

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Manipulation of the cervical spine during endotracheal intubation and surgery has the potential to cause serious spinal cord injuries. Cervical spine fractures are a serious complication of maxillofacial trauma, because of the high potential for mortality and neurological morbidity [1]. The atlas and axis support the pivot motion of the neck. Injury to the upper cervical vertebrae (C1 to C4) usually presents with difficulty to breathe or talk, inability to control bladder bowel function, and paraplegia or quadriplegia if there is injury to the spinal cord, which may be fatal [23]. Early treatment includes stabilization of the neck, to prevent further damage, and the regulation of respiration. Long term treatment includes corticosteroid injections, analgesics, and surgery to reduce pressure on the spinal cord. Injuries to the lower third of the face are more commonly associated with damage to the upper cervical spine [1]. Maxillofacial trauma can have concomitant cervical spine or spinal cord injury [14]. In 1961, Carpenter was the first to describe an association between cervical spine fractures and vertebral artery injuries (VAI) [5]. VAIs may result from cervical spine trauma and have the potential to cause cerebral, brainstem, and even spinal cord ischemia [67]. Long term complications may take place over days to years following vertebral artery injuries and include arteriovenous fistula, late hemorrhage, pseudo aneurysm, thrombo embolic episodes, cerebral ischemia, vertigo, and death [67]. Treatment options include observation, anti-platelet agents, and endovascular treatments. The early diagnosis and prompt introduction of anticoagulants reduce ischemic neurologic events and their associated disabilities [678]. The absence of neurologic symptoms in patients with cervical spine fracture does not preclude vertebral artery injuries [8]. VAI symptoms are due to ischemia of the cerebellum, brainstem, and the primary visual cortex and include headache, neck pain, disturbance of speech, sensory and gait disturbance, impairment of vision, vertigo, nausea, vomiting, and altered consciousness [9].
CASE REPORT
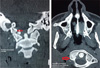
An 18-year-old male (height 155 cm and weight 51 kg) was accidentally hit by an unfastened crane hook and suffered serious injuries to the right side of his neck and jaw. He presented to the hospital emergency room with severe neck pain, bleeding from the mouth, and a deep lacerated injury on the right side of his jaw and upper part of the neck, with surgical emphysema (Fig. 1). His Glasgow Coma Scale (GCS) score was E4V5M5, and his pupils were bilaterally equal and 2 mm in size. His initial recorded vital signs were: blood pressure of 96/60 mmHg, heart rate of 100 beats/min, respiratory rate of 18/min, and SpO2 of 93% in room air. A computerized tomography (CT) scan of his facial bones and upper cervical spine revealed a comminuted displaced fracture, which involved the angle and body of the right hemimandible, with adjacent soft tissue laceration, hematoma, and air pockets (Fig. 2). There was a displaced comminuted fracture of the right transverse process of the atlas that extended into the right lateral mass, and a fracture of the right occipital condyle that extended to the foramen transversarium margin (Fig. 3). The atlas was rotated, with displacement of the atlanto-occipital and atlanto axial joints. A magnetic resonance image (MRI) scan of neck showed the absence of right vertebral artery flow void and a thrombus in the right vertebral artery (Fig. 4). Bilateral vertebral artery Doppler was performed, which showed right vertebral artery flow stasis, indicating a thrombus. The nasal bones, nasal cavity, nasopharynx, and laryngeal cartilages were normal. There was no intracranial injury and no involvement of the spinal cord; hence, no sensory motor deficits or bladder or bowel involvement were identified. A thin pre-vertebral hematoma was seen extending from level C1 to C4, and the rest of the cervical vertebrae were normal. Since the inner cortex of the mandible was comminuted and shattered, the right inferior alveolar artery was cut completely, with bleeding into the oral cavity. Mouth opening was restricted, and the inter incisor distance was 1 cm.
After the neck wound was covered with dressing, a cervical collar was applied. The patient was admitted to the high dependency unit (HDU); and after proper explanation of the anesthetic and surgical plan to the patient and his guardian, he underwent an open reduction and internal fixation of the mandible and exploration of the neck injury the next day. His basal oxygen saturation was at 95%, and an arterial blood gas analysis in room air revealed a pH of 7.36, PaCO2 of 40 mmHg, PaO2 of 110 mmHg, bicarbonate level of 22 mmol/L, and arterial oxygen saturation of 98%. His blood investigations revealed hemoglobin levels of 11.9 gm%, platelets of 2.04 lakhs/mm3, serum urea of 22.0 mg/dL, serum creatinine of 0.6 mg/dL, serum glucose of 93 mg/dL, sodium of 140 meq/dL, and potassium of 3.9 meq/dL. A large bore intravenous cannula was inserted into the dorsum of the left hand, and ringer lactate was started. He was connected to a multipara monitor that displayed his electrocardiogram (ECG), noninvasive arterial pressure, pulse oximetry, endtidal carbon dioxide (ETCO2) and core temperature. The ECG showed a sinus rhythm, with a heart rate of 92/min and a normal axis, blood pressure of 110/65 mmHg and respiratory rate of 14/min. Glycopyrrolate (0.2 mg) was given intravenously. An awake fiber-optic nasotracheal intubation was planned, with a backup emergency surgical airway kit in case the first method failed. The nasal cavity was anesthetized by packing with cotton tape gauze soaked in 2% lidocaine and 0.05% oxymetazoline hydrochloride, and the oropharynx was nebulized with 2% lidocaine spray. The larynx and trachea were anaesthetized by nebulization with lignocaine, and supplemental oxygen was administered via a nasal catheter. A 5.5 mm fiber-optic bronchoscope was taken, and a 7.0 mm size cuffed reinforced endotracheal tube was slid up the full length of the shaft and gently secured to the beveled end of the bronchoscope.
The oral cavity was full of clots as the right inferior alveolar artery was cut. The oral cavity was intermittently cleared, to enable clear visualization. The fiber-optic bronchoscope was introduced into the left nasal cavity and gently advanced through the glottis into the trachea to just above the carina. Then, the endotracheal tube was gently railroaded and advanced into the trachea. Successful placement of the tube in the trachea was verified by capnography and bilateral equal air entry. The cuff was inflated to seal the airway, and the tube was securely fixed. Fentanyl (50 µg, 1 µg/kg), propofol (80 mg), and atracurium (25 mg) were given intravenously. A throat pack was inserted gently through the available inter incisor space. Anesthesia was maintained using a mixture of 50% oxygen, 50% nitrous oxide, and 1–1.5% isoflurane, with intermittent doses of atracurium. Intermittent positive pressure ventilation was instituted, and ETCO2 was maintained at 35 mm Hg. The perioperative period was uneventful, without significant changes in blood pressure or heart rate (systolic pressure 110–130 mmHg, diastolic pressure 70–86 mmHg, heart rate 85–108 beats/min). The mean arterial pressure (MAP) was maintained between 90 to 100 mmHg to maintain perfusion and reduce the risk of posterior circulation ischemia. A total of 1000 mL of crystalloids was given perioperatively. At the end of the procedure, which lasted 90 minutes, neuromuscular blockade was reversed with neostigmine (2.5 mg) and glycopyrrolate (0.4 mg), which were given intravenously. The throat pack was removed and the trachea was extubated when the patient was awake with protective airway reflexes, and the neuromuscular transmission recovered to a train of four (TOF) ratio of 0.9. Paracetamol (1,000 mg) was given intravenously for postoperative analgesia, and ondansetron (4 mg) was given intravenously for antiemetic prophylaxis. The patient was transferred to the HDU for observation, and he made an uneventful recovery and was started on IV antibiotics and enoxaparin for anticoagulation, 48 hours following surgery for one week, to establish vertebral artery flow. This was later replaced with oral aspirin. The neurosurgical intervention included cervical immobilization using a cervical collar brace for 12 weeks, to achieve spinal stabilization and prevent further nerve damage, including injury to the brain stem.
DISCUSSION
With any maxillofacial trauma, injury to the cervical spine and VAI should be suspected even if the patient is asymptomatic. Most cases of VAI are asymptomatic and can be missed. In particular, non-dominant unilateral VAI is compensated by adequate collateral circulation to the basilar system through the contralateral vessel and the posterior inferior cerebellar arteries. Clinical symptoms related to vertebrobasilar ischemia include vertigo, nystagmus, dysphagia ,dysarthria, diplopia, blurred vision, and altered consciousness [9]. In our case, the patient did not have any cerebral involvement due to left vertebral artery dominance, collateral circulation from the opposite vertebral artery, and carotid circulation through the posterior communicating arteries. He did not have any neurological involvement symptoms except for pain in the neck. The use of awake fiber-optic nasotracheal intubation after topical anesthesia of the airway prevented further neck manipulation and was the only choice, as his mouth opening was grossly restricted. A backup surgical tracheostomy kit was kept ready, in case of failure to establish the airway. Hence, with any maxillofacial trauma, injury to the cervical spine and VAI should be suspected, even if the patient is asymptomatic. Systemic anticoagulation therapy is associated with improved neurologic outcomes in patients with and without stroke and prevents deterioration of neurologic statuses [10]. The prevalence of blunt VAI is approximately 0.5 to 2.0% in trauma patients and 70% in all traumatic VAI patients with cervical spine fractures [11]. Vertebral artery injuries are inherent to foramen transversarium fractures [1112], subluxations [813], and fractures of the upper cervical spine [714]. Treatment of most traumatic VAI patients involves observation or anticoagulation therapy [15]. In a few cases, endovascular interventions such as stents, coiling, or embolization are used. Anticoagulation therapy is currently recommended for patients with low bleeding risks. However, unfractionated heparin can easily normalize blood coagulation, after an interruption is recommended, and can be changed to oral anti-platelet drugs post-operatively [15]. In our case, the VAI was treated conservatively with low molecular weight heparin and oral anti-platelet drugs post-operatively. The fracture of the transverse foramen of the atlas was also managed by a cervical collar brace for 12 weeks. In conclusion, we present this case to highlight the need for extra vigilance by the anesthesiologist, to avoid neck manipulation in patients with cervical spine fractures with VAI that complicates a comminuted mandibular fracture. The anesthesiologist must be aware of the potential morbidity and mortality following VAI which can be a part of maxillofacial trauma with blunt neck injuries.



 XML Download
XML Download