

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Chronic subdural hematoma (CSDH) occurs frequently in elderly patients and it is associated with acquired predisposing factors, such as trauma, the use of antiplatelets, and chronic alcohol overuse.28) In contrast, arachnoid cysts (ACs) are mostly of congenital origin and develop in pediatric patients. The prevalence of the cyst is approximately 1% of nontraumatic intracranial lesions.1524) CSDH contains a collection of old blood and its breakdown products between the dura and brain parenchyma, while AC mainly consists of cerebrospinal fluid (CSF) in cavity surrounded by the arachnoid membrane or between the arachnoid and pia mater.
They are generally isolated disease entities. However, in rare incidences they may occur concomitantly, and in these cases, the recurrence rate of CSDH increases.1351214) Although an acceptable method for treating primary CSDH is burr-hole trephination, a consensus for recurrent CSDH has not been reached yet. Many studies have applied and reviewed various methods of treating the recurrence, but no recognized treatment guideline has been developed.19)
Among the several treatment methods for recurrent CSDH, middle meningeal artery (MMA) embolization has been suggested as a method for treating refractory CSDH.792023) However, to our knowledge the technique has not been attempted in South Korea. Thus, we report treating a patient who suffered from both AC and recurrent CSDH with Burr-hole trephination and MMA embolization.
Case Report
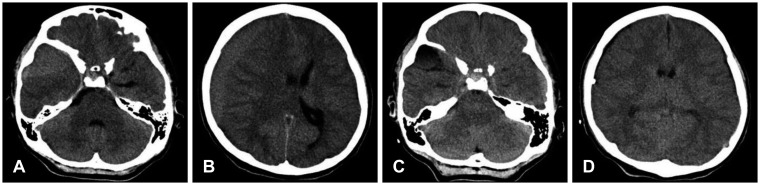
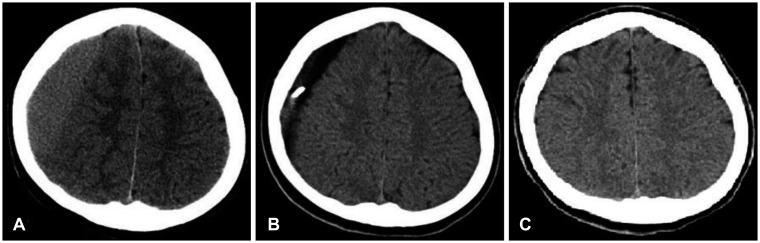
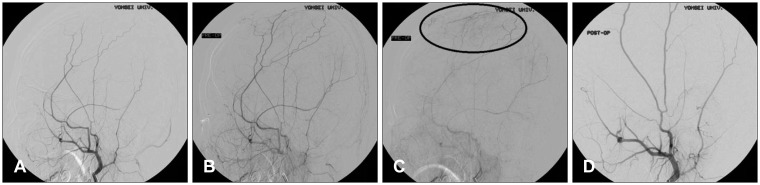
A 13-year-old male patient presented with headache, nausea, and vomiting that began 4 days prior to his arrival at our emergency clinic. His past medical and trauma history was unremarkable, and no evidence of recent trauma was found on physical examination. Except nausea, vomiting and headache, no other specific neurologic findings were noted. On computed tomography (CT) performed in the clinic, CSDH was observed in the right fronto-temporo-parietal region, and combined AC was discovered in the right midfossa area. He was admitted to our hospital and underwent emergency burr-hole trephination on the right parietal skull area. Follow-up CT performed two days after the surgery revealed complete drainage of CSDH (Figure 1). His condition improved after the surgery without complications, and he was discharged from the hospital 10 days after the operation. However, he visited the outpatient clinic complaining of headache on postoperative day 26. CT was ordered, and recurrent CSDH was diagnosed. Besides headache, no other neurologic symptoms or signs were present. A reoperation was scheduled, and a second burr-hole trephination was performed along the previous burr-hole line. The follow-up CT taken 2 days after the second operation showed near-complete drainage of the recurrent CSDH (Figure 2). On digital subtraction angiography performed on postoperative day 4, a diffuse abnormal vascular stain was identified on the distal part of the right MMA. However, we could not find any abnormal vasculature associated with temporal AC. A microcatheter (SilverSpeed®, Covidien, Plymouth, MN, USA) was placed in the proximal portion of the MMA. Then, MMA embolization was performed with four coils (Tornado®, Cook Incorporated, Bloomington, IN, USA; 3×2 mm, proximal and distal end). The abnormal vascular stain was no longer evident on follow-up angiography (Figure 3). Postoperatively, the patient complained of mild headache with a visual analogue scale of 3, but he complained of no other neurologic complications or symptoms on the day of embolization. The headache also subsided one day after the procedure. He was discharged from our hospital without any symptoms and complications, and no recurrence was found on the follow-up brain CT taken three months after the second operation. Currently, there has been no remarkable clinical finding other than AC during the five years of follow-up.
Discussion
There have been many studies on treatment methods of CSDH, and burr-hole trephination is a generally accepted method for treating primary CSDH.18) Since burr-hole trephination is a simple hematoma draining technique with a high recurrence rate of up to 20%, it is not certain that burr-hole trephination is the best way to treat a chronic CSDH.101116) Many surgical methods, such as removal of the outer membrane with craniotomy, implantation of a reservoir, subdural-peritoneal shunt and burr-hole retrephination have been proposed, but these methods are widely debated and without a defined set of treatment algorithms for recurrent CSDH.691319)
The relationship between CSDH and AC was first reported by Robinson.17) There have been many theories concerning the sporadic occurrence of CSDH combined with AC, such as the elevation of intracranial compressibility by AC causing frequent CSDH even from minor trauma, the occurrence of CSDH from increased fluctuation of CSF flow within the AC with the subsequent rupture of the bridging or intracyst vein, and the prevalence of CSDH due to reduced tolerance to trauma caused by the diminished intracranial cushion effect resulting from the presence of a less compliant AC.414) AC has been considered a risk factor for recurrent CSDH, but the presence of the risk factor is not an appropriate reference for predicting the potential prevalence rate of recurrent CSDH. In our case, the patient underwent two separate operations for primary and recurrent CSDH, but accurate assessment for the recurrence was not possible for either case. Besides having concomitant AC, the patient experienced recurrent CSDH despite having no other known risk factors. Since our review of the literature revealed that having concomitant AC increases the risk of recurrent CSDH,792023) we performed MMA embolization with the second trephination. Angiography is relatively less invasive, like the literature of the above, if the vascular staining is visible, one stage procedure can be proceeded. Therefore, we decided to conduct angiography and embolization.
Tanaka et al.21) discovered three types of vessel-small veins, arteries and capillaries-from the histologic examination of CSDH's outer membrane, and they found that these vessels cross the dura mater and connect to the MMA. Their study became a background for performing MMA embolization in CSDH patients, and Mandai et al.7) reported the first clinically successful treatment of CSDH with MMA embolization in 2000. On the other hand, Kwak et al.5) initially performed burr-hole trephination for primary CSDH combined with AC with good results. However, they stated that in recurrent cases, a more extensive and invasive treatment method involving the subtotal removal of AC and CSDH membranes through craniotomy yielded a better outcome than lesions treated with burr-hole trephination alone. In the present case, we performed MMA embolization instead of the craniotomy, since we considered embolization less invasive than craniotomy. Many previous reports about distal MMA embolization of CSDH suggested that diffuse vascular stainings are the theoretical reason of the procedure.72022) Thus, if there were not abnormal vascular staining lesions of distal MMA branch, we will not have performed our embolization procedure. We would have rather considered about the craniotomy for hematoma and AC removal.
Our patient experienced a good outcome, and this result shows that embolization may be a good alternative therapy for minimizing the recurrence of CSDH combined with AC. However, the role of embolization in minimizing recurrence should be studied further in future studies. Although our patient achieved complete remission without recurrence for three months, it is unclear whether MMA embolization itself was effective in preventing the recurrence, since we performed the embolization soon after the patient underwent repeated burr-hole trephination for recurrent CSDH. However, many studies, including this case report, propose that MMA embolization reduces the recurrence rate of CSDH. Thus, we propose that with a careful review of the patient's medical and drug history, MMA embolization should be considered early in the treatment of patients with combined CSDH and AC to minimize the risk of recurrence, the possibility of repeated burr-hole trephination, and the complications and cost involved in undergoing an additional operation or anesthesia.
Conclusion
MMA embolization could be a useful treatment method in the case of pediatric CSDH with AC. However, since there have been only sporadic case series about the method, a large randomized controlled study is necessary in the future to confirm the efficacy in the treatments of refractory CSDH.
 XML Download
XML Download