

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Retinoblastoma is the most common intraocular tumor in children [1]. As the long-term survival rate and eyeball salvage rate of retinoblastoma have increased, attention has begun to focus on treatment that preserves vision [1-4]. Chemotherapy plus local treatments have nearly replaced external beam radiotherapy (EBRT) in order to avoid the serious side effects including secondary malignancy and ocular and orbital complications [5-7]. Because the visual potential of treated retinoblastoma depends on the location of the tumor [3], the relationship between macular involvement and visual prognosis may be an issue. However, studies on the visual prognoses of patients with macular retinoblastoma are insufficient and controversial. The reported visual acuities of the eyes after treatment for macular tumors vary from 20/20 to no light perception [8-11]. Desjardins et al. [12] reported that all eyes with macular retinoblastoma treated with chemotherapy plus local treatments had an acuity of 20/200 or less. Recently, Schefler et al. [13] reported that 57% of macular retinoblastoma eyes treated with chemotherapy and repetitive foveal laser ablation retained 20/80 or better vision. We conducted a retrospective study to evaluate the visual outcomes of retinoblastoma in the posterior pole (RBPP) treated with chemotherapy plus local treatments. Additionally, we addressed the prognostic factors that influence visual outcomes.
Materials and Methods
All patients with RBPP diagnosed at the Department of Pediatric Ophthalmology, Seoul National University Children's Hospital between August 1987 and September 2007 were reviewed retrospectively. Only patients treated with primary chemotherapy with local treatments such as laser photocoagulation or thermotherapy were included. The posterior pole was defined as the area within the major vascular arcades, and any tumor partially or entirely within the posterior pole at diagnosis was considered as RBPP. Representative fundus photographs of the RBPP are shown in Fig. 1. Patients who underwent radiotherapy during the disease course were excluded.
The first-line chemotherapy regimen consisted of a combination of cisplatin, etoposide, adriamycin, and cyclophosphamide. Thirteen cycles of chemotherapy were administered at monthly intervals. The chemotherapy regimens and cycles were altered in consideration of drug side effects such as infection, renal dysfunction and tumor responsiveness.
Diode laser photocoagulation and thermotherapy were performed for local control of RBPP. Diode laser photocoagulation was used for posterior pole tumors with base sizes of five or fewer disc diameters (DD). Thermotherapy was used for posterior pole tumors with base sizes of ten or fewer DD. Diode laser photocoagulation and thermotherapy were not applied at the fovea in order to avoid treatment-related visual loss.
During the aforementioned period, 154 patients were diagnosed with retinoblastoma associated with a posterior pole mass. Twenty-three eyes in 19 patients eventually experienced successful tumor control and eyeball preservation via primary chemotherapy plus local treatments. Ten eyes in seven of these patients were unable to be measured for visual acuity due to young age (< 3 years) or developmental delay; these patients were excluded from the final analysis. Ultimately, a total of 13 eyes in 12 patients were included in this study.
The variables recorded for each eye included age at diagnosis and at the final follow-up, gender, duration of follow-up, Reese-Ellsworth classification and International Classification of Retinoblastoma at diagnosis, presence of foveal involvement, tumor area in the posterior pole, type of regression pattern and best corrected visual acuity (BCVA) at the final follow-up.
In cases of multiple masses, only masses located in the posterior pole were considered. Evaluations of the presence of foveal involvement and tumors area in the posterior pole were performed both before and after treatment to account for tumor shrinkage and scar extension caused by the treatment. Tumor area in the posterior pole was measured as affected percentage of posterior pole. Post-treatment evaluation was performed based on residua including scar changes. The regression patterns were classified as type 0 (no visible residua), type I (fully or almost fully calcific residua), type II (fleshy tissue with little or no calcification), type III (mixed calcific and fleshy), or type IV (atrophic chorioretinal flat scar) according to the methods used in a previous study [14]. All measurements of visual acuity were performed using a standardized Snellen chart. Thereafter, the Snellen visual acuities were converted into a logarithmic minimum angle of resolution equivalent for statistical analysis.
The eyes were divided into subgroups of probable visual prognostic factors including presence of foveal involvement, tumor area in the posterior pole, and type of regression pattern. We expected foveal involvement and tumor area in the posterior pole to be strong probable prognostic factors. The guideline of the International Classification of Retinoblastoma can be used as a visual prognostic factor for tumor location and size, but it does not sufficiently consider foveal involvement or tumor area in the posterior pole. Thus, we investigated these two factors in patients with RBPP.
The mean final BCVA and the distribution of final BCVA were compared between subgroups of probable visual prognostic factors. The presence of foveal involvement was classified into two groups: 1) group F (fovea) + represented the positive foveal involvement and 2) group F-represented negative foveal involvement. Tumor area in the posterior pole was also classified into two groups: 1) group L (large) represented patients with tumor greater than one-half the area of the posterior pole and 2) group S (small) represented patients with tumor less than one-half the area of the posterior pole. The representative fundus photographs of the RBPP according to this classification are shown in Fig. 1. The types of regression patterns were classified according to the aforementioned criteria. Final BCVAs were classified into three groups for comparison of the distribution of final BCVA: 1) group 1 (good visual acuity) represented visual acuities of 20/50 or better, 2) group 2 (fair visual acuity) represented visual acuities of 20/200 or better, but less than 20/50, and 3) group 3 (poor visual acuity) represented visual acuities less than 20/200. To analyze the influence of tumor area in the posterior pole on final BCVA, only eyes with foveal involvement were included. SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Statistical significance was assigned at p < 0.05.
Results
The mean age at diagnosis was 9.3 ± 7.4 months (mean ± SD) for four male patients and eight female patients. The mean follow-up period was 79.3 ± 29.3 months, and the mean age at the final follow-up was 87.1 ± 32.5 months. Two eyes (15.4%) were classified as Reese-Ellsworth classification group I, nine eyes (69.2%) were classified into group II, two eyes (15.4%) as group III, and no eyes were classified as Reese-Ellsworth group IV or V. All eyes were classified as International Classification of Retinoblastoma group B. All patients underwent primary chemotherapy; seven also underwent laser photocoagulation, while two underwent accompanying thermotherapy. The presence of foveal involvement and tumor area in the posterior pole were not affected by treatments. The mean final BCVA of treated RBPP was 20/210 (range, hand motion to 20/16). However, eight eyes (61.5%) had an acuity of 20/200 or better and seven eyes (53.8%) had an acuity of 20/50 or better.
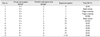
All data regarding the probable risk factors and final BCVA are listed in Table 1. The only factor found to significantly correlate with visual outcome was the presence of foveal involvement. Mean final BCVA was significantly better in group F- (five eyes) than in group F+ (eight eyes), with averages of 20/26 (range, 20/50 to 20/16) in group F- and 20/778 (range, hand motion to 20/25) in group F+ (p = 0.006). All eyes in group F- had an acuity of 20/50 or better, whereas only four eyes (37.5%) in group F+ had an acuity of 20/200 or better, as shown in Fig. 2. The representative fundus photographs are presented according to the foveal involvement and visual outcome in Fig. 3.
Other probable prognostic factors were not significantly correlated with visual outcome. Mean final BCVA was better in group S (1 eye) than in group L (7 eyes), with averages of 20/25 and 20/1,262 (range, hand motion to 20/50), respectively. However, this result was not statistically significant due to the small number of cases in group S (p = 0.250). Two eyes (28.6%) in group L had an acuity of 20/200 or better, despite foveal involvement and large tumors in the posterior pole, as presented in Fig. 4.
Mean final BCVA was not significantly different according to type of regression. However, eyes with type IV regression patterns tended to have a better final BCVA compared to those of other types in the final BCVA distribution, as shown in Fig. 5A. According to the data presented in Fig. 5B, eyes with type IV regression patterns tended to have less frequent foveal involvement and smaller tumor area in the posterior pole.
Discussion
Several recent treatment advances have led to increased eyeball salvage rates in the treatment of retinoblastoma. Chemotherapy plus local treatments resulted in nearly 100% treatment success in eyes with R-E groups I to IV and avoiding EBRT or enucleation [4]. Thus, the attention paid to the visual outcomes of treated retinoblastoma has increased. Migdal [10] reported that 50% of bilateral retinoblastoma cases had a final visual acuity of 6/12 or better in one eye, and Holbek and Ehlers [15] reported that 54% of retinoblastoma patients in their study had an acuity of better than 6/12 after treatment with EBRT.
Several authors have presented counterintuitive cases of patients with macular tumors and surprisingly good vision [9,11,16,17]. The results of previous retrospective studies on visual outcomes of treated macular retinoblastoma vary according to the definition of macula. Hall et al. [8] reported a strong association between tumor location and visual outcome; however, they simultaneously reported that 33% of treated macular tumors (defined as a tumor within 1.5 DD of the fovea) had an acuity of 20/40 or better. Desjardins et al. [12] also reported a strong association between tumor location and visual outcome, although all eyes with maculopathy due to retinoblastoma had a post-treatment acuity of 20/200 or less [12]. Schefler et al. [13] reported that 57% of macular retinoblastomas (defined as tumors within the vascular arcades) treated with planned chemotherapy and repetitive foveal laser ablation had an acuity of 20/80 or better. In our study, the mean final BCVA of RBPP treated with chemotherapy plus local treatments was not excellent, but 61.5% of eyes with RBPP had an acuity of 20/200 or better and 53.8% had an acuity of 20/50 or better.
In our study, the presence of foveal involvement was a strong prognostic factor for visual outcome. Schefler et al. [13] reported that all tumors outside the fovea had an acuity of 20/40 or better, whereas all tumors in the fovea had an acuity of 20/60 or worse. As previously mentioned, Desjardins et al. [12] also reported that all eyes with maculopathy caused by retinoblastoma had a post-treatment acuity of 20/200 or less. However, in our study, four eyes (36.4%) with RBPP with positive foveal involvement had an acuity of 20/200 or better. This result suggests the treated RBPP can have working vision, although RBPP involving fovea.
Another logical assumption is that a large tumor assures a poor visual prognosis, and a small tumor assures a good visual prognosis. However, we could not demonstrate differences in final BCVA according to the tumor area in posterior pole because of the small number of cases. Further studies are needed that evaluate the influence of tumor size on final visual outcome.
Regression patterns have changed as chemotherapy has replaced EBRT as the treatment of choice for retinoblastoma. Singh et al. [14] reported the distribution of regression patterns of retinoblastoma treated with EBRT to be 18% for type 0 tumors, 50% for type I, 17% for type II, and 14% for type III; their report contained no comment on type IV regression patterns. Shields et al. [18,19] reported the distribution of regression patterns of retinoblastoma treated with chemotherapy to be 2% to 3% for type 0 tumors, 10% to 13% for type I, 3% to 5% for type II, 23% to 33% for type III, and 51% to 57% for type IV tumors. In our study, the distribution of the regression patterns was similar to those documented in previous studies examining patients treated with chemotherapy. The relationship between the regression pattern and the final visual outcome was not evaluated in previous studies. In our study, we were unable to demonstrate a significant difference in mean final BCVA according to the type of regression pattern due to the small numbers of cases. However, the eyes with type IV regression patterns tended to have better final BCVAs. This result is paradoxical because the type IV regression pattern indicates projected sclera for the atrophic choroid and retina. However, in previous studies, the regression pattern was associated with tumor size and location [14,18,19]. For instance, Shields et al. [19] reported that the factors predictive of type IV regression patterns were smaller tumor base and greater distance from the foveola. These features were also observed in our study. The relatively good visual outcomes of the type 4 regression patterns may be due to these features.
In our study, foveal involvement and tumor area in posterior pole were not changed by treatments. However, in some cases, a large fusiform-shaped RBPP that hid the fovea at the initial examination and without foveal involvement at the tumor base decreased after treatment. This finding suggests that large RBPPs hiding the fovea at initial examination can shrink after treatment and preserve the fovea. Therefore, we must consider the possibility of vision preservation in cases of RBPP, even though large RBPPs may obscure most of the posterior pole.
There are several limitations to the present study. First, the sample size was small, as we had to exclude many patients for which we had no visual acuity scores due to young age, developmental delays, or primary enucleation. Second, our study included eyes with multiple tumors, although only RBPP was considered in these cases. However, tumor regrowth, seedings, tractional or serous retinal detachments and retinal pigment epithelial atrophy surrounding the tumor can affect the central vision even if the tumor is outside of the posterior pole. Third, visual outcomes were assessed only according to central visual acuity. Other analyses of visual function, such as a contrast-sensitivity test or a visual field test, could also be used. Further studies taking these above issues into account are needed.
Retinoblastoma patients now have an excellent prognosis, both for survival and eyeball preservation. Although visual prognosis is strongly correlated with the presence of foveal involvement, the visual outcomes of RBPP cannot be easily predicted. Thus, the possibility of preserving vision should be considered before making treatment decisions. Additionally, active efforts to improve visual function in retinoblastoma must be taken into account, such as via occlusion therapy and through close follow-up of visual acuity [20].





 XML Download
XML Download