

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Hepatocellular carcinoma is unique in that it largely occurs within an established background of chronic liver disease and cirrhosis, which are mostly attributed to hepatitis B virus (HBV) and hepatitis C virus (HCV), the main causal agents of chronic hepatitis.1 In South Korea, where 5~6% of the population are carriers of HBV, there are approximately 10,000 new hepatocellular carcinoma (HCC) cases each year, and the overall incidence rate of HCC is 46.5 cases per 100,000 population, making it the third most common cancer in Korea after stomach and lung cancers.2
With treatment options of liver transplantation, radiofrequency ablation, transarterial chemoembolization (TACE), and radiation therapy, the optimal management of HCC remains controversial. In patients with anatomically resectable tumors and adequate hepatocellular function, liver resection is the first consideration in most medical centers.3 However, although surgical resection offers patients with HCC a chance for cure, the post-resection tumor recurrence rate is high, with reported cumulative 5-year tumor recurrence rates ranging from 40 to 70%.45 Poon and colleagues reported different risk factors and prognoses as a function of early and late intrahepatic recurrence after resection by comparing postoperative time periods of 6, 12, 18, and 24 months.678
The objective of the current study was to identify risk factors of intrahepatic recurrence and post-recurrence survival after potentially curative resection of HCC in patients with hepatitis B virus infection. The results identify a patient subset at high risk for tumor recurrence and are useful for decisions regarding adjuvant treatment modalities.
Methods
Between January 1999 and December 2003, 59 patients at Hospital our with hepatitis B virus infection underwent potentially curative liver resection for HCC. Patients with other causative viral infections were excluded. Curative resection was defined as complete resection of the tumor with a clear microscopic margin and no residual lesion on ultrasonography or CT scan within the first month postoperatively. The patients were followed-up by the surgical team with serum AFP tests, liver function tests, and ultrasonography monthly in the first year and every 3 months thereafter. CT scans, hepatic angiography, or fine-needle aspiration cytology were done to confirm the diagnosis of disease recurrence. All patients were observed for at least 3 years, and the median duration of follow-up was 40 months. Clinical, biological, and histopathological characteristics of these patients were collected and tested for their prognostic significance using the Chi-square test and the Student's t-test. We evaluated risk factors for intrahepatic recurrence as a function of time after surgery (early vs. late recurrence). We defined intrahepatic recurrence up to 12 months postoperatively as the early recurrence group; recurrence after 12 months post-operatively was the late recurrence group; those who did not experience intrahepatic recurrence in the median follow-up period was the non-recurrence group. Time to recurrence and survival rate were analyzed by the Kaplan-Meier method and log-rank test using SPSS software version 14.0 for Windows. p<0.05 was considered statistically significant.
Results
1. Patient and tumor characteristics
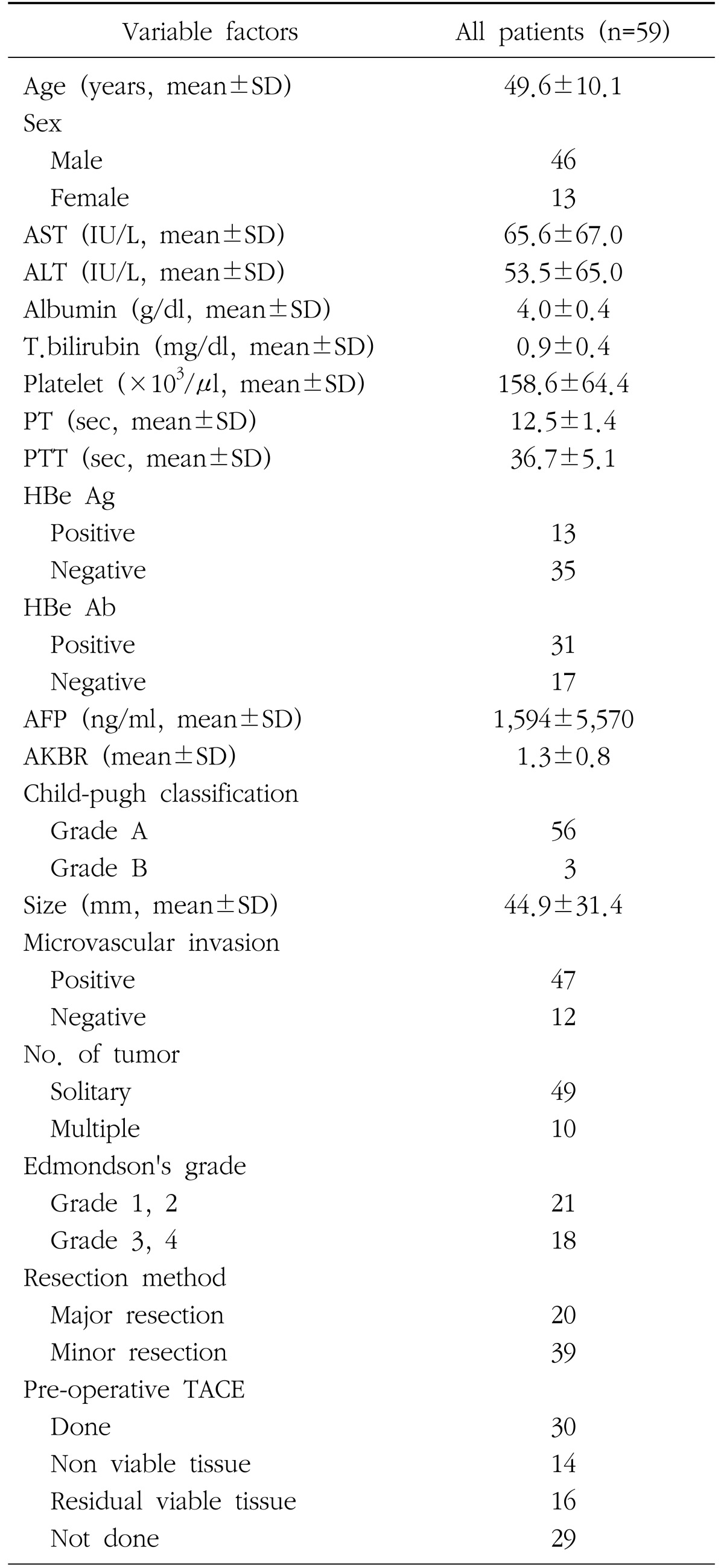
Data from 59 patients diagnosed with HCC and with hepatitis B virus infection were analyzed. Their clinical characteristics are summarized in Table 1. There were 46 (78%) males and 13 (22%) females. Preoperative mean blood analyte levels were: AST 65.6 IU/L, ALT 53.5 IU/L, and alpha fetoprotein 1,594 ng/ml. Forty-eight patients were tested for HBe Ag and HBe Ab; 13 (27%) were positive and 35 (73%) were negative for HBe Ag. The mean tumor size was 44.9 mm. There was a solitary tumor in 49 (83%) patients and multiple tumors in 10 (17%) patients. Histologically, 47 (79%) patients showed microvascular tumor invasion. Major hepatectomy, such as right or left hepatectomy, was done for 20 (34%) patients, and minor hepatectomy, such as segmentectomy or wedge resection, was done for 39 (66%) patients.
2. Risk factors influencing early and late intrahepatic recurrence
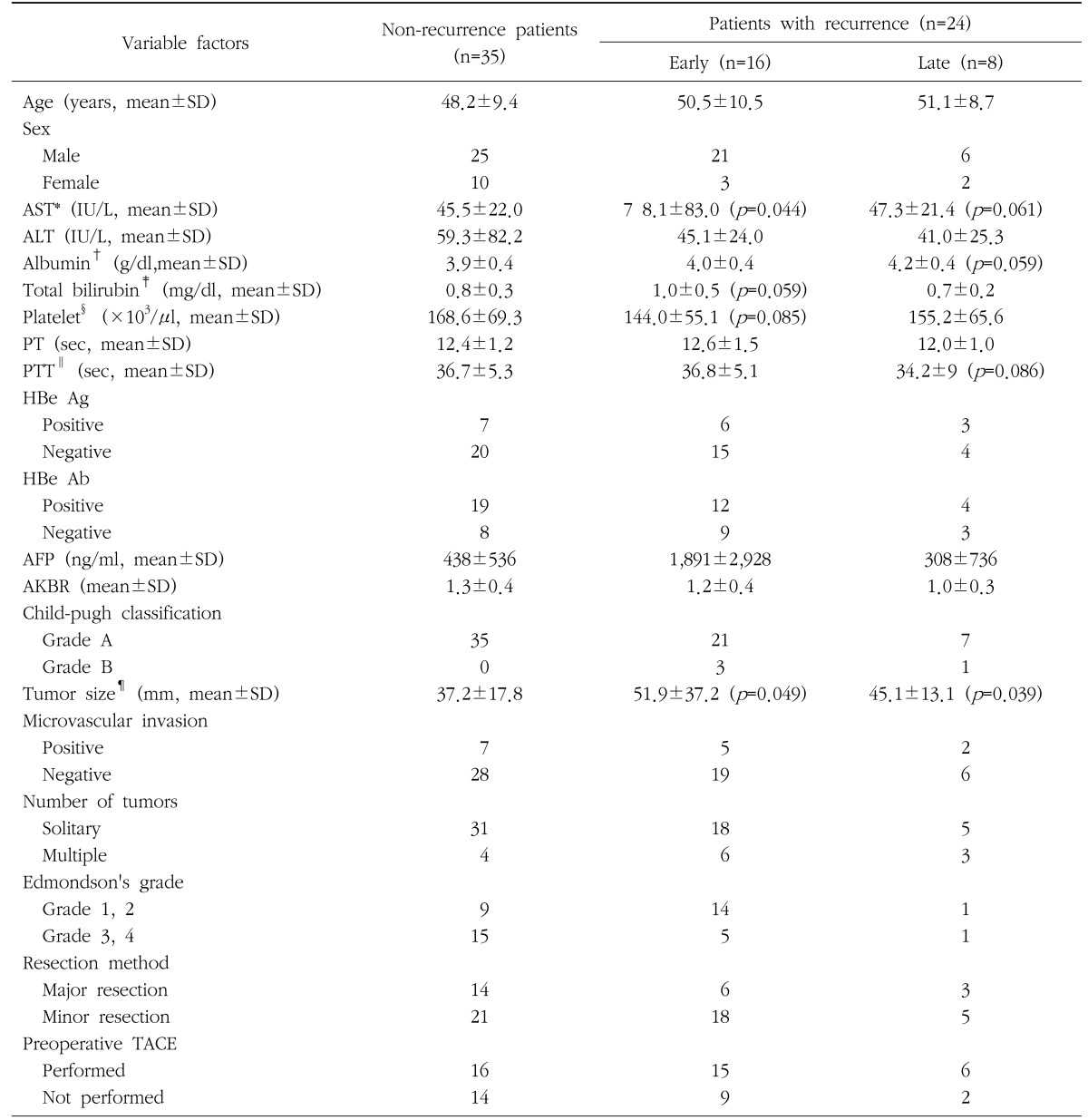
Prognostic factors were analyzed using the chi-square test and the Student's t-test (Table 2). Of the 59 patients who underwent liver resection, 24 (41%) experienced intrahepatic recurrence and 35 did not. Of the 24 with recurrence, 16 (25%) were in the early recurrence group, and 8 (14%) were in the late recurrence group (Table 2). Mean serum AST was 78.1±83.0 IU/L in the early recurrence group and 45.5±22.0 IU/L in the non-recurrence group (p=0.044). The mean tumor size was 51.9±37.2 mm in the early recurrence group and 37.2±17.8 mm in the non-recurrence group (p=0.049). Thus, increased tumor size and level of serum aspartate aminotransferase (AST) were significantly associated with early intrahepatic recurrence. Differences in total bilirubin and platelet levels were not statistically significant but our study may have been underpowered to show a significant effect. Total bilirubin was slightly higher in the early recurrence group than in the non-recurrence group (p=0.059), and platelet count was lower in the early recurrence group than the non-recurrence group (p=0.085) (Table 2). Mean tumor size was 45.1±13.1 mm in the late recurrence group and 37.2±17.8 mm in the non-recurrence group (p=0.039). Serum AST, albumin and PTT just missed statistical significance. Therefore, risk factors for early recurrence are serum aspartate aminotransferase (AST) level (p=0.044) and tumor size (p=0.049), whereas for late recurrence, tumor size (p=0.039) was the only risk factor.
3. Survival rate
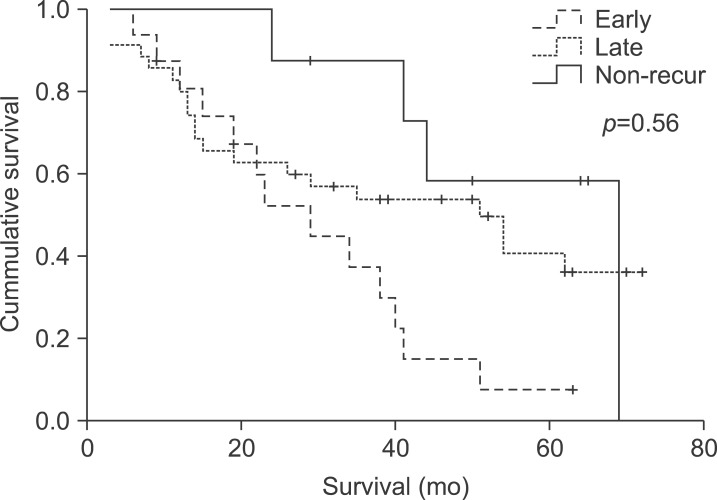
The mean follow up period was 40 months. The 1-, 3-, and 5-year overall survival rates of enrolled patients were 83%, 63%, and 42%, respectively. The 1-, 3-, and 5-year overall survival rates after recurrence were 87%, 52%, and 20%, respectively. Differences in survival rate between early, late, and non-recurrence groups were not quite statistically significant (p=0.056) (Fig. 1).
Discussion
Although radical resection is the most effective treatment method for hepatocellular carcinoma, it has been reported that the long-term survival rate is low due to the high recurrence rate after hepatectomy and, according to these reports, 69~75% of cases recur within 5 years and 78~ 92% of these are intrahepatic recurrence.91011 The recurrence of hepatocellular carcinoma is believed to be caused by intrahepatic metastasis through the hepatic portal vein and metachronous multicentric carcinogenesis in the remaining liver parenchyma.712 In addition, some studies have reported chronic active hepatitis and liver cirrhosis as the most important risk factors of multicentric carcinogenesis. 1314 According to these reports, the repeated inflammatory responses and hepatocellular necrosis in chronic hepatitis and liver cirrhosis patients ultimately induce mitosis in liver cells and accelerate the growth of hepatocellular carcinoma cells.
For the last 20 years, many studies have been conducted on the factors influencing the recurrence of hepatocellular carcinoma in order to enhance the survival rate after hepatectomy. Salleh et al.15 reported that serum AST, the presence of satellite nodules, and microvascular invasion are involved in the recurrence of hepatocellular carcinoma related to hepatitis B and C viruses. In addition, Ou et al.16 reported that serum alphafetoprotein, vascular invasion, the distance from the tumor to the resection margin, and preoperative transfusion are factors involved in the early recurrence of hepatocellular carcinoma related to hepatitis B virus, and the grade of differentiation of the tumor and the number of intrahepatic metastatic lymph nodes are involved in late recurrence. Adachi et al.17 reported that intrahepatic infection is an important factor influencing recurrence and that adhesion molecules adhering to cancer cells in liver undergoing an inflammatory response are involved in postoperative recurrence.
As mentioned above, an intrahepatic chronic inflammatory response is not only a causative factor of primary hepatoma, but also can be a major factor influencing its recurrence after hepatectomy.15 Park and colleagues5 reported that, of 904 patients with HCC in a hepatitis B virus-endemic area, 76.3% were positive for hepatitis B antigen, and 72.7.% showed the presence of cirrhosis.
Similarly, in our study, the preoperative level of serum AST in hepatoma patients with hepatitis B was a factor affecting recurrence after hepatectomy. This was statistically significant, particularly in the early recurrence group, and suggests that a severe inflammatory response in the liver is related to recurrence.
Some authors have reported that interferon therapy can inhibit recurrence after hepatectomy and can prevent hepatocellular carcinoma caused by a continuous inflammatory response. van Zonneveld et al.18 did a long follow-up study of a response group showing loss of HBeAg and a non-response group showing HBeAg positivity continuously after interferon therapy, and reported that the incidence of hepatocellular carcinoma decreased and the survival rate increased significantly in the interferon therapy response group. Choi et al.19 used interferon to treat Korean chronic hepatitis B patients who were positive for HBe, and reported that the survival period was extended and the incidence of hepatocellular carcinoma decreased in the group maintaining a continuous response.
Considering these previous reports, the identification of AST as a risk factor of recurrence in this study is believed to reflect the environment of continued chronic inflammation or the progression of hepatic fibrosis resulting from continuous viral activity. In addition to the limitations of a retrospective study, the number of patients tested for preoperative HBV DNA in this study was small and therefore we could not analyze the association between the recurrence of cancer and virus replication, which is likely to either sustain hepatic inflammation or to be directly involved in the occurrence of cancer. Further research is considered necessary on the relationship between the use of antiviral drugs and postoperative recurrence, and on the effect on recurrence of hepatitis B viral load and HBe Ag clearance after the use of antiviral drugs. Lang et al.20 reported that liver cirrhosis is one of the most important risk factors of hepatocellular carcinoma, and that 85~90% of hepatocellular carcinoma patients also have liver cirrhosis. Most of the eight patients who experienced late recurrence in this study also suffered progressive liver cirrhosis and, in contrast to the early recurrence group, the late recurrence group typically received only conservative treatment due to severe liver failure.
Park et al.21 reported that tumor size - hepatocellular carcinoma ≥5 cm diameter - is associated with postoperative early recurrence. When the tumor is large, there is a high possibility of microvascular invasion by hepatocellular carcinoma that is barely detectable on imaging, the grade of differentiation is low, and the disease is often multinodular, which is a factor related to recurrence. Furthermore, many cases are accompanied by liver cirrhosis, which causes hepatic dysfunction and makes it difficult to secure a sufficiently large resection margin. These factors are believed to be associated with the high recurrence rate after hepatectomy when the tumor is large.2223
In our study, although the mean size of the mass was 44.9 mm for all of the surgical patients, it was 37.2 mm in the non-recurrence group and 51.9 mm in the early recurrence group and the difference between the two groups was statistically significant (p=0.049). Thus, the size of the mass is believed to affect both early recurrence and late recurrence.
We followed patients with hepatocellular carcinoma related to hepatitis B for an average of 40 months postoperatively, and did not see a statistically significant difference in the survival rate among the non-recurrence group, the early recurrence group, and the late recurrence group (p=0.056), although it just missed being significant. In addition, no difference in the survival rate was observed between the non-recurrence group and the late recurrence group.
Summing up, as described in many previous reports on the postoperative survival rate of patients with hepatocellular carcinoma related to hepatitis B, early recurrence is considered an important factor related to the survival rate.
Conclusion
Our findings indicate that patients with the risk factors of large tumor size and high level serum aspartate aminotransferase should have more careful supervision, and more aggressive follow-up and decisions regarding adjuvant treatment modalities. Adequate actions such as detection of early recurrence, rehepatectomy, transcatheter arterial chemoembolization, and radio-frequency ablation may be directly linked to a rise in the survival rate. Moreover, additional studies may be required on the early recurrence of hepatocellular carcinoma related to hepatitis B, particularly on the association between liver function, HBV DNA and recurrence.
 XML Download
XML Download