatogram. According to the quality assurance program in Korea, about 75% of laboratories employed HPLC in 2014 [6]. Accurate HPLC-based measurement of HbA1c concentration may be difficult in patients with Hb variants, when an abnormal chromatogram is present.
Recently, substantial efforts have been made to measure HbA1c concentrations that are corrected for Hb variants; for example, some studies have used HPLC methods excluding the fraction of Hb variants [78]. The HLC-723 G8 HbA1c analyzer (Tosoh Bioscience, Inc., Tokyo, Japan) has two versions, Variant Mode (G8vr) and Standard Mode (G8st). In the G8vr, Hb variants are detected, but the turnaround time is long, whereas in the G8st, the turnaround time is short, but Hb variants may go undetected. We evaluated the basic performance of the HLC-723 G11 Variant Mode (G11vr; Tosoh Bioscience), recently introduced in Korea, which is based on the ion-exchange HPLC method, and evaluated its usefulness for HbA1c assays in the case of Hb variants.
METHODS
Instruments
We evaluated the basic performance of the G11vr. For correlation evaluation, we used G8vr, HLC-723 G11 Standard Mode (G11st, Tosoh Bioscience) and G8st. For comparison with the discordant results between G11vr and G8vr, we used the Cobas Integra 800 immunoassay (Roche Diagnostics, Basel, Switzerland). For comparison with the reference method, HPLC-MS, we used liquid chromatography (Shimadzu Nexera X2 UPLC; Shimadzu Co., Kyoto, Japan) and MS (AB Sciex 6500 Triple Quad, AB Sciex, Framingham, MA, USA). CE was performed using a Sebia Capillarys 2 Flex Piercing Hemoglobin(E) kit (Sebia, Lisse, France).
Sample collection
This study was conducted at Samsung Medical Center, a tertiary-care hospital in Seoul, Korea, and was approved by its Institutional Review Board (IRB No. 2016-12-134). Regardless of age, sex, and underlying diseases, samples submitted for routine HbA1c test between Dec 2016 to May 2017 were included in this study for method comparison. Each sample was stored at −70℃ until analysis.
A total of 208 samples were collected, and samples were divided into two groups using the G8vr: 108 flagged and 100 non-flagged samples. Flags indicate unusual chromatogram patterns, including low total chromatogram area, low HbA1c concentrations (<4%), high HbF concentrations (≥5%), abnormal peaks in the HbA1c fraction, the presence of unknown peaks, peaks not detected, and peaks with the possible presence of Hb variants. Of the 108 flagged samples, 52 had flags associated with abnormal peaks in the HbA1c fraction, the presence of unknown peaks, or peaks related to the possible presence of Hb variants. In addition, 15 samples with known Hb variants were provided by Seoul National University Bundang Hospital, Seongnam, Korea, to confirm the HbA1c concentrations by HPLC-MS.
Precision
Precision was assessed using high- and low-concentration quality control substances for HbA1c, which were provided by the manufacturer, according to the Clinical and Laboratory Standards Institute (CLSI) EP05-A3 guidelines [9]. Repeatability and within-laboratory precision values (% CV) were assessed twice daily for 20 days at both low and high concentrations. Each test value was determined as the mean value of the two measurements.
Linearity
Linearity was evaluated according to the CLSI EP06-A guidelines [10]. High- and low-concentration control materials that were close to the upper and lower limits of the measurement range (18.59% and 3.64%, respectively) were used. Linearity was evaluated at mixture ratios of 4:0, 3:1, 2:2, 1:3, and 0:4. The test was repeated four times for each of the five concentrations, and linearity was evaluated on the basis of the coefficient of determination (R2).
Comparison
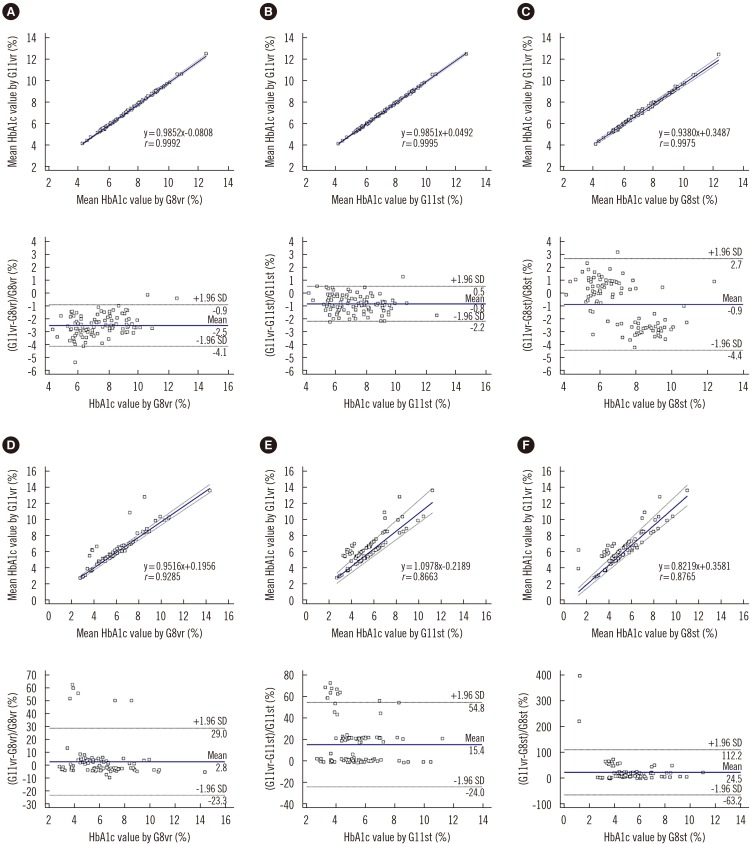
The comparison study was conducted according to the CLSI EP09-A3 guidelines [11]. For each of the 108 flagged and 100 non-flagged samples, we compared the G11vr with G8vr, G11st, and G8st, by calculating correlation coefficients (r) and the percentage difference between the results of the respective analyzers.
To evaluate HbA1c measurement in the presence of Hb variants, the 15 samples with known Hb variants were measured with each analyzer. We also measured HbA1c concentrations using both HPLC-MS and CE in these 15 samples.
Turnaround time
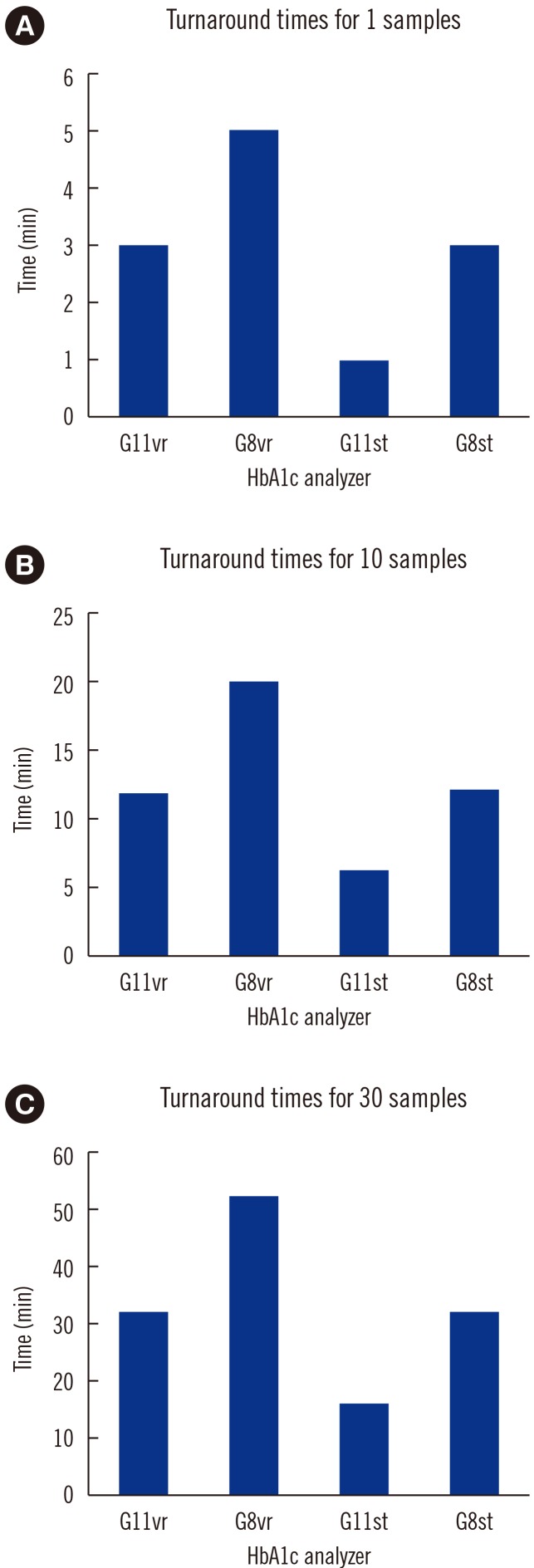
We recorded the time required to test one sample, 10 samples, and 30 samples, for the G11vr, G8vr, G11st, and G8st. Turnaround time means the testing time from mounting the samples to reporting the results. No flagged sample was included in this analysis.
Carry-over effect
To evaluate the carry-over effect for the G11vr, low- and high-concentration patient samples were selected and were measured four times, starting with the high-concentration samples (16.0%, H1–H4). After measuring the low-concentration samples four times (4.6%, L1–L4), the carry-over ratio was calculated using the following equation:
Statistical analysis
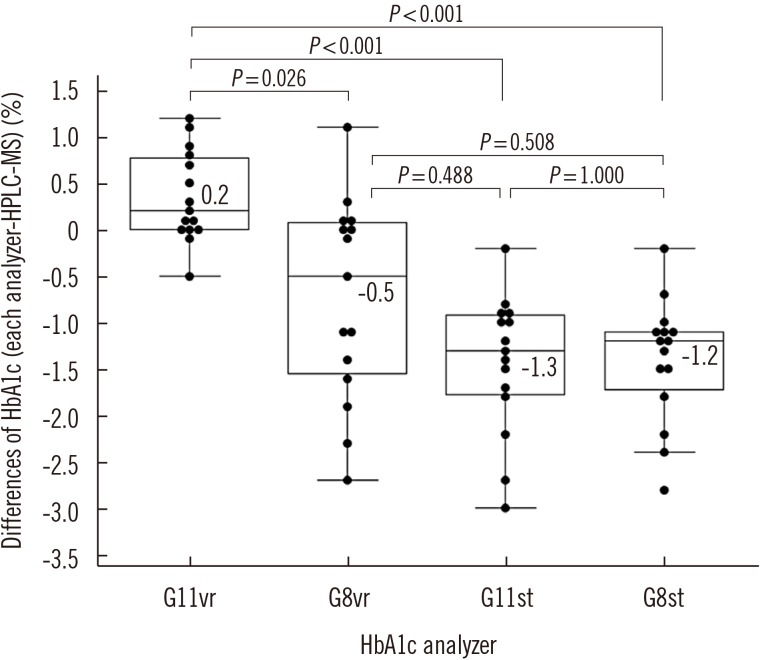
We used MedCalc (version 11.5, MedCalc Software, Mariakerke, Belgium) and R ver. 3.5.1 for statistical analysis. We also drew box-and-whiskers plots to show medians and interquartile ranges for the differences between each analyzer and HPLC-MS results of the 15 additional samples. Each P value was calculated using the Wilcoxon rank-sum test. P<0.05 was considered significant.
RESULTS
Precision
Repeatability (% CV) in measuring low- and high-concentration controls was 0.57% and 0.35%, respectively. Within-laboratory precision was 0.86% and 0.69%, respectively.
Comparison
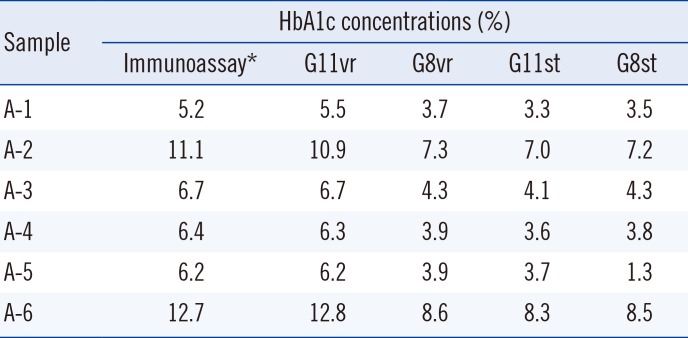
Fig. 1 shows the correlations between analyzers for flagged and non-flagged samples. When we used immunoassays to reanalyze the six samples (A-1 to A-6) with the most discordant results between G11vr and G8vr (% difference >30%), the G11vr results were more similar to those of the immunoassay than to those of the G8vr (Table 1).
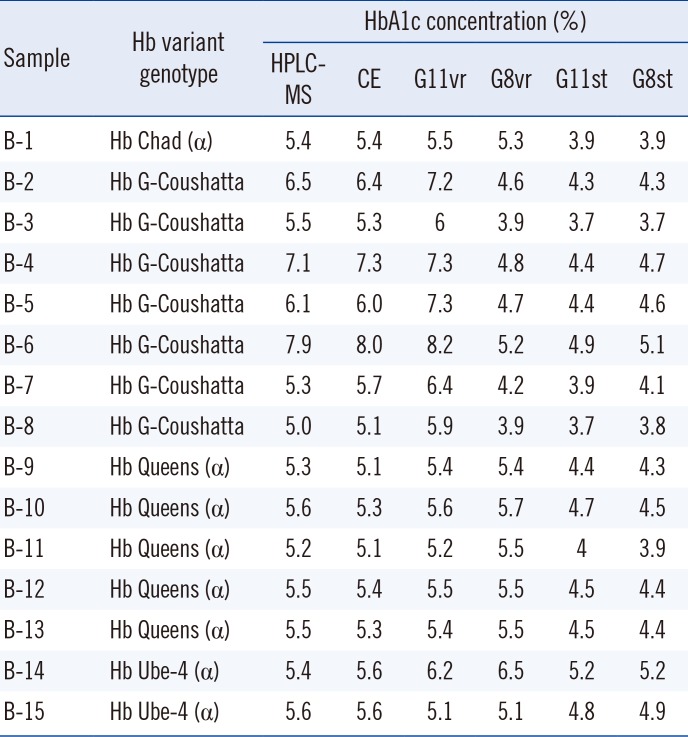
HbA1c concentrations for eight of the 15 additional samples (B-1 to B-15) were higher when measured with G11vr than with the other analyzers (Table 2). The differences in HbA1c results between G11vr and HPLC-MS were significantly smaller than the differences between the other analyzers and HPLC-MS (Fig. 2). The HbA1c results of HPLC-MS and CE were similar. Three representative chromatograms of the 15 additional samples are shown in Fig. 3.
DISCUSSION
Differences in results between methods can be due to interfering factors (e.g., bilirubin, triglyceride, cholesterol, and drugs) or variation related to the measurement of HbA1c concentration in the presence of other members of the Hb family (HbF, Hb variants) [12]. The usefulness of ion-exchange HPLC for measuring HbA1c concentration in the presence of Hb variants is limited [13]. We focused on the ability of the G11vr to measure Hb variants as well as its basic performance. The repeatability and within-laboratory precision of this analyzer were excellent, within 1%, at both high and low concentrations. The linearity of R2 was also excellent; it was as high as 0.9999. Regarding the comparison test, the correlations between analyzers were weaker for flagged samples than for non-flagged samples (the latter having r values over 0.997). Of the flagged samples, the six with the greatest differences between G11vr and G8vr were all with flags indicating potential Hb variants by G11vr. When we re-analyzed the samples by immunoassay, the results were similar to those of G11vr.
HPLC analyzers have the advantages of great precision and a visually identifiable chromatogram, but the disadvantage of interference by various hemoglobinopathies, HbF, and carbamylated Hb. An advantage of immunoassays is that they are not affected by HbE, HbD, or carbamylated Hb; however, they can be affected by hemoglobinopathies with altered amino acids on binding sites or by HbF [14]. To compare the influence of Hb variants, we measured HbA1c concentrations in 15 samples with known Hb variants. HbA1c concentrations on G11vr were more similar than those of other analyzers to HbA1c concentrations measured using HPLC-MS or CE. The seven samples for which Hb concentrations were higher in G11vr than in G8vr all contained Hb G-Coushatta variants. This variant is most commonly found in Koreans [15], and samples with Hb G-Coushatta show significant negative bias on G8vr [16]. The differences between the G11vr and G8vr results can be explained by the fact that the G11vr separates the abnormal peak better (Fig. 3) and that HbA1c concentration was calculated after excluding the variant peak area. G11 is an upgrade of G8—the software was upgraded from v. 5.24 to v. 3.01—in which the issue of interference with HbE is reduced. The Hb G-Coushatta peak is eluted at a similar retention time as that of HbE in HPLC analyzers, and reduced interference with Hb G-Coushatta on G11vr was expected. Thus, G11vr seems to reduce the probability of misdiagnosis of diabetes because there is no negative bias against Hb G-Coushatta.
The performance of HPLC analyzers in the presence of interference by unusual Hb variants (Hb Yamagata, Hb G-Hi's-Tsou, etc.) needs to be further investigated. When comparing G11vr and G11st, G11vr tended to produce higher concentrations, and most of the results that showed similar values between the G11vr and the G11st were detected with flags unrelated to Hb variants (HbA1c <4%, Hb-F ≥5%, low total area). Most of the samples that showed a higher value on G11vr than on G11st were those, in which G11vr detected Hb variants, whereas G11st did not. The fact that some samples have higher HbA1c concentrations on G11vr than on G8vr, along with the better correlation with immunoassay and HPLC-MS, suggests that the G11vr provides more accurate HbA1c results than the G8vr in the presence of Hb variants. Thus, we expect that use of G11vr will improve the diagnosis of diabetes in patients with Hb variants.
With regard to turnaround time of the four analyzers, when the sample preparation time (two minutes) was not taken into account, G11vr required less time than G8vr to test one sample (1 vs 1.6 minutes) but the same as that for G8st, which is widely used in Korea. G11st is twice as fast as G11vr. Variant analyzers that are currently used are disadvantageous compared with standard analyzers; thus, standard analyzers have been the mainstay in many Korean laboratories. We showed that the turnaround time for G11vr is similar to that for the existing G8st, and thus, G11vr seems to overcome this limitation.
In the past year at our hospital, reported HbA1c concentrations were lower in patients with Hb variants. Hence, we replaced all HbA1c analyzers with G8vr to improve Hb variant detection; since the replacement, a considerable number of patients with Hb variants have been identified. Until recently, Hb variants were thought to be uncommon in Koreans and thus, we did not consider it necessary to detect Hb variants and correct HbA1c concentrations. However, as more than two million foreigners reside in Korea, [17] Hb variants are expected to be observed at increasing concentrations, and a variant-mode HPLC analyzer would be a requisite for accurate measurement of HbA1c concentrations in foreigners. Although the reference interval of HbA1c is 4–6% as suggested by the manufacturer, testing the recent American Diabetes Association (ADA) cut-offs for diagnosis of diabetes and for risk assessment of vascular complications would be useful [18].
A limitation of this study is that we described the HbA1c concentration unit as a percentage, as is currently in use, and did not convert values into SI units (mmol/mol) as per IFCC, which is globally recommended. There are several reasons for using the percentage. In Korea, most laboratories report HbA1c in %, and clinicians also use % as a common unit, according to the National Glycohemoglobin Standardization Program. Raw data from the G11vr is also displayed in % (Fig. 3), and the recent College of American Pathologists (CAP) survey also reported % as the HbA1c unit. Since there are still many documents primarily using % as the HbA1c concentration unit [1920212223], we decided to report HbA1c concentration as %.
In conclusion, G11vr showed excellent precision and linearity, and minimal carry-over effect in HbA1c measurement, as well as fast turnaround time. G11vr would be clinically useful, as it has the advantages of detecting Hb variants and correcting HbA1c measurements to values consistent with the immunoassay, HPLC-MS, and CE results, compared with existing standard analyzers.

 XML Download
XML Download