

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urinary tract infection (UTI) is a common bacterial infection in infants, with an incidence of 2% during the first two years of life [1]. Infants with UTI are more likely than the older children to have significant morbidity and acute pyelonephritis (APN). Infants have non-specific symptoms such as fever and irritability and are less able to communicate their symptoms, leading to potential delays in diagnosis. Infants have a higher incidence of sequelae after APN than older children, suggesting an age-related risk [23]. Thus, early and accurate detection of APN is a primary goal, especially in infants with febrile UTI.
In clinical practice, symptoms along with acute-phase inflammatory markers such as white blood cell (WBC) count, erythrocyte sedimentation rate, C-reactive protein (CRP), and procalcitonin have been used to detect cortical defects [45]. However, when used alone, these inflammatory markers may not accurately reflect cortical defects (CD) owing to their non-specific nature [6]. Tc-99m dimercaptosuccinic acid (DMSA) renal scintigraphy is considered optimal for the detection of renal parenchymal involvement or scarring in UTI [7]. However, this invasive method requires sedation and exposure to radiation. Therefore, a more practical method is needed to determine renal parenchymal involvement.
Evolving biomarkers have been studied for non-invasive detection of APN in children with UTI [891011]. Although several studies have revealed promising results for neutrophil gelatinase-associated lipocalin (NGAL) in children with UTI [91011], only limited data are available for infants [1213]. This study aimed to assess whether plasma NGAL (pNGAL) could be used as a reliable marker for renal parenchymal involvement and to determine the appropriate diagnostic cut-off value of NGAL for detection of renal parenchymal involvement in infants with febrile UTI.
METHODS
1. Study design and infant selection
This retrospective study was conducted at a single tertiary center (Chonnam National University Hospital, Gwangju, Korea) between January 2015 and July 2016. Hospitalized infants under 12 months of age and who had febrile UTI were enrolled. Exclusion criteria were as follows: (1) underlying disease, (2) previous febrile UTI, and (3) delayed blood sampling after administration of antibiotics. UTI was defined as an abnormal urinalysis result and a positive urine culture (≥5×104 colony forming units/mL) according to the American Academy of Pediatrics guidelines [14]. The infants were divided into two groups based on the presence or absence of CD on DMSA scintigraphy. Of the 64 infants enrolled, 43 (67.2%) had CD (UTI-CD) and 21 (32.8%) had no CD (UTI-ND). The median age was 4.0 months; 41 were males and 23 were females. Medical records were reviewed for data such as age, sex, urine culture results, and laboratory and radiological parameters. The study was approved by the Institutional Review Board of Chonnam National University Hospital (CNUH-2017-124), Gwangju, Korea and followed the Declaration of Helsinki.
2. Laboratory and radiological investigations
Blood samples for WBC, CRP, and pNGAL and urine samples were obtained on admission before third generation cephalosporin therapy. Blood (5 mL) was collected by vein puncture in Vacutainer K3 EDTA Tubes (Becton-Dickinson and Co., Franklin Lakes, NJ, USA) and Vacutainer Plus Plastic Serum Tubes. WBC count was determined with UniCel DxH 800 (Beckman Coulter, Brea, CA) using the impedance method, and immunoturbidimetric assay of CRP was carried out with Olympus AU5800 autoanalyzer (Olympus Co., Tokyo, Japan). pNGAL concentration was measured using a commercial kit (in 2015, Triage NGAL test; Alere, San Diego, CA, USA; since 2016, NGAL ELISA kit; BioPorto Diagnostics, Gentofte, Denmark). NGAL concentrations were expressed as ng/mL. The measurable range of NGAL is 15–1,300 ng/mL by Triage NGAL test and 25–3,000 ng/mL by NGAL ELISA kit. Inter- and intra-assay CVs of the assays were, 13.5% and 11% for the Triage test, respectively, and 5% for the NGAL ELISA kit. Urine (approximately 10 mL) was collected using a catheter, and automated dipstick urinalysis was carried out (CLINITEK Novus Analyzer, Siemens, Erlangen, Germany). All infants were evaluated by ultrasound (US) and DMSA scintigraphy to identify any anatomical abnormalities and the presence of renal parenchymal involvement, respectively. DMSA scintigraphy was performed 2–3 hours following the IV injection of 99m-technetium-DMSA (Tecnescan, Mallinckrodt Diagnostica, Netherlands) using a dose of 50 µCi (1.85 MBq)/kg (minimum dose 500 µCi). DMSA scintigraphy was repeated six months later in children with renal CD. Voiding cystourethrography was conducted in children with any abnormal findings on US or DMSA scintigraphy to check the vesicoureteral reflux. The severity of vesicoureteral reflux was classified according to the International Reflux Study Committee classification [15].
3. Statistical analysis
Categorical data were summarized as counts and percentages, and continuous data were summarized as median values with interquartile range (IQR). Continuous data were analyzed using the Student's t-test or Mann–Whitney U test as appropriate, and categorical data were analyzed using the chi-square test. Logistic regression was used to assess predictors of CD. As NGAL and CRP data were not normally distributed, log-transformed data was used for logistic regression. In the primary analysis, univariate analysis was used to identify the association between CD and the following factors: age, sex, hydronephrosis, WBC count, MPV, log CRP, and log pNGAL concentrations. We included all significant variables in a multivariate model. ROC curve analysis was performed, and the area under the curve (AUC) was calculated to identify the best predictive cut-off values for WBC, CRP, and pNGAL for the detection of CD. The sensitivity and specificity for the best cut-off values were calculated. P<0.05 was considered statistically significant. All analyses were performed with SPSS ver. 21.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Baseline and clinical characteristics
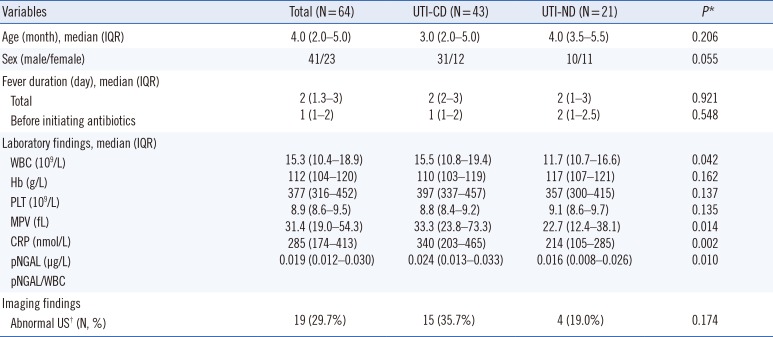
The characteristics and laboratory data of the UTI-CD and UTI-ND groups are summarized in Table 1. There were no significant differences in sex, median age, duration of fever, and US abnormalities between the groups (Table 1). A total of 38 infants underwent VCUG (33 in UTI-CD and five in UTI-ND). Ten (30.3%) of the infants in the UTI-CD group and two (40%) of the infants in the UTI-ND group had vesicoureteral reflux, but this percentage did not significantly differ between the two groups (Table 1).
2. Biomarkers
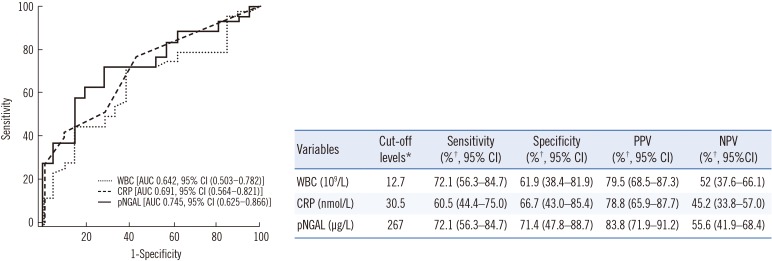
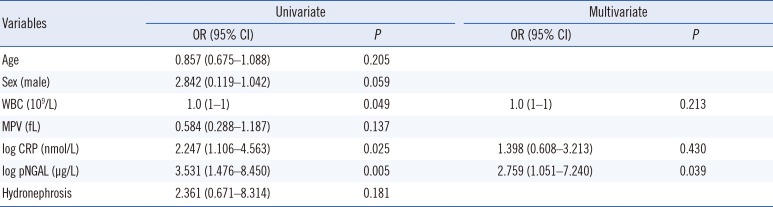
WBC, CRP, and pNGAL values were significantly higher in the UTI-CD group than in the UTI-ND group. Univariate analysis showed that elevated WBC count (P=0.049), log CRP level (P=0.025), and log pNGAL concentration (P=0.005) were related to the presence of CD (Table 2). Multivariate analysis showed that log pNGAL concentration was the only independent predictor of CD (odds ratio [OR] 2.759, P=0.039). ROC curve analysis showed that pNGAL had the highest AUC of 0.745 (95% CI, 0.561–0.821, P=0.014), followed by 0.691 for CRP (95% CI, 0.561–0.821, P=0.014), and 0.642 for WBC (95% CI, 0.503–0.782, P=0.066) (Fig. 1). pNGAL showed fair predictive accuracy for CD. According to the ROC curve analysis, the appropriate cut-off values for WBC, CRP and pNGAL were 12.7×109/L, 30.5 nmol/L, and 267 µg/L, respectively. pNGAL showed the highest sensitivity (72.1%), specificity (71.4%), positive predictive value (PPV) (83.8%), and negative predictive value (NPV) (55.6%) for CD (Fig. 1 and Table 2).
DISCUSSION
The present study revealed that pNGAL concentrations were significantly higher in UTI-CD group than in UTI-ND group. Compared with WBC count and CRP, pNGAL had the highest AUC and the highest sensitivity, specificity, PPV, and NPV. pNGAL concentration was the only independent predictor of CD. These results suggest that pNGAL could be a useful marker for the detection of CD in infants with febrile UTI.
UTI is a common bacterial infection in infants and children, with approximately 1% of boys and 1–3% of girls developing a UTI during childhood [16]. APN, which refers to infection of the renal parenchyma, may cause chronic renal damage. Renal scarring may lead to hypertension, renal insufficiency, and end-stage renal failure. In clinical practice, some inflammatory markers have been used to detect infection of the renal parenchyma, but these markers may not accurately reflect the CD [616].
According to several clinical studies, NGAL is an excellent marker for the detection and monitoring of acute kidney injury [17] and is an emerging biomarker for the diagnosis of UTI [1218]. Recently, NGAL has been proposed as a marker of CD in UTI [11]. Several studies have analyzed data on children, but limited data are available for infants [13], and the diagnostic value of NGAL for the prediction of CD in infants with UTI is unclear. Two pediatric UTI studies reported optimal cut-off levels for pNGAL to be 102.5 µg/L [11] and 117 µg/L, respectively [19], for the prediction of APN. In our study, the optimal cut-off level was 267 µg/L in infants with febrile UTI. Furthermore, the UTI-ND group also showed high levels of pNGAL (mean: 204.9 µg/L) compared with pediatric UTI groups in previous studies [1119]. No international studies have been conducted to date to accurately evaluate the reference values of NGAL measurement in blood or urine samples based on large population surveys, stratified according to age, gender, and ethnicity [20]. Stejskal et al [21] reported a median pNGAL concentration of 78.8 ng/mL in men and of 80.0 ng/mL in women in healthy white individuals [21]. The pNGAL levels for the detection of acute renal injury in adult patients range from 150 to 400 ng/mL [22]. However, there is no established reference value for NGAL in infants. According to a previous study, the distribution of urine NGAL (uNGAL) values in pediatric-age patients approximates a log-normal distribution, with values being higher in neonates than in children [23]. During acute bacterial infection, the optimal cut-off value of pNGAL was 217 µg/L in older children and 247 µg/L in young children (below the age of two years) [24]. Of note, in this study, high concentrations of pNGAL were observed in infants compared with children with UTI. The reason for this observation remains unknown. Previously reported cut-off values for NGAL did not allow accurate prediction of the presence of parenchymal involvement in infants with febrile UTI in this study (using a cut-off of 102.5 µg/L [11]: sensitivity, 93% and specificity, 24%; and a cut-off of 117 µg/L [19]: sensitivity, 88% and specificity, 38%). On the other hand, our cut-off value for NGAL (267 µg/L) showed a sensitivity of 72% and a specificity of 71.4% in detecting CD.
NGAL can be tested in both blood and urine. These two forms of NGAL have distinct mechanisms of induction and upregulation, allowing for different applications in clinical settings [9]. pNGAL has been reported to be a useful predictor of systemic inflammation associated with pyelonephritis and damage [111319], while uNGAL is also a potentially useful marker for the detection of subclinical renal damage such as scarring, vesicoureteral reflux, or obstruction [9252627]. In UTI, NGAL production by neutrophils may increase the actual NGAL concentration. As NGAL may be released from neutrophils during the preparation of serum, it may be preferable to use plasma [20]. In the present study, we used plasma samples and corrected the pNGAL values to the WBC counts. Our study revealed the potential of pNGAL as a sensitive and useful marker for early prediction of parenchymal involvement.
Our study has some limitations. First, given the relatively small sample size, our results should be interpreted with caution. Second, pNGAL was measured only at admission, thus, time-series data were not available. Third, the assay method for NGAL measurement was changed from the Triage NGAL test to the ELISA kit, and the assay method may affect the measured levels; however, no significant differences were observed in our study. Fourth, the cut-off value in our study was higher than that used in previous studies. This may be due to differences in enrollment criteria; further studies should be based on a larger population.
In conclusion, rapid screening of pNGAL at admission provides valuable information for the detection of parenchymal involvement for the prediction of the clinical course in infants with acute febrile UTI.
 XML Download
XML Download