

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thalamic tumors constitute about 1–5% of pediatric intracranial tumors [12345]. Gliomas predominate among pathologic diagnoses. The proportion of high-grade lesions is much higher in thalamic tumors than in tumors in other locations of brain [56]. In the past, conservative approaches such as stereotactic biopsy or radiotherapy were preferred for treatment of thalamic tumors rather than radical resection because the thalamus is surrounded by important white matter tracts and the thalamus itself is a crucial structure [7]. However, it has been reported that the efficacy of chemotherapy and survival can be increased by resection of these tumors [89]. Currently, with the help of preoperative neuroimaging and intraoperative neurophysiological monitoring (IOM), surgical resection of thalamic tumors has become achievable with acceptable morbidity [24567101112].
Because of the rarity of thalamic tumors in children, the surgical outcomes and relevant prognostic factors for this disease are not clearly defined. Furthermore, the role of the aforementioned technologies on outcomes, including the extent of resection and postoperative neurological status, has not been clearly stated. Therefore, we reviewed the records of 37 children with thalamic tumors and evaluated the surgical outcomes and relevant prognostic factors. This study provides up-to-date information regarding the role of diffusion tensor imaging (DTI), neuro-navigation and IOM in the treatment of pediatric thalamic tumors.
MATERIALS AND METHODS
The Institutional Review Boards of Seoul National University Hospital approved the study protocol (H-1610-079-799). We retrospectively reviewed the medical records of 37 children with thalamic tumors treated at the Division of Pediatric Neurosurgery of Seoul National University Children's Hospital from March 2004 to December 2017. The data include demographics, presenting symptoms, imaging characteristics, tumor extent, histology, treatment received and follow-up. The median follow-up duration was 19 months (range from 1 to 225 months).
We independently reviewed the preoperative and postoperative MRI to determine the epicenter of the tumor, the neighboring structures and the extent of tumor resection. There were 44 operations in our study. Twenty-seven cases were tumor resections, and the other 17 cases were biopsies. DTIs were done before surgery in 17 tumor resections, and these images were reviewed by a pediatric neuroradiologist (Choi Y.H.), particularly for the displacement of the thalamus and the internal capsule. Neuro-navigation was employed in 23 cases, and IOM was used in 14 cases.
The extent of resection was divided into gross total resection (GTR, 100% removal), subtotal resection (STR, 90–99% removal) and partial resection (PR, <90% removal) based on the intraoperative findings and postoperative MRIs. The postoperative neurological outcomes were divided into two groups: “Worsened” and “Not worsened”. Neurological evaluations included mental status and motor grades of extremities. The “Worsened” group had decreased mental status from alert to less than alert or a decreased motor grade to ≤3 from a motor grade of ≥4. Patients not meeting these criteria were included in the “Not worsened” group [1314]. Pathology specimens were reviewed by a neuropathologist (Park S.H.). All diagnoses were reviewed according to the 2016 World Health Organization (WHO) Classification of Tumors of the Central Nervous System (CNS) [15].
Statistical analysis was performed using the SPSS 19 statistical package (IBM Corp., Armonk, NY, USA). Fisher's exact test was used for binary of categorical variables. We calculated progression-free survival (PFS) and overall survival (OS) using the Kaplan-Meier method. For comparison of variables in the Kaplan-Meier curves, a log-rank test was used. The level of significance (p) was 0.05 for all the tests.
RESULTS
Clinical features
Thirty-seven patients were enrolled in the study. Age at diagnosis ranged between 1.1 and 21.5 years (median 9.8 years). The male to female ratio was approximately 1:1. The duration of symptoms ranged between 0.2 and 28 weeks (median 2 weeks). Symptoms of increased intracranial pressure (n=20) and hemiparesis (n=8) were the most common presenting symptoms, followed by tremor (n=4), dizziness (n=1), gait disturbance (n=1), and rigidity (n=1). Two patients had MRI because of head trauma, and the tumors were considered incidental lesions.
Neuroimaging
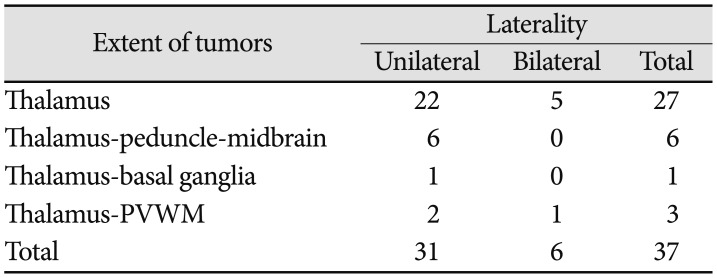
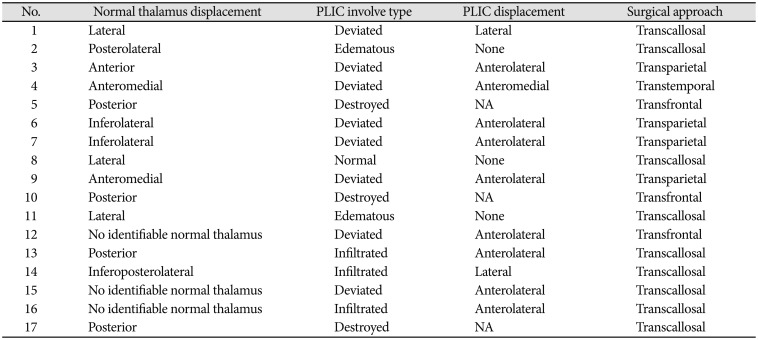
Thirty-one patients had unilateral thalamic tumors, and 6 patients had bilateral thalamic tumors (Table 1). Tumors were only located in the thalamus in 22 patients with unilateral tumor and 5 with bilateral tumors. Tumors extended to the cerebral peduncle and midbrain in 6 patients with unilateral tumor. The tumor extended to the basal ganglia in 1 patient with a unilateral tumor. Tumors extended to the periventricular white matter in 2 patients with unilateral tumors and 1 with a bilateral tumor. Preoperative DTIs were done in 17 tumor resections. In particular, displacement and involvement of the posterior limb of the internal capsule (PLIC) was evaluated by DTI because it is important to avoid this crucial structure in planning surgical approach in order to avoid postoperative hemiparesis [16]. Eleven cases had displacement of the PLIC (8 anterolateral deviation, 2 lateral deviation and 1 anteromedial deviation) and among them, 3 had PLIC infiltration. The PLIC was not visualized in 3 cases that had heavy destruction of the PLIC by tumor. Three cases had normal position of the PLIC. These data, including the surgical approach planned with DTI findings, are summarized in Table 2.
Tumor resection
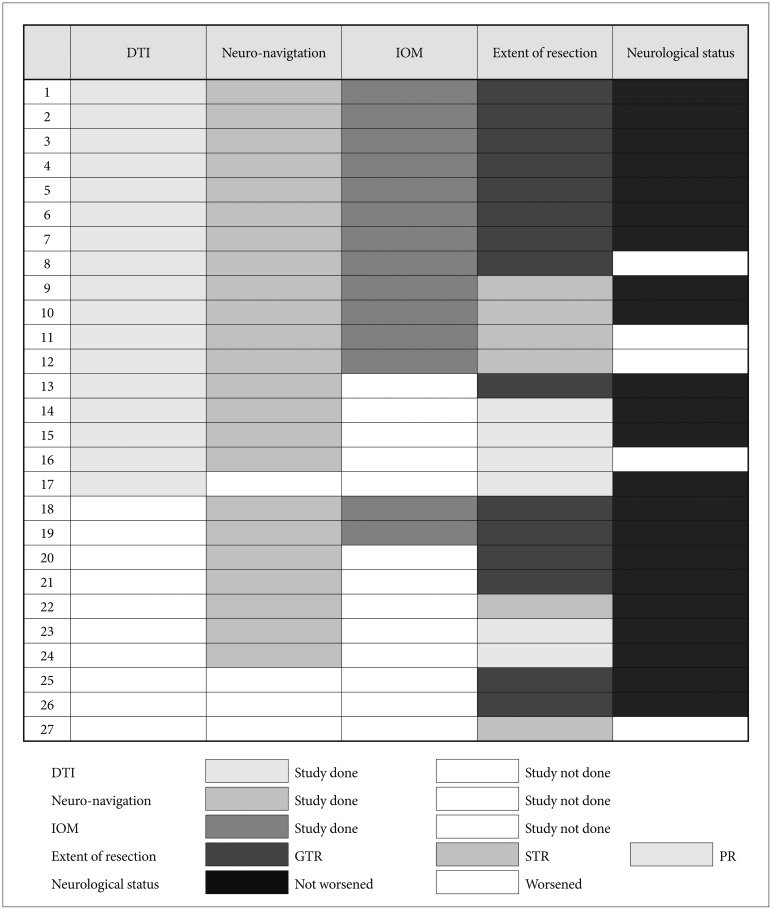
Forty-four operations were performed for these 37 patients. We performed 17 biopsies and 27 tumor resections. Among the 27 tumor resection cases, 15 cases were GTR, 6 were STR and 6 were PR. Thirteen tumor removals were done via interhemispheric transcallosal approaches, and 14 tumor resections were made via transcortical approaches. When we compared the extent of resection between the group with DTI, neuro-navigation and IOM (n=12) and the group without at least one of the three techniques (n=15), all 12 tumor resection cases in the former group were GTR or STR, and 9 out of 15 tumor resection cases in the latter group were GTR or STR (Fig. 1). The difference was statistically significant (p=0.020).
Neurological status after tumor resection
There were 27 tumor resections in 23 patients. In 22 tumor resection cases, neurological status did not worsen after surgery. In 5 tumor resection cases, neurological status worsened after surgery. When we analyzed the differences in neurological status between the group with DTI, navigation MRI and IOM and the group without at least one of the aforementioned measures, the difference was not statistically significant (p=0.294). The extent of resection and PLIC involvement were not related to postoperative neurological status changes.
Histopathological findings
The pathological diagnoses of the 37 patients were as follows: ten patients had glioblastoma, IDH-wildtype (GBL); 6 patients had anaplastic astrocytoma, IDH-wildtype (AA); 6 patients had pilocytic astrocytoma (PA); 6 patients had diffuse midline glioma, H3 K27M-mutant (DMG); 4 patients had CNS-embryonal tumor, NOS; 3 patients had diffuse astrocytoma, IDH-wildtype (DA); 1 patient had germinoma; and 1 patient had anaplastic ependymoma.
Adjuvant therapy
Of the 37 patients, 23 (56%) patients had both chemotherapy and radiotherapy following surgery. Three patients had only radiotherapy, one patient had only chemotherapy, and 10 patients had no adjuvant treatment.
Seven patients with GBL received chemotherapy with temozolomide (Stupp protocol) [17]. Five out of 6 patients with DMG received chemotherapy. Four of them received temozolomide (Stupp protocol), and one had POG9031 [18] for a diagnosis of primitive neuroectodermal tumor based on the 2000 WHO Classification of Tumors of the CNS. Patients with AA received varied chemotherapy regimens (procarbazine+CCNU+vincristine; temozolomide+thalidomide; Stupp protocol). Patients with CNS-embryonal tumor, NOS also had various chemotherapy regimens (carboplatin+etoposide+ifos famide; carboplatin+vincristine+temozolomide; etoposide+cyclophosphamide).
Treatment outcomes
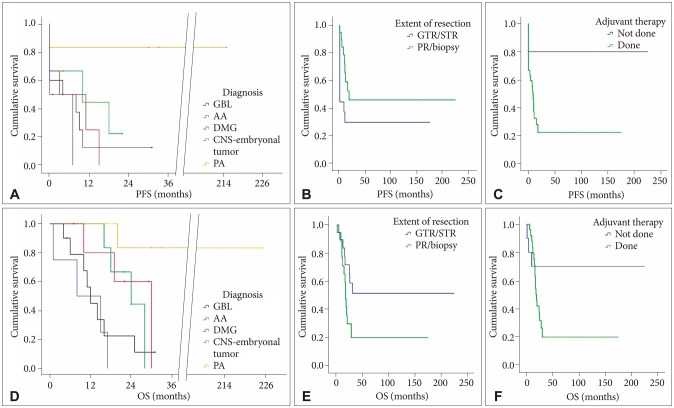
The mean PFS was 87.2±38.0 months. The mean PFS was 7.7±6.5 months for GBL; 11.1±7.5 months in AA; 7.0±5.8 months for DMG; 3.5±4.3 month for CNS-embryonal tumor, NOS; 122.0±86.5 months for DA; and 187.5±68.5 months for PA. The 5-year PFS was 37%. The mean OS was 90.7±36.1 months. The mean OS was 14.5±5.4 months for GBL; 23.4±4.6 months for AA; 23.8±8.9 months for DMG; 10.3±7.3 months for CNS-embryonal tumor, NOS; 122.3±86.0 months for DA; and 190.8±62.4 months for PA. The 5-year OS was 47% (Fig. 2).
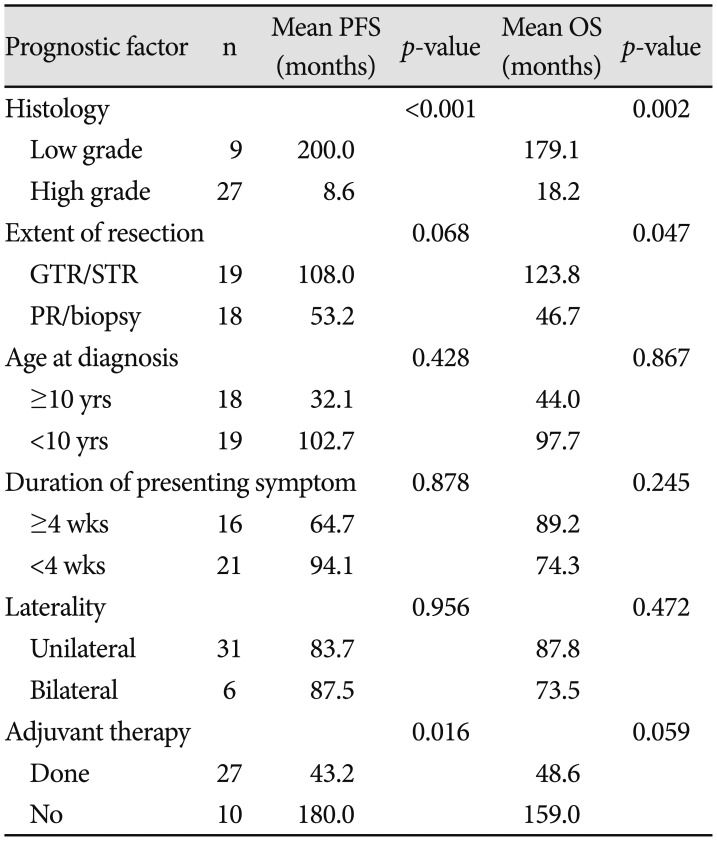
In 9 patients with histopathologically proven low-grade tumor (PA, DA), the mean PFS was 200.0 months, and the mean OS was 179.1 months. In 27 patients with high-grade tumors excluding germinoma (GBL; AA; DMG; CNS-embryonal tumor, NOS; anaplastic ependymoma), the mean PFS was 8.6 months, and the mean OS was 18.2 months. The difference between both PFS and OS between low-grade and high-grade tumors was statistically significant (p<0.001, p=0.002) (Table 3). Nineteen patients with GTR/STR had a mean PFS of 108.0 months and a mean OS of 123.8 months, while 18 patients with PR/biopsy had a mean PFS of 53.2 months and a mean OS of 46.7 months. The difference of the mean OS between these two groups was statistically significant (p=0.047). However, there was no difference in the mean PFS between the two groups (p=0.068). Ten patients without adjuvant therapy had a mean PFS of 180.0 months and a mean OS of 159.0 months, while 27 patients with adjuvant therapy had mean PFS of 43.2 months and mean OS of 48.6 months. The difference of mean OS between these two group was not statistically significant (p=0.059). However, there was significant difference of mean PFS between two groups (p=0.016) (Fig. 2).
We also divided the patients into two groups according to various factors such as age (≥10 years, <10 years), duration of symptoms (≥4 weeks, <4 weeks) and laterality (unilateral, bilateral). None of these factors were statistically significant in terms of differences of the mean PFS or mean OS.
DISCUSSION
There has been some controversy regarding surgical removal of thalamic tumors because of uncertain outcomes and operative morbidities. Previously, Bernstein et al. [19] and Beks et al. [20] recommended biopsy or PR with adjuvant treatment. As surgical techniques improved, Cuccia and Monges [2] stated that surgical resection of thalamic tumors must be done regardless of tumor grade. Recent studies also found that GTR or STR improved survival of patients with thalamic tumors [51112]. In our study, GTR or STR of tumor proved to be a statistically significant factor for OS. Especially in low-grade tumors, it appears that radical tumor removal is much more important for survival. In the present study, GTR or STR was performed in 6 of 9 patients with low-grade tumors, and all 6 patients have survived to date. For high-grade tumors, there was no statistically significant difference in PFS and OS between the GTR/STR group and the PR/biopsy group. Nevertheless, surgical resection of tumor can also be meaningful in high-grade tumor because it can stabilize the patient's status during adjuvant treatment by relieving increased intracranial pressure and mass effect. Furthermore, it can decrease target volume of radiotherapy. Tumor grade was the most statistically significant factor related to differences in both PFS and OS, as also reported in other studies [457111216]. Interestingly, adjuvant therapy was also a statistically significant factor for difference in PFS. This probably reflected the fact that patients with high-grade tumors were more likely to have adjuvant therapy than were patients with low-grade tumors. Unlike other reported studies [5712], symptom duration and laterality proved to be irrelevant to both PFS and OS in the present study.
Unless the tumor has clear margins with normal brain tissues, radical resection of thalamic tumor carries too much risks of postoperative morbidity even to an experienced surgeon. But with advancements in imaging technologies and IOM, maximal surgical removal of thalamic tumors can be achieved with acceptable morbidity. Twenty-seven tumor resections were done for 23 patients in the present study. Staged operation was done in 4 patients, and one of them was operated on emergently because of tumor bleeding. In 27 tumor resection cases, GTR or STR were performed in 21 (78%), a higher percentage than reported in other series [571112], and neurological status worsened in only 5 cases (19%), similar to results from recent studies [51621]. In addition, there was a statistically significant difference in the extent of resection between the group that employed DTI, neuro-navigation and IOM and the group that did not employ at least one of the aforementioned measures. Nevertheless, there was no statistically significant difference in postoperative neurological status between the two groups. The lack of difference in morbidity may be attributed to a more conservative surgical approach employed to minimize neurological deficits in the latter group. This is also reflected in the difference in the extent of resection, because extent of tumor resection could be maximized to the where crucial structures were not injured with application of these aforementioned technologies.
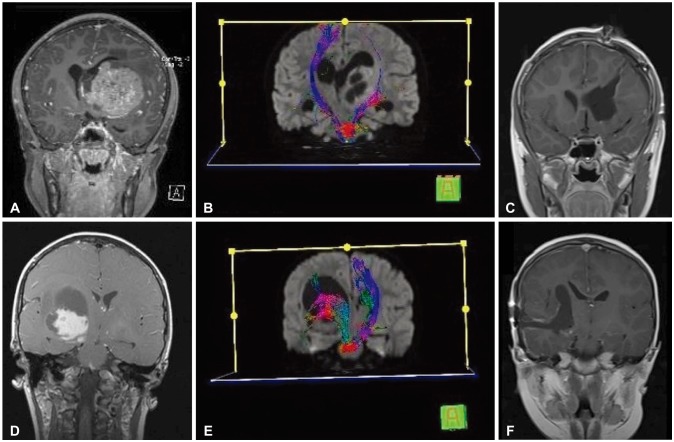
In planning a surgical approach, DTI has been introduced in several reports [101622]. Using DTI, we analyzed exact location of the tumors, displacement of the thalamus and PLIC and then planned the appropriate surgical approach without invading either the thalamus or the PLIC [1622]. We favor the anterior interhemispheric transcallosal approach when this approach does not invade any eloquent structure such as the thalamus or the PLIC. Evaluation by DTI was done in 17 tumor resection cases, and about half of the surgeries (n=9) were performed via the interhemispheric transcallosal approach. In cases of anterior or medial displacement of the thalamus, we choose other transcortical approaches such as the transparietal or transtemporal approach, according to deviation of the PLIC. In case of posterior displacement of thalamus with destroyed PLIC, we choose the transfrontal approach. Following this principle, 8 surgeries were performed via the transcortical approach (Fig. 3). But one must be cautious about application of DTI in planning surgical approach because DTI has some limitations. First, DTI is dependent on operators which leads to difficult in interpretations and standardization [23]. And DTI is low resolution image that shows averaging effects of multiple crossing fibers in a voxel. Also, there is not established result that whether resection of fiber that seems to be infiltrated or destroyed by tumor in DTI will cause permanent neurologic deficit [24]. This may reflected in the our result that there is no difference in extent of tumor resection between group with DTI and group without DTI.
Before 2016, the patients in this study were diagnosed and treated based on previous WHO Classification of Tumors of CNS. In the present study, we reviewed all pathologic specimens and rediagnosed them based on the 2016 WHO Classification of Tumors of the CNS. Therefore, it would be necessary to conduct further studies that include patients who were diagnosed and treated after 2016.
In conclusion, maximal surgical resection can be achieved with acceptable morbidity by employing DTI, navigation MRI and IOM. Maximal tumor resection should be the initial therapeutic consideration for the treatment of thalamic tumors, especially low-grade tumors.
 XML Download
XML Download