

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Refractory thrombocytopenia (RT), classified by the WHO as a subtype of refractory cytopenia with unilineage dysplasia, is an unusual MDS subtype that initially presents as chronic pure thrombocytopenia [1]. RT is often misdiagnosed as idiopathic thrombocytopenic purpura (ITP) becausethe dysplasiain ITP is indistinguishable from that in RT [2].
Cytogenetic abnormalities associated with RT include del(20q), +8, and abnormalities of 5 and/or 7 [3]. RT with chromosome 5 abnormality should be differentiated from MDS with isolated del(5q) (5q-syndrome). Because the prognoses and treatments for RT, ITP, and 5q-syndrome are very different, the accurate diagnosis of patients presenting with thrombocytopenia or chromosomal abnormalities is essential. Here, we report a patient with RT, harboring a 5q deletion.
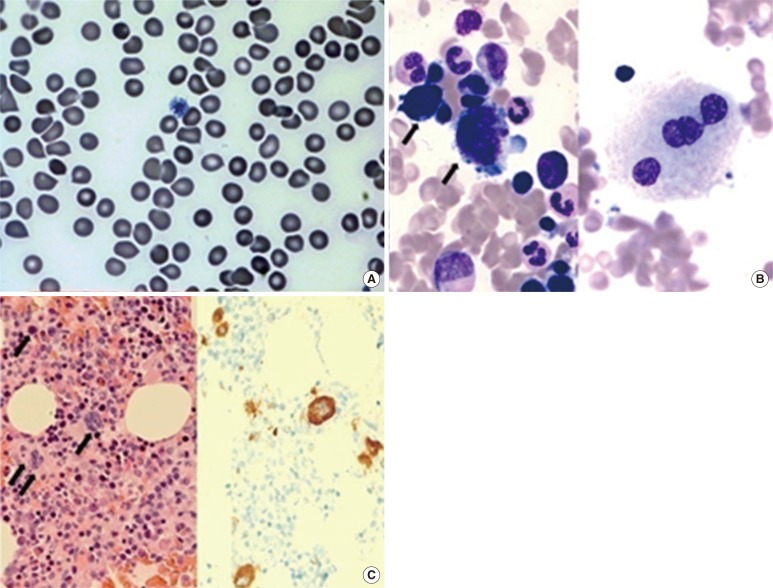
A 55-yr old Korean woman was admitted to our hospital in April 2012 because of a low platelet count. She had no symptoms and had not been taking any drugs. She had no past history of any hematologic diseases or medications. Neither hepatosplenomegaly nor lymphadenopathy was found on physical examination. A complete blood count (CBC) showed the following: platelet count, 44×109/L; mean platelet volume (MPV), 14.2 fL; platelet distribution width, 21.5%; hemoglobin, 13.9 g/dL; white blood cell count, 5.7×109/L; and mean corpuscular volume, 91.1 fL. White blood cell differential was normal. A peripheral blood smear confirmed low platelet count with the presence of giant platelets (Fig. 1A). A CBC was performed every month for 10 months, commencing on the first visit after the last treatment; however, the platelet count remained low. In February 2013, we performed a bone marrow (BM) study with cytogenetic analysis. The BM aspirate revealed that more than 10% of megakaryocytes showed dysmegakaryopoiesis (Fig. 1B). The BM biopsy showed 45% cellularity and no fibrosis. The number of megakaryocytes in the BM clot section was markedly increased showing dysmegakaryopoiesis, which was confirmed by using CD61 immunohistochemical staining (Fig. 1C).
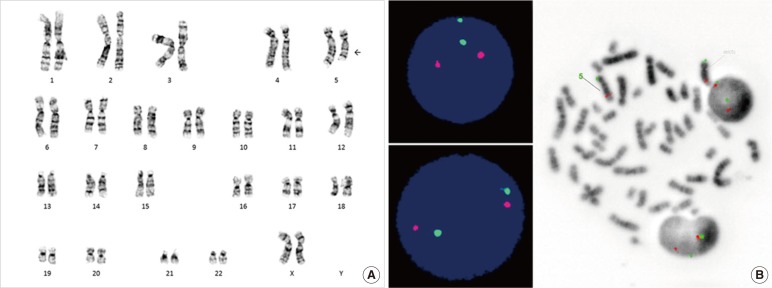
Because she had no previous diseases related to thrombocytopenia, we ruled out secondary thrombocytopenia. We initially suspected ITP because of the low platelet count and increased megakaryopoiesis; however, the chromosomal analysis revealed an abnormal karyotype,46,XX,del(5)(q15q31)[5]/46,XX[15] (Fig. 2A). This effectively ruled out ITP and we considered a diagnosis of 5q-syndrome, which is characterized by del(5q), macrocytic anemia, and normal or elevated platelet count [4]. However, the patient had normal hemoglobin levels, normocytic red blood cells, and thrombocytopenia. Interphase and metaphase FISH, using a Vysis EGR1 FISH probe kit (Abbott,Des Plaines,IL, USA), revealed no EGR1 deletion (Fig. 2B). Finally, the patient was diagnosed as having RT according to the WHO classification (2008) [1], and splenectomy is now being considered.
RT is a type of MDS with clonal characteristics, whereas ITP is a benign nonclonal hematologic disease caused by autoantibodies [2]. The two different diseases share many common features including megakaryocytic hyperplasia and dysmegakaryopoiesis [5]. Therefore, patients with RT are often misdiagnosed as having ITP [6]. However, it is important to distinguish RT from ITP because the treatments and prognoses are very different. Cytogenetic tests are very helpful when differentiating between the two diseases. If cytogenetic abnormalities are found, then the patient does not have ITP. According to a previous study, the proportion of abnormal karyotypes in refractory anemia patients is approximately 50% [7], but the proportion of abnormal karyotypesin RT patients is not well established because the incidence of RT is very low.
In 5q-syndrome, thrombocytosis is common, whereas thrombocytopenia is not [4]. However, the present patient showed thrombocytopenia. Therefore, the patient could not have had 5q-syndrome. Cytogenetic abnormality in 5q-syndrome is an interstitial deletion of chromosome 5, and the loss of function of the tumor suppressor genes EGR1 and CTNNA1 in 5q32 is possibly responsible [1, 8]. In this case, EGR1 was intact, which was shown by EGR1 FISH. A previous study on the analysis of RT karyotypic abnormalities reported that abnormalities in chromosomes 3 and 5 are common. In that study, del(5q) was also found in a patients with RT and, to the best of our knowledge, it was the only reported case of a RT patient presenting with del(5q). Unlike our case, the deleted region included 5q31 [5].
In conclusion, more studies are required to increase our understanding of RT. Cytogenetic analysis is very helpful in differentiating RT from ITP. However, even when cytogenetic tests reveal an abnormal karyotype, further tests could be needed for the correct diagnosis.
 XML Download
XML Download