

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pallister–Killian syndrome (PKS) (Online Mendelian Inheritance in Man #601803) is a rare genetic disorder characterized by craniofacial dysmorphisms including a prominent forehead with sparse frontotemporal hair and a wide range of developmental delays, intellectual disability, hypotonia, seizures, skin pigmentation, and other systemic anomalies [1]. PKS is diagnosed by the presence of tetrasomy 12p, which consists of additional short arms of chromosome 12. The additional short arms are usually detected as isochromosomes of 12p with tissue-limited mosaicism [2], which is rarely found in peripheral blood; therefore, the diagnosis usually requires analysis of cultured fibroblasts [3]. Array-based comparative genomic hybridization (array CGH) may enable detection of copy number variations using DNA isolated from an uncultured tissue sample. This method has improved molecular diagnostic detection of clinically significant chromosomal aberrations.
In this study, we identified three patients with mosaic tetrasomy 12p. There have been a few case reports in Korea, in which all patients were detected by chromosome or FISH analysis. To our knowledge, these are the first reported cases of PKS detected by array CGH in Korea. The first two patients were initially identified by array CGH, and the other patient was diagnosed with FISH analysis alone. The genetic study was performed with the written informed consent of the parents. This study was exempted from approval by institutional review board of the hospital.
CASE REPORT
1. Patient 1
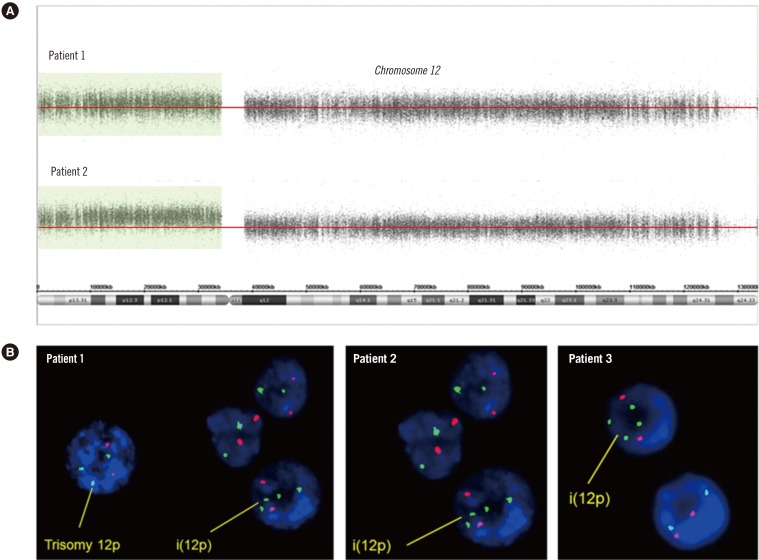
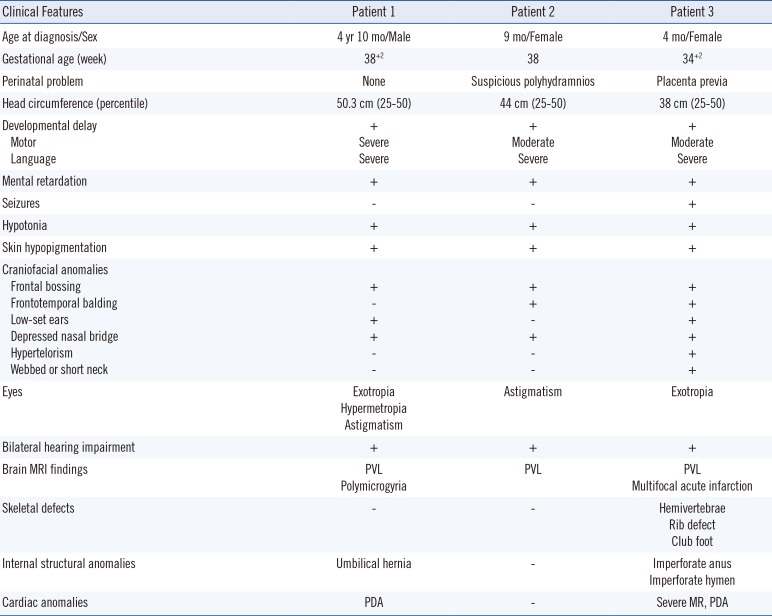
A 4-yr-old boy presented with a developmental delay with a large hypopigmented macule on his face. Chromosome analysis of peripheral lymphocytes revealed karyotype 46,XY. Array CGH was performed by using the Affymetrix Cytogenetics 2.7M Array (Affymetrix; Santa Clara, CA, USA) with DNA extracted from peripheral lymphocytes, which identified two to three copies of chromosome 12p. This finding was suggestive of chimerism between trisomy 12p and tetrasomy 12p (Fig. 1A). FISH analysis by means of ETV6 (TEL)/RUNX1 (AML1) Extra signal dual color probe (Abbott Molecular Inc., Des Plaines, IL, USA) was performed on cultured peripheral lymphocytes according to the manufacturer's instructions. This assay revealed that 2.3% and 3.5% of the cells were positive for trisomy 12p and tetrasomy 12p, respectively (Fig. 1B).
3. Patient 3
A 4-month-old female infant was referred due to multiple congenital anomalies with a hypopigmented macule. Chromosomal analysis revealed 46,XX. To confirm the suspected clinical features, FISH analysis was conducted to identify possible additional copies of chromosome 12. Approximately 11% of the cells showed tetrasomy 12p (Fig. 1B).
DISCUSSION
PKS is a rare chromosomal disorder with characteristic features that change with the patient's age [4]. Craniofacial abnormalities are prevalent in most patients. Nearly 90% of patients have ophthalmologic abnormalities, and over 75% have a hypopigmented skin lesion and hearing loss [5]. Our cases had the common dysmorphic facial features such as frontal bossing, a depressed nasal bridge, frontotemporal balding, and abnormal skin pigmentation. The patients presented here are similar to those reported in other studies.
Different tissues are known to show variable presence or absence of isochromosome 12p, i(12p) [6]. The level of mosaicism varies depending on the gestational age or tissue-specific mosaicism [6]. The patients described in this report initially had normal chromosomal results on cultured peripheral lymphocytes.
We identified three patients with mosaic tetrasomy 12p. To our knowledge, these are the first reported cases of PKS detected by array CGH in Korea. The first two patients were initially identified by array CGH, and the other patient was diagnosed with FISH analysis alone. It is likely that FISH analysis is sufficient for identifying PKS because FISH confirmed the presence of mosaicism in the three patients presented here. In the prenatal and perinatal periods, however, the clinical characteristics of PKS are not prominent. Therefore, conventional chromosomal analyses may yield normal results at these ages, necessitating array CGH for definitive diagnosis.
Mosaicism in the supernumerary metacentric isochromosome 12p is often detected in skin fibroblasts although the karyotype of cultured lymphocytes appears normal. There seems to be a higher success rate of detecting mosaicism in cultured skin fibroblasts than in peripheral blood because abnormal cells have a lower attrition rate than T lymphocytes do [67]. Furthermore, cell culture may select against abnormal cells. Phytohemagglutinin is often used in chromosomal analysis to stimulate T lymphocytes to divide. If abnormal cells are less competitive than are normal cells in stem cell populations, then they may be underrepresented in stimulated cultures [89]. Therefore, cells with isochromosome 12p are likely to be selected against during cell culture [10]. Ballif et al [11] found that the percentage of abnormal cells among phytohemagglutinin-stimulated cells is lower than that observed in uncultured cells when FISH is used for analysis. This finding suggests that there is a chromosome-or chromosomal-region-specific growth bias in cell culture. Furthermore, a rapid decline of abnormal clones [with i(12p)] was discovered during amniocyte subculture [12], and the death of these abnormal cells has been suggested as the cause of tissue-limited mosaicism in PKS [13]. Low-level mosaicism of chromosomal abnormalities with clinical significance can be overlooked when masked by a high proportion of normal cells or by culturing bias that is necessary for conventional cytogenetic testing [11]. Wilkens et al [5] reviewed the existing literature and stated that peripheral lymphocytes show a higher percentage of cells with a healthy karyotype and a lower percentage of i(12p) mosaicism. The correct diagnosis has probably been overlooked in a number of patients because skin fibroblasts were not routinely included in karyotyping in the past [1415].
Array CGH is useful for patients who have suspected clinical and/or constitutional abnormalities. This method can rapidly screen genomes at an unprecedented resolution and has dramatically improved the molecular diagnostic detection of clinically significant chromosomal aberrations [1617]. Array CGH has several advantages over FISH. The former using extracted DNA, does not require cell culture, which can introduce culturing bias [10]. In addition, cells in all cell cycle phases can be analyzed simultaneously [18]. However, array CGH of unstimulated peripheral lymphocytes has failed to detect all cases of PKS because it can detect mosaic abnormal cells at prevalence not lower than 10-20% [1011]. Analysis of skin fibroblasts [19] or buccal smears [20] has been proposed as a diagnostic gold standard, but this notion is still controversial. Hodge et al [19] proposed that a skin biopsy sample should continue to be the diagnostic gold standard for PKS because of the variable and insufficient quality of buccal smears. Nonetheless, Cobben et al [20] showed that in patients with suspected PKS, array CGH or FISH analysis of buccal smear cells seems to be the first diagnostic choice because these two methods are reliable, rapid, and noninvasive. Cobben et al [20] recommended a skin biopsy only if buccal-smear analysis cannot detect i(12p).
PKS is a rare multisystem disorder that is difficult to diagnose prenatally and in early infancy. The diagnosis of PKS can be made by physical examination if characteristic dysmorphic features and global developmental delay are present. Array CGH can be used to diagnose PKS in early infancy and during the prenatal period. Clinicians can also employ FISH analysis to diagnose this disorder in patients with visible PKS features.

 XML Download
XML Download