

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Arachnoid cysts are benign, non-neoplastic and extra-axial lesions; most of them are clinically silent and unchanged in size. In previous studies112131524), the incidence of arachnoid cysts has been estimated to range between 0.3% to 1.7%. However, the advanced neuroimaging techniques have facilitated the diagnosis of arachnoid cysts, which, in turn, has led to an increase in the number of patients2121415).
In some cases, an arachnoid cyst arouses symptoms and its clinical presentations vary according to the size and location of the cyst. The most frequent symptom is headache, which is caused by the local mass effect, increased intracranial pressure (ICP), and/or hydrocephalus15). Above this, seizures, cognitive dysfunction, developmental delay, and intracranial hemorrhage can be also presented.
In this report, we describe a case where a patient with a posterior fossa arachnoid cyst complained of visual field defect, visual disturbance, and mild headache; no ataxia and unsteady gait were reported. The patient's visual symptoms rapidly deteriorated in a week and, consequently, the patient's vision got worse.
CASE REPORT
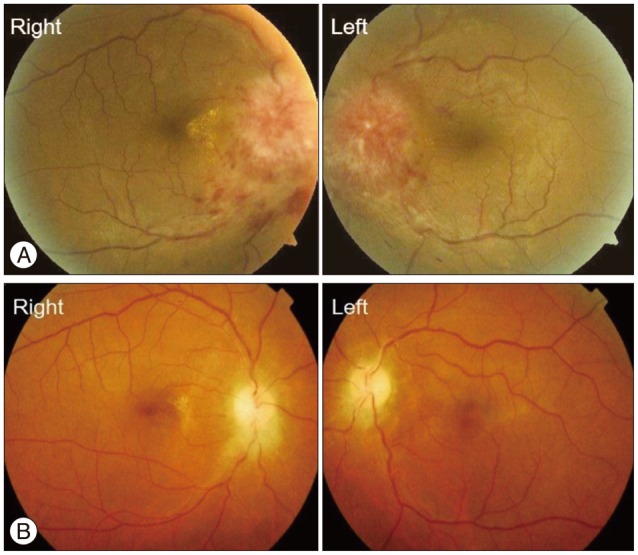
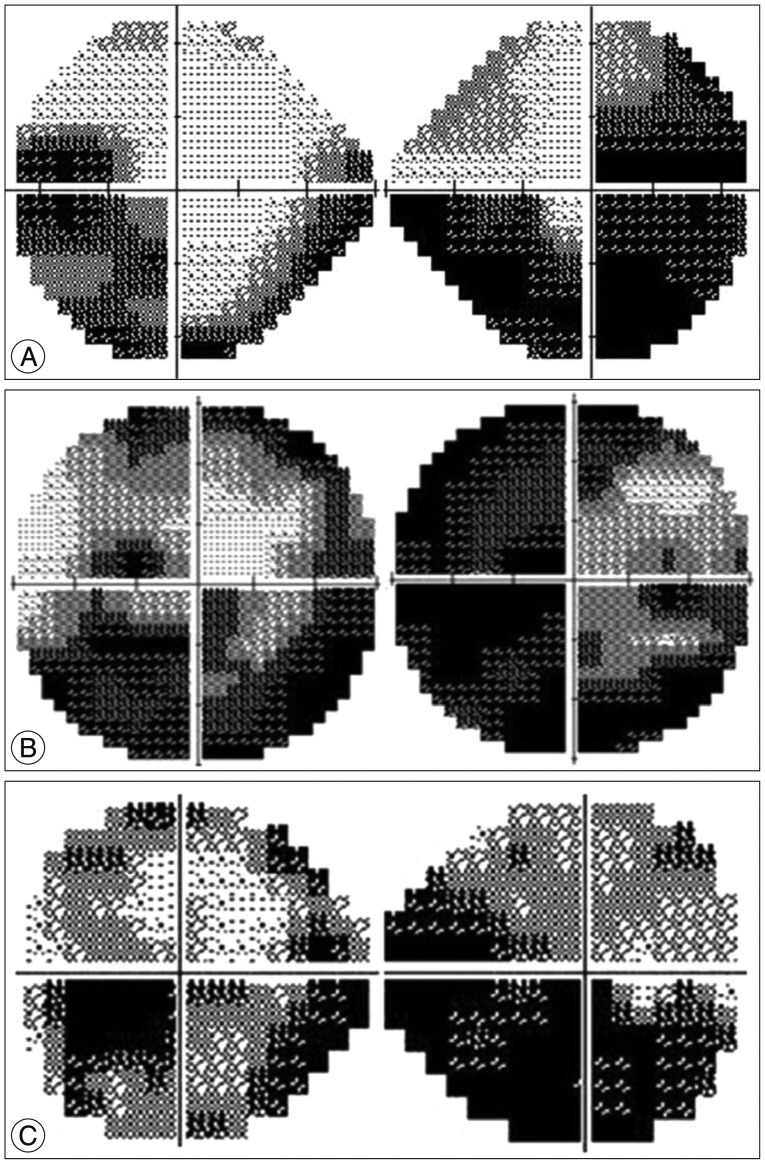
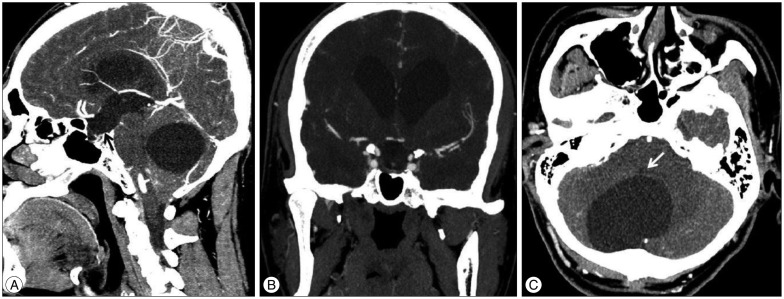
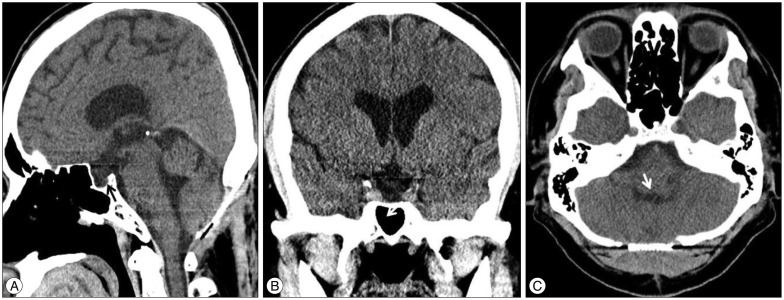
A 39-year-old male patient presented at our emergency room after a traffic accident and the brain computed tomography (CT) scan indicated an incidental arachnoid cyst on posterior fossa. At that time, the patient complained only of facial abrasions and the left knee pain, but not of headache or visual disturbance. In eight months, however, he revisited our Department of Ophthalmology to check the decreased visual acuity, visual field defect, and headache. On the ophthalmologic examination, bilateral papilledema (Fig. 1A), decreased visual acuity, and visual field defect (Fig. 2A) were found. After the transfer to the Department of Neurosurgery, we rechecked brain CT scans (Fig. 3). The diameter of the patient's arachnoid cyst did not change compared to the previous CT scans; however, the slightly enlarged third ventricle was compressing the optic chiasm and the suprasellar area. Since visual complications were expected, we recommended an emergency operation. However, the patient refused the operation for personal reasons. One week later, he came back to the hospital with nearly complete visual loss. His right eye was completely blind, whereas his left eye recognized only light (Fig. 2B).
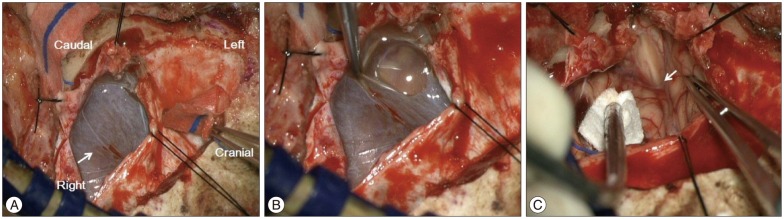
On that day, he underwent an emergency operation. A conventional suboccipital craniectomy was performed on the patient lying on the operating table in the prone position. After the dural incision, the arachnoid cyst was exposed and cystic fluid was expelled. Arachnoid membrane was carefully dissected and the arachnoid cyst was fenestrated to cisterna magna for connecting with the cerebrospinal fluid (CSF) flows. Arachnoid membrane which covering the foramen of magendie was also fenestrated and the CSF flows was running properly (Fig. 4). Excluding the brain tumor, the collected membrane was sent to the pathologic laboratory. In high power field microscopy under the hematoxylin and eosin stain, the cystic membrane was composed by membranous fibrocollagenous tissues without tumor cells. Finally, the patient was diagnosed as arachnoid cyst (Fig. 5).
One week afterwards, we checked the brain CT scans and the removal of the cyst and the decreased ventricle size were confirmed. On the ophthalmologic examination, the papilledema and visual field were slightly improved; however, the patient's visual acuity did not improve. Upon the tenth day after the operation, the patient was discharged and, during the next one month, he was subject to the steroid therapy.
In five months after the operation, papilledema (Fig. 1B), headache, and radiological images (Fig. 6) quickly returned to the normal ranges. Nevertheless, visual acuity and visual field improved slowly and slightly (Fig. 2C). The blind right eye improved to recognize the light and the blurred left eye improved to acknowledge the silhouette of an object; thus, it did not fully recovered to the prior, normal condition.
DISCUSSION
Arachnoid cysts are benign, non-neoplastic and extra-axial lesions. Their prevalence has been reported to amount to approximately 1% of all intracranial mass lesions112152430); however, advanced neuroimaging techniques and the widespread use of CT and MRI imaging have led to an even higher incidence of report of these lesions1249121619203031). One recent study, Al-Holou et al.1), reviewed 48417 brain images and identified 661 (1.4%) arachnoid cysts. This report found that the prevalence of arachnoid cyst in children was 2.6%, slightly higher than in adults, and men (1.8%) have a high prevalence than women (1.1%). The most common locations were middle fossa (34%), retrocerebellar (33%), and cerebral convexity (14%)124). Despite the increased identification of arachnoid cysts, the natural history and mechanism of enlargement has not been well defined1131524).
Most arachnoid cysts are asymptomatic and are found incidentally in most cases1112429). Nevertheless, when arachnoid cysts give rise to any symptom, headache is the most common complaint. This symptom is caused by the local mass effect and hydrocephalus. In addition to headache, gait imbalance, seizure, and visual changes can also be presented according to the location and size of the arachnoid cyst. If clinical symptoms develop, surgical interventions are recommended3615162122232728). Various operation techniques, such as cyst excision1517), stereotactic aspiration1825), endoscopic cyst fenestration512), ventriculocystostomy26), and cystoperitoneal shunt810152728), have been introduced and the main purpose of such operations is similar, namely, a direct decompression of the arachnoid cyst or making the connection between the cyst and the CSF flows for spontaneous resolution.
Generally, visual symptoms occur in the patients with suprasellar arachnoid cysts, because the arachnoid cyst is adjacent to the optic nerves7). The patients with posterior fossa arachnoid cysts usually do not complain of visual symptoms, as the cyst is not adjacent to the optic nerves. However, a posterior fossa arachnoid cyst can indirectly disrupt the CSF flows and, in turn, the disruption increases the whole ventricle size and the ICP. In our case, the enlarged third ventricle was compressing the optic chiasm with cephalocaudal direction on the CT scan (Fig. 3A, B). The compressed superior part of optic chiasm led to the defect of inferior visual field (Fig. 2). In addition, visual acuity was affected by the papilledema, which was caused by the increased ICP. Consequently, both visual acuity and visual field were influenced by the posterior fossa arachnoid cyst.
When the patient first visited our Department of Ophthalmology, his visual symptoms and headache were not severe and the patient could walk and drive. Besides, the brain CT scan showed no changes as compared to previous CT scans, so we could not predict a risk of rapid deterioration. The patient's refusal to have an operation and the surgeon's wrong prediction delayed the appropriate on-time treatment; ultimately, the patient's vision was severely damaged during the critical seven days. After the operation, the patient's visual acuity, visual field, and papilledema were slightly improved; however, we regard that the patient's vision will unfortunately not fully recover.
CONCLUSION
Unlike gait disturbance and ataxia, visual symptoms do not frequently occur in the patients with posterior fossa arachnoid cysts; this is so because the cyst is located away from the optic nerves. However, the disruption of CSF flows can indirectly induce visual symptoms and these symptoms can rapidly deteriorate.
Considering the results of our case, it should be emphasized that the patients with posterior fossa arachnoid cysts could develop a rapid neurologic deterioration. Furthermore, the aggravation pace of the symptoms can be neither estimated nor predicted. Therefore, in the event of the development of symptoms, an early intervention or close observation are crucial.

 XML Download
XML Download