

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In the field of orofacial surgery, a red blood cell transfusion (RBCT) is often needed during either double jaw or oral cancer surgery. RBCT can be a life-saving procedure for most patients with acute anemia caused by perioperative bleeding; on the contrary, it also presents various risks, such as infectious complications (viral and bacterial), transfusion-related acute lung injury, ABO and non-ABO associated hemolytic transfusion reactions, febrile non-hemolytic transfusion reactions, transfusion associated graft-versus-host disease, transfusion-associated circulatory overload, and hypersensitivity transfusion reactions, including anaphylaxis, and transfusion-related immune-modulation (TRIM) [12]. In the field of transfusion medicine, three studies have used propensity score matching with regard to transfusion and mortality namely, the ABC [3], CRIT [4], and SOAP [5] studies. The ABC and CRIT studies considered RBCT as an independent risk factor for mortality, whereas the SOAP study proved that RBCT increased the survival rate [345]. Although these results seem to contradict one another, the differences were attributed to the influence of introducing leukocyte-depleted RBCs in the SOAP study. Moreover, there are other studies involving prospective, adequately powered, randomized controlled trials that have applied restrictive and liberal transfusion strategies with respect to mortality, and more recently, a greater emphasis on restrictive strategy [678].
As shown, the research in this area remains ongoing and can be quite controversial. Accordingly, the present review aimed to summarize transfusion based on the studies that have been previously completed on this topic to date and to discuss the role of perioperative RBCT in the field of orofacial surgery.
HISTORY OF TRANSFUSION
In 1628, William Harvey, a British physician and physiologist, first presented the theory of blood circulation. While in 1665, Richard Lower, another British physician, first reported on transfusion between animals at the Royal Society. In 1667, Jean-Baptiste Denys, a French physician, transfused the blood of sheep to a 15-year-old boy for the first time and the boy survived. In 1818, James Blundell, a British obstetrician, became the first to transfuse human blood to a patient with postpartum hemorrhage. In 1840, Samuel Armstrong Lane at St George's Hospital Medical School in London used whole blood transfusion for the first time to treat hemophilia. Then in 1900, an Austrian physician and immunologist Karl Landsteiner differentiated blood agglutinins and divided them into ABO groups, and subsequently, RBC transfusions have been performed for over 100 years as a treatment modality for moderate-to-severe anemia [9].
PHYSIOLOGICAL PRINCIPLES
Oxygen transfer to the tissues in the human body involves RBCs that carry hemoglobin-bound oxygen from the lungs to the cells. Under resting conditions, the amount of oxygen supplied exceeds the oxygen demand of the tissues. This margin of safety for oxygen transport is needed for emergency situations, such as bleeding, when oxygen demand spikes rapidly; however, if excessive bleeding exceeds this safety margin, transfusion becomes necessary in order to supply enough oxygen to the peripheral vascular system and the tissues.
RBCT increases the ability to deliver oxygen to hypoxic tissues under acute anemia conditions (perioperative bleeding), as well as with diseases such as sickle cell disease or malaria. It is also responsible for carrying out a hemostatic role by increasing coagulation [10], and recent findings have indicated its involvement in clot contractions [11]. Moreover, it is also performed for the purpose of plasma volume expansion in cases of possible clinically significant perioperative bleeding.
TRANSFUSION STRATEGY & TRIGGER
The indications and triggers for RBCT are on-going issues. There have been many studies and there are still on-going studies in search of an answer. Based on studies to date, there are two strategies. Historically, the threshold that triggered a RBCT has been based on a liberal strategy (hemoglobin [Hb] level below 10 g/dL or hematocrit [Hct] below 30%). In 1988, the “10/30 Rule” was presented at the National Institutes of Health Consensus Development Conference, which presented the level of RBCT during perioperative period to be less than Hb 10 g/dL and Hct 30% and transfusions were performed based on those values for a while [12]. In 1999, a randomized, multicenter, controlled clinical trial that compared a restrictive transfusion trigger (Hb 7 g/dL) and liberal transfusion trigger (Hg 10 g/dL) in critically ill patients found that the mortality rate was lower in the group with the restrictive transfusion strategy than that of the group with the liberal transfusion strategy (22.3 % vs 28.1 %, P = 0.05) [613]. Recently, the restrictive strategy (Hb level below 7 g/dL) has become more accepted due to the accumulation of evidence regarding the negative impact on prognoses following RBCT per the liberal strategy as well as the complications and costs associated with RBCT [1415161718192021].
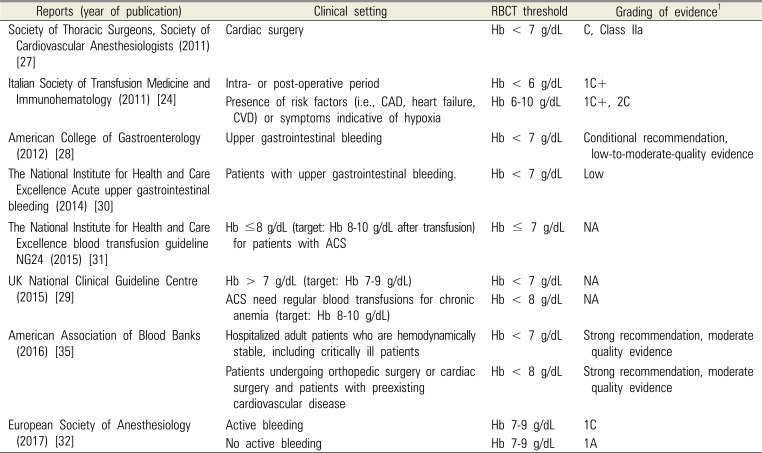
Recent reports on the guidelines for the RBCT threshold are summarized in Table 1. The American Society of Anesthesiologists sets the RBCT threshold as Hb < 6 g/dL, and for Hb between 6-10 g/dL, the decision is left up to the discretion of the anesthesiologist [222324], while the Society of Cardiovascular Anesthesiologists and several other associations has set the transfusion threshold at Hb < 7 g/dL [1325262728293031]. The European Society of Anesthesiology recommends maintaining Hb between 7-9 g/dL, regardless of perioperative bleeding [32]. The American Academy of Family Physicians has set the transfusion trigger at Hb between 7-9 g/dL for immature infants or cases involving cyanotic heart disease, severe hypoxemia, active blood loss, or hemodynamic instability [13]. The Italian Society of Transfusion Medicine and Immunohematology has set the transfusion trigger at Hb between 6-10 g/dL for cases involving coronary artery disease or cardiovascular disease [24]. The European Society of Cardiology has set the transfusion trigger at Hb of 7 g/dL when the acute coronary syndrome is present [33] and the American College of Physicians has set it at Hb between 7-8 g/dL when coronary heart disease is present [34]. Meanwhile, the UK National Clinical Guideline Centre and American Association of Blood Banks have set the transfusion trigger at Hb of 8 g/dL for cases involving cardiovascular diseases [2935].
Therefore, based on studies and guidelines up to now, it would be appropriate to set the RBC transfusion trigger at Hb of 7 g/dL, while applying the higher threshold of 8-9 g/dL for patients with cardiovascular disease or hemodynamically unstable patients. Due to recent studies, an additional issue to consider when performing RBCT has been added. Continuous noninvasive Hb (SpHb) monitoring can be helpful for determining the RBCT trigger [3637]. Another study reported that by checking the trend of the change in Hb by continuously monitoring SpHb, the amount of bleeding can be predicted and allow for a rapid response to bleeding. It is also helpful in double-jaw surgery [38].
RISK OF RBC TRANSFUSION
Although there is a clear-cut therapeutic benefit of relieving hypoxia in tissues with a RBCT, it should be performed after careful evaluation of its risks and benefits. A meta-analysis that analyzed 45 studies on the effects of RBCT on prognoses found that RBCT had a negative impact on prognoses, while two studies showed a neutral risk and one study placed more emphasis on its benefits [39]. The following are the details of each risk.
1. Infection
Interest in transfusion-transmitted infections peaked in the 1980s due to transmission of human immunodeficiency virus (HIV) and hepatitis C virus [40]. Subsequent medical advances, along with the use of serological and nucleic acid testing assays, have led to a drastic decline in the number of transfusion-transmitted infections, including HIV and the hepatitis viruses (hepatitis A, B, C) [4142]. With respect to infections, today is historically the safest time for a transfusion, but with the emergence of novel viruses, such as the recent Zika virus, transfusion-transmitted cytomegalovirus (CMV) still occurs and it remains a key issue for immunosuppressed patients [43]. Moreover, the post-transfusion infection rate may also increase due to TRIM [44].
2. Hemolytic transfusion reaction
A major potential consequence of RBCT is alloimmunization to blood group antigens. Alloimmunization can result in acute hemolytic transfusion reactions [45], potentially producing significant morbidity and mortality. One of the most important transfusion-related issues is still administrative error, which is associated with hemolytic transfusion reaction and ABO incompatibilities that lead to mortality in many cases.
3. Febrile non-hemolytic transfusion reaction
This is a more common reaction than hemolytic transfusion reaction. It is caused by cytokines within the units of red cells. Such cytokines occur when the donor red cells break up during storage or they originate from the donor leukocytes. Such reactions can be reduced by using a leukocyte filter [46].
4. Transfusion-related acute lung injury (TRALI)
Currently, TRALI is one of the most dangerous transfusion-associated complication [1]. TRALI is defined as a new acute lung injury occurring within 6 h post transfusion in patients without risk factors for acute lung injury. TRALI typically manifests as shortness of breath, fever, and hypotension [47]. Antibody-medicated TRALI (immune TRALI) is now recognized as one of the most common causes of transfusion-associated major morbidity and death in the Western world [48]. Although TRALI can occur as a result of all types of blood products, it is known to occur more commonly with plasma and pooled buffy coat-derived platelet products, rather than with RBCs (fatal TRALI incidence: plasma, 1:200,000-300,000; platelets, 1:300,000-400,000; RBCs, 1:2,500,000-2,900,000) [49]. The mechanism of TRALI has not been clearly identified, but it can be explained by the 2-hit hypothesis. Antibodies, as well as alternate substances in blood products result in neutrophil activation, which, in a susceptible patient, results in TRALI [49].
5. Hypersensitivity transfusion reaction
Hypersensitivity transfusion reaction is a very rare reaction. The biologic mechanism associated with this remains largely unknown, but patients who have had a transfusion-associated adverse reaction may have had an underlying immunodeficiency [50]. Particularly in cases transfused with blood products containing plasma, the development of anaphylaxis, a severe form of hypersensitivity, is highly associated with IgA deficiency, which appears from the production of Ig E Ab against Ig A [51].
6. Transfusion-associated circulatory overload (TACO)
Although it is called transfusion-associated circulatory overload (TACO), it is not easy to differentiate between TACO and TRALI. It is a rare complication with less than 100 articles published since its introduction during the 1990s [52]. Therefore, it is difficult to determine whether the exacerbation of pulmonary function occurred as an immunomodulation effect or due to circulatory overload [53]. Other assessments of volume overload, such as jugular venous pressure and B-natriuretic peptide (BNP) levels, can help distinguish the two [46].
7. Transfusion-related immunomodulation (TRIM)
Transfusion may trigger an immunologic reaction from the recipient antibody coming together with the donor antigen. This immunologic reaction that has a negative effect on the human immune system is referred to as “transfusion related immunomodulation (TRIM)” [54]. TRIM is a complex physiological reaction, which is mediated by residual leukocytes, apoptotic cells, and numerous biological response modifiers such as cytokines, soluble mediators, and soluble HLA peptides [55]. TRIM can be explained by two mechanisms, the first of which is HLA-dependent and directed against adaptive immunity, while the second is mild, non-specific, and directed against innate immunity [56]. Such mechanisms are related to the release of immunosuppressive prostaglandins, suppression of cytotoxic cell and monocyte activity, inhibition of interleukin-2 (IL-2) production, and an increase in regulatory T cells (Tregs) and suppressor T-cell activity [57585960].
7.1. Pathophysiology of TRIM
7.1.1. Inflammatory mediators
TRIM is associated with the following: transforming growth factor beta (TGF-β), a transfusion-related inflammatory/immunosuppressive cytokine [61]; secondary cytokines secreted by phagocytosis of apoptotic cells; and non-polar lipids and a mixture of pro-inflammatory lyso-phosphatidylcholines (lyso-PCs) contained in RBCs [62]. Lyso-PC regulates the activation of natural killer (NK) T cells and T lymphocytes [63]; induces dendritic cell maturation [64]; acts as an NK cell chemoattractant [65]; and stimulates the production of pro-inflammatory cytokines [66]. Eicosanoids such as prostaglandins, leukotrienes, and thromboxanes can accumulate in RBCs [67], and all of these inflammatory mediators may suppress immunity or aggravate tumors [68697071].
7.1.2. Residual leukocytes
There is evidence that leukocyte-containing red blood cell concentrates have negative effects, such as increased postoperative complications, associated with mortality rate [72]. Consequently, the recent trend is to use leukoreduced RBC concentrates; as a result, the risk of febrile transfusion reactions and CMV transfusion transmissions is reduced [73]. However, even after leukoreduction, a few leukocytes and cytokines may remain [7475] and can cause the secretion of IL-6, IL-10, and tumor necrosis factor alpha (TNF-α) or activation of Tregs [7677]. The activation of Tregs is antigen non-specific; it can occur due to lipopolysaccharide (LPS) and, through the Toll-like receptor-4 pathway, lead to immune suppression [78].
7.1.3. Apoptotic cells
Apoptotic cells, which are created while blood is being stored, activate and secrete TGF-β to trigger immunosuppression [6179]. Apoptotic cells express phosphatidylserine on the surface [80]. Phosphatidylserine not only induces secretion of anti-inflammatory cytokines, such as IL-10 and TGF-β, but it also suppresses secretion of inflammatory cytokines, such as IL-12, IL-1β, IL-6, and TNF [818283].
7.2. Positive effect of immunomodulation
Immunomodulation may be helpful at times, as indicated by a study result that showed a transfusion improved the survival of the kidney graft in patients who received one [84]. Moreover, among Crohn's disease patients with small bowel resection, the recurrence rate of Crohn's disease was lower in the group that received a transfusion when compared to the group that did not [85]. Therefore, when immunosuppression is required for therapeutic purposes, immunomodulation from a transfusion may be helpful.
8. Cancer risk
8.1. Cancer & immunomodulation
The American Society of Clinical Oncology/American Society of Hematology introduced transfusion as an effective treatment strategy for improving the health of cancer patients with chemotherapy-associated anemia [86]. However, numerous studies have reported that recurrence and metastasis of cancer increased following transfusion [87888990] and this is suspected to be the result of immunosuppression following allogenic RBCT [91]. Immunomodulation due to inflammatory mediators, residual leucocytes, and apoptotic cells is associated with recurrence and progression of cancer, while platelets, microparticles, and FFP are known to stimulate growth and spreading of the tumor [929394].
8.2. Cancer growth and dissemination
TGF-β suppresses NK cell activity and induces Tregs activation, in conjunction with TNF-α [88]. Moreover, in a tumor microenvironment, TGF-β contributes to the osteoclastic degeneration of the bone matrix necessary for the establishment of bone metastasis [9596]. Inflammatory mediators, such as TNF-β and lyso-PCs regulate the activation of NK cells and T cells, while also promoting the production of pro-inflammatory cytokines. [6366]. The aforementioned inflammatory mediators, residual leukocytes, and apoptotic cells induce immunomodulation by various mechanisms, which can directly or indirectly contribute to tumor growth.
8.3. Influence on cancer type
While only a few studies have reported that RBCT in colorectal cancer (CRC) cases did not have a negative effect on overall mortality, 5-year survival, recurrence, metastasis, complications, and prognosis [979899100], many studies have reported the opposite [90101102103104105106107108]. In fact, there are even reports of perioperative RBCT in CRC cases causing increased rate of infection [109110]. Even in cases that required liver resection due to metastasis of CRC to the liver, RBCT had a negative effect on free survival, recurrence, and prognosis [111112]. RBCT had a negative effect on clinical outcomes, mortality, recurrence, and complications in cases that required liver resection due to primary cancer in the liver [113114115]. It also had a negative effect on mortality, recurrence, and prognosis in cases that required surgery for gastric cancer [116117118]. Moreover, it was also reported that RBCT had a negative effect on long-term survival, recurrence, and long-term outcome in cases involving surgery for esophageal cancer [119120121122], while allogenic RBCT in cervical or ovarian cancer cases resulted in decreased survival and poor prognosis from increased metastasis [89123124]. When RBCT was performed during radical cystectomy for bladder cancer, it caused the postoperative tumor recurrence and cancer-specific mortality to increase [125]. When RBCT was performed on patients undergoing surgery for lung cancer, RBCT had a negative effect on 5-year disease-free survival [126].
8.4. Influence on oral cancer
Many cases of cancer are encountered in the field of orofacial surgery, which occasionally require perioperative RBCT. There have been many reports indicating that using RBCT during oral cancer surgery resulted in adverse outcomes. In a study comprised of 520 patients who underwent surgery for oral and oropharyngeal cancer, those who received an allogenic RBCT showed increased postoperative complications, which was reported to be associated with the amount of transfusion received [127]. In another study comprised of 276 patients who underwent oral cancer surgery, RBCT was reported to increase the rate of surgical-site infection [128]. A retrospective study on 1,693 patients who underwent oral cavity cancer surgery reported that RBCT was a risk factor for wound infection [129]. In various studies on patients who underwent surgery for oral cavity squamous cell carcinoma, performing RBCT with 3 units (U) or more shortened the survival and had a negative effect on prognosis [130131]. Moreover, RBCT during surgery for head and neck cancer resulted in an increased recurrence and decreased survival [132].
9. Influence on double-jaw surgery
Double-jaw surgery can potentially cause vascular injury or lead to a prolonged surgery, which may result in severe blood loss. Some studies have reported up to 1191 mL [133] of blood loss requiring fluid replacement with crystalloids, colloids, or blood products. Studies on the effects of RBCT during double-jaw surgery and prognosis are lacking. However, adverse effects from other surgeries may be anticipated. Therefore, induced/controlled hypotension may be considered as a method for reducing perioperative bleeding and RBCT [134135]. Study results on patients who underwent a Le Fort I osteotomy showed that the average blood loss in a group that used hypotensive anesthesia was 740 ml, whereas the average blood loss in the control group was 400 ml [136]. Furthermore, preoperative and intraoperative administration of the antifibrinolytic agent, tranexamic acid, is effective for controlling blood loss and improving the quality of the surgical field [137].
10. Influence on extra-operation
There are numerous study results indicating that RBCT in non-cancer surgeries result in poor prognosis. RBCT of 3 or more U during liver transplantation surgery increased the length of the hospital stay [138]. The patient group that received RBCT during a coronary artery bypass had a 5-year mortality that was twice as high as that of the group without RBCT [139]. In transcatheter aortic valve implantation surgery cases, using RBCT resulted in an increased 12-month mortality and prolonged hospital stay [140]. Even in major vascular surgery cases, RBCT increased the risk of myocardial infarction and 30-day mortality [141]. RBCT also induced a minor wound-healing disturbance in hip replacement surgery cases, while also increasing the length of the hospital stay [142]. For general surgery, 1 U RBCT increased the risk of 30-day mortality, composite morbidity, pneumonia, and sepsis/shock, while 2 U RBCT increased these outcome risks, as well as surgical-site infections [143].
AMOUNT OF TRANSFUSION
Are there differences in adverse effects according to the amount of transfused RBCs? A study comprised of 89,000 patients reported that the mortality and morbidity were higher in the patient group that received 1U RBCT than the non-transfused patient group, showing a dose-dependent tendency [144]. Besides mortality, wound problems, pulmonary complications, postop renal dysfunction, sepsis, morbidity, and length of the hospital stay were reported to be high in the group that received RBCT than that in the group that did not and caution was recommended when performing transfusions on patients with a mild anemia [144]. Other studies have reported poor outcomes when 2 U of RBC was used compared to that when 1 U was used [143]. Even in the field of orofacial surgery, there is evidence that a greater amount of RBCT has a greater negative effect on the outcome [127130]. In contrast, a study that compared restrictive (Hb < 7 g/dL) vs liberal (Hb < 9 g/dL) strategy on ICU patients who underwent major cancer surgery reported a higher rate of major complications in the restrictive group despite using a lesser amount of RBCT [145].
1. Amount of transfusion and bleeding in double-jaw surgery
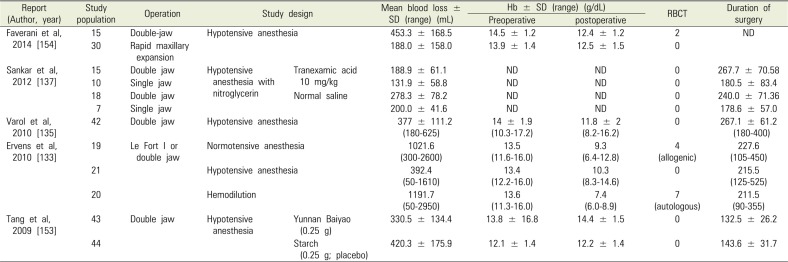
Orofacial surgery may be associated with significant bleeding. The amount of blood loss and transfusion is always a concern during double jaw surgery. In single jaw surgery, RBCT is considered unnecessary [146-148]. However, studies published prior to 2005 show that the average amount of bleeding in double jaw surgery ranged from 344 ml to 889 ml, while the percentage of RBCT varied widely between 0.8 % and 30 % [146148149150151152]. Meanwhile, recent studies (Table 2), including that by Tang et al., report that the mean blood loss was 420.3 ± 175.9 ml (range 183.0-965.6 ml) and there were no cases that required RBCT [153]. Ervens et al. report that the mean blood loss under normotensive anesthesia was 1,021.6 ml (range 300-2600 ml), while the preoperative Hb was 13.5 g/dL (range 11.6-16.0 g/dL) and the postoperative Hb was 9.3 g/dL (range 6.4-12.8 g/dL) [133]. Varol et al. reported a mean blood loss of 377.0 ± 111.2 mL (range 180-625 mL), preoperative Hb of 14.0 ± 1.9 g/dL (range 10.3-17.2 g/dL), and postoperative Hb of 11.8 ± 2.0 g/dL (range 8.2-16.2 g/dL) [135]. Sankar et al. reported a mean blood loss of 278.3 ± 78.2 mL [137]. Faverani et al. reported a mean blood loss of 453.3 ± 168.5 mL, preoperative Hb of 14.5 ± 1.2 g/dL, and postoperative Hb of 12.4 ± 1.2 g/dL and that RBCT was performed on 2 out of 15 patients [154]. As shown, there are differences in the measured amount of blood loss between studies. While recently published studies have shown that a few cases required RBCT, the amount of blood loss in double-jaw surgery was higher than that during other surgeries and some cases required transfusion. Therefore, it is necessary to prepare for situations that require a transfusion while continuously monitoring perioperative bleeding.
YOUNG (FRESH) VS OLD RBC
RBC concentrates are produced by removing the plasma fraction from centrifuged whole blood. Using 1 U of RBCs can typically increase the hemoglobin level by about 1 g/dL [155]. The number of storage days of RBC concentrates produced in this manner increased from 21 days to 42 days (at 1-6 ℃) when they were treated with hypotonic solutions such as anticoagulant-preservative solution, acid citrate dextrose, citrate phosphate dextrose, and citrate phosphate dextroseadenine [156157]. Based on this development, the study was conducted by dividing the RBC concentrates into groups of “young (fresh)” (< 14-21 days) and “old” (> 21 days) RBC concentrates. The increased storage duration of RBCs in hypotonic solution can lead to hemolysis, morphological changes, lactic acid accumulation, increased potassium/calcium, decreased 2,3-DPG and ATP, decreased pH and glycolysis rate, and the accumulation of various residues [158159160]. Because of this reason, transfusion using “old” RBC may cause adverse effects, including a higher infection risk and higher transfusion-dependent mortality rate [161162163]. Actually, a large-scale study conducted in Australia, Canada, Israel, and the US showed that the group that received a transfusion of “young” RBCs had a better prognosis than the group that was transfused with “old” RBCs [164]. However, there are other studies that report no difference in prognoses between the two groups [165] and a study that reports that an “old” RBC transfusion had the benefit of reducing cancer recurrence [163]. Therefore, this is an issue still under debate and there is the need for a sufficient discussion on issues that can arise a preference for “young” RBCs.
AUTOLOGOUS BLOOD TRANSFUSION
Various aforementioned RBCT risks are mostly associated with allogenic transfusion. An allogenic RBCT is not only the cause of various adverse events, but it also increases the economic and psychological burden of the patient. On the other hand, an autologous transfusion can avoid various adverse events associated with an allogenic transfusion, while addressing the issue of lack of blood and reducing the economic burden of the patient [166167]. A randomized study on CRC surgery reported that the recurrence rate was lower with autologous RBCT compared to that of an allogenic RBCT [168]. An autologous RBCT is frequently used during double-jaw surgery in the field of orofacial surgery and an autologous RBCT can serve as a method for reducing allogenic RBCT [169]. The following are the three options for an autologous RBCT: preoperative autologous blood donation (PABD), acute normovolemic hemodilution (ANH), and intraoperative and postoperative autotransfusion.
1. Preoperative autologous blood donation (PABD)
PABD refers to the method of drawing blood from the patient preoperatively and keeping it until reinjecting it into the patient intra- or postoperatively. Repeated blood donations before surgery can stimulate bone marrow cell proliferation, stimulate erythrocyte regeneration, increase hematopoietic function in patients after surgery, accelerate the patient's hematopoietic recovery after surgery, is conducive for wound healing, and reduces the chances of infection caused by immunoreaction from allogenic RBCT [170]. In addition, the improved autologous RBCT has a number of advantages such as the mild dilution of blood, improved microcirculation, reduction in blood viscosity, and prevention of hypoxia caused by anemia after blood donation [171].
For Hb ≥ 11 g/dL, donation 4 days prior to surgery is recommended, but donations for a ≥ 8-9 ml/kg is not recommended. Oral iron may be helpful for restoring the Hb to the level prior to donation. Contraindications include bacteremia and acute localized infection, myocardial infarction in the past 6 months, unstable angina, aortic stenosis, congestive heart failure, significant ventricular arrhythmias, marked uncontrolled hypertension, and cerebrovascular accident within 6 months.
2. Acute normovolemic hemodilution (ANH)
ANH is a method of autologous transfusion, which was first introduced in 1946, and is still widely used today [171]. ANH is generally performed under general anesthesia and prior to the start of surgery. Blood is drawn from the patient and stored and an equivalent amount of crystalloid (1:3) or colloid (1:1) fluid is added to maintain the plasma volume. If required intra- or postoperatively, the collected blood can be reinjected to the patient [172]. ANH can effectively reduce erythrocyte loss caused by perioperative bleeding and reduce allogenic RBCT [173174]. This method is widely used for postpartum hemorrhage and cancer and orthopedic surgeries, such as joint replacement and spine surgery. Moreover, this method is used in the field of dentistry when cancer or double jaw patient with expected bleeding is a Jehovah's Witness [175]. This method offers several advantages. The first is the reduction of perioperative erythrocyte loss since crystalloid or colloid, in equivalent amount as blood collected, is used to restore volume. This enhances the body's tolerance and reduces actual blood loss [172176]. The second advantage is that it is simpler and less costly than the PABD method. The third advantage is that it is the only method that can provide fresh autologous blood that has almost no effect on the functions of platelets and clotting factors. ANH may be used in cases where Hb is > 11 g/dL and platelets are > 100 × 109 /L and the prothrombin time and cardio-pulmonary function are normal [177].
3. Intraoperative or postoperative autotransfusion
Intraoperative or postoperative autotransfusion refers to a method of transfusion in which the blood in the body cavity of a patient, blood lost during surgery, and postoperatively drained blood, can be recovered through a blood recovery device [171]. The blood subsequently undergoes anticoagulation, filtration, and washing and is finally transfused back to the patient [178]. The American Association of Blood Banks guidelines recommended intra- or postoperative autotransfusion when perioperative bleeding (more than 20% total volume) is expected. However, it is not recommended for intraoral surgeries, such as oral cancer or double jaw surgeries, due to the risk of systemic infection caused by the resident bacteria inside the oral cavity.
CONCLUSION
The answer to the question whether RBCT during perioperative period is beneficial or harmful to patient is not an easy one. In the field of orofacial surgery, transfusion is performed for the purpose of oxygen transfer to hypoxic tissues and plasma volume expansion when there is bleeding. Many studies and guidelines have suggested a hemoglobin level of 7 g/dL for general patients and 8-9 g/dL for patients with cardiovascular disease or hemodynamically unstable patients as the trigger for RBCT. However, RBCT is an essential treatment for surgeries and it is often required in emergency cases. We need to consider perioperative bleeding, various clinical situations, level of intra- and postoperative patient monitoring, and various problems that may arise from a RBCT in a comprehensive manner from the perspective of patient safety. Since orofacial surgery carries an especially high risk of bleeding due to the complex structures involved and extensive vascular distribution, measures to prevent bleeding should be taken and the conditions for a transfusion should be optimized and appropriate in order to promote patient safety.
 XML Download
XML Download