

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As more survivors exist who have suffered brain injuries, such as a stroke and traumatic brain injury, the rehabilitation of these survivors has become an important issue. Of the fifty million stroke survivors in the world 25% to 74% are dependent on caregivers for their activities of daily living (ADL) after a stroke [123].
In patients after a stroke, the recovery of ability to conduct ADL affects the quality of life [45]. Ability to perform their own ADL, including eating, grooming, and bathing, is very important for both the patient and the caregiver.
There are several studies about factors that can affect the prognosis of rehabilitation in patients with brain lesions. These includes the extent of brain damage, the initial extent of disability, the extent of the cognitive function damage, the age of onset as well as psycho-environmental factors. Among these, it has been debated which factors would affect the prognosis of rehabilitation, especially predicting ability for the ADL. In addition, identifying subgroups of patients who may benefit most from a particular rehabilitation and stratifying patients into prognostically comparable groups can also be important [67].
In this study, we aimed to discover those factors that may affect ADL after rehabilitation, especially in severely disabled stroke patients. This information would help caregivers and researchers plan and provide effective rehabilitation for post-stroke patients.
MATERIALS AND METHODS
Participants
We did a retrospective analysis of patients admitted to rehabilitation hospitals. The inclusion criteria were: 1) patients who had had a stroke during the preceding 2 years, 2) disabled patients who needed continuous rehabilitation, 3) patients who had received rehabilitation for at least three months, 4) patients who had stable medical conditions, and 5) were participating in an active rehabilitation program.
Any patients with severe aphasia were excluded because the scores on the Korean version of the Mini-Mental State Examination (K-MMSE) scores might not precisely represent their current cognition status. Patients with other severe musculoskeletal disorders were also excluded. This study was approved by the Institutional Review Board (IRB) of Ewha Womans University Medical Center (IRB No.2017-10-059).
Methods
All information was acquired from medical records of patients, retrospectively. The ADL was evaluated with the Korean version of Modified Barthel Index (K-MBI) at the time of admission and after 3 months. During the study period, all patients were evaluated with the K-MMSE at the time of admission.
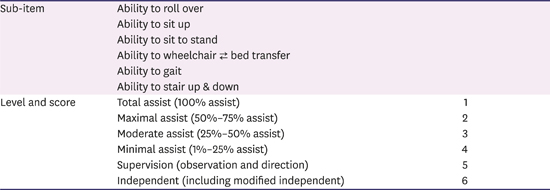
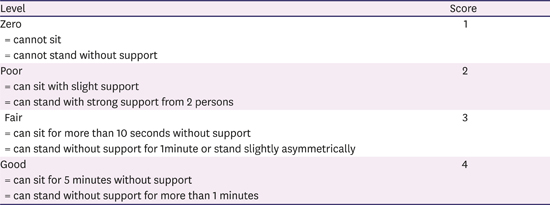
The functional ability (FA), which consists of 8 sub-items, including ability to roll over, sit, stand up, transfer, gait, climbing stairs, sitting balance, and standing balance, was evaluated at the time of admission and at three months after the admission. This assessment used a slight modification of the Postural Assessment Scale for Stroke Patient (PASS) [8], a post-stroke balance assessment tool. The 6 sub-items (ability to roll over, sit, stand up, transfer, gait and climbing stairs) were graded with a range from 1 to 6 (total assist, 1; maximal assist, 2; moderate assist, 3; minimal assist, 4; supervision, 5; independent, 6) (Appendix 1), and the 2 sub-items (sitting balance and standing balance) were scored with a range from 1 to 4 (Zero, 1; Poor, 2; Fair, 3; or Good, 4) (Appendix 2).
To evaluate the effect of age, patients were divided into 2 groups: group A1 and group A2, with the cutoff age of 70; their K-MBI scores were compared. Concerning the duration of disability, the patients were divided into 3 groups: group D1 had a stroke in the past 6 months; group D2 had a stroke within the last 6 and 12 months; and group D3 had a stroke within the past 1 to 2 years. To evaluate the effects of the initial cognitive function, patients were divided into 4 groups based on their K-MMSE score: group M1 had a score between 0 and 9; group M2 had a score between 10 and 19; group M3 had score between 20 and 24; and group M4 had a score between 25 and 30.
Statistics
The SPSS ver. 17.0 (SPSS, Inc., Chicago, IL, USA) was used for the statistical analysis. A p value of less than 0.05 was considered statistically significant. A univariate analysis with a t-test and 1-way analysis of variance was used to compare demographic and baseline information between the groups. A paired t-test was used to compare their ADL before and after treatment. A univariate correlation was done to find those significant factors that could affect the participants' K-MBI scores. A multivariate linear regression with stepwise elimination was done to find the independent factors which can affect K-MBI score.
RESULTS
Sixty-four post stroke patients were included in this study. Their average age was 73.62 ± 10.64 years, and the number of females was 33 (51.6%). The mean duration of stroke was 11.53 ± 5.93 months; 34 (53.1%) patients had a left hemiplegia, 23 (35.9%) patients had a right hemiplegia, and 7 (10.9%) patients had quadriplegia. The causes of stroke were ischemic stroke (n = 51, 79.7%), intracranial hemorrhage (n = 9, 14.1%), and subarachnoid hemorrhage (n = 4, 6.3%) (Table 1).
Table 1
Demographic characteristics of patients at admission to rehabilitation

The mean K-MBI score before the treatment was 30.14 ± 21.12. After 3 months of rehabilitation, the K-MBI score had increased significantly (39.67 ± 23.45). In the K-MBI, the 10 sub-items were significantly improved after 3 months of rehabilitation except for the ambulation item (p = 0.095). The ‘Stair climbing’ sub-item showed less improvement than did other items (p = 0.049) (Table 2).
Table 2
FA and K-MBI assessed at admission and after 3 months
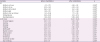
The significant improvement was shown also in all assessments of FA. At the time of admission, the mean score of ability to sit up was 3.30 ± 1.60. After 3 months of rehabilitation, the mean score of ability to sit up was increased to 4.03 ± 1.54, which meant that the patients required only minimal help rather than moderate help for sitting up (Table 2).
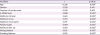
When patients were divided into groups based on their age, both groups showed significant improvement in their K-MBI score after rehabilitation (p < 0.01). Group A1 had significantly more improvement in the K-MBI score than did group A2 (p = 0.144). When patients were divided into groups based on the duration of stroke, all groups showed significant improvement in their K-MBI scores. There was no significant difference between the groups. When patients were divided into groups based on their K-MMSE score, all groups except for group M1 showed significant improvement in their K-MBI scores after treatment. When the improvement of the K-MBI score was compared between groups, it was significantly different between groups (p < 0.005) (Table 3).
Table 3
Score of K-MBI according to the age group, duration of stroke and K-MMSE level at admission and after 3 months rehabilitation

Values are presented as mean ± standard deviation.
K-MBI, Korean version of Modified Barthel Index; K-MMSE, Korean version of Mini Mental State Examination.
*Statistically significant (p < 0.01) in comparison of K-MBI before and after rehabilitation in each group by paired t-test; †Statistically significant (p < 0.005) in comparison of K-MBI before and after rehabilitation in each group by paired t-test; ‡Statistically significant (p = 0.005) between groups by 1-way analysis of variance.
In the univariate analysis, age, K-MMSE group, ability to roll over, sit up, stand up, ambulation, stair climbing, sitting balance and standing balance were significant factors which was associated with the final K-MBI score after 3 months of rehabilitation (Table 4).
Table 4
Pearson correlation coefficients (p value) of K-MBI score after rehabilitation with variables
The multivariate analysis with stepwise elimination showed that the ability to sit up (β = 0.589) and initial K-MMSE (β = 0.360) were significant independent factors affecting the K-MBI score after 3 months of rehabilitation. The final multivariate analysis model was as below (Table 5).
Table 5
Multiple stepwise regression analysis affecting K-MBI score after rehabilitation

| Factors | K-MBI Score after Rehabilitation | ||
|---|---|---|---|
| β | p value | ||
| Ability to sit up | 0.589 | 0.000 | |
| K-MMSE level | 0.360 | 0.000 | |
| R2 | 0.669 | ||
| Adjusted R2 | 0.658 | 0.000 | |
K-MBI score after 3 months of rehabilitation:
DISCUSSION
In this study, improvement of ADL in post-stroke patients who were severely disabled and needed inpatient rehabilitation was achieved after 3 months of rehabilitation, even in those older than 70 or in chronic patient at a year after from onset. In terms of cognitive function, significant improvement in ADL was observed in all patients except for patients with very low cognitive function, such as below 10 in the K-MMSE. In addition, in this study the ability to sit up and the initial K-MMSE scores were independent predictors of ADL outcome after 3 months rehabilitation, with statistical significance.
The predictive value of many clinical determinants for the outcomes of ADL after a stroke has remained unclear. Some studies showed strong evidence for a baseline neurological status, upper-limb paresis, and age as predictors for outcomes of ADL. In addition, gender and risk factors of a stroke such as atrial fibrillation were not associated with functional outcome [9]. However, those studies focused on the early post-stroke phase for the final ADL. They included studies conducted 2 weeks or less after the stroke onset and evaluated the final outcome of ADL 3 months post-stroke, thus limiting their application to subacute and chronic periods. So, we studied the recovery of ADL for the period of 24 months post-stroke.
In this study, the ability of daily living activities was improved after rehabilitation in all age groups, even in those over 70 years, though the improvement of ADL was significantly greater in the group under 70 years. Some previous studies have shown that older people who are stroke patients have poor functional outcomes after rehabilitation [10111213]. Nevertheless, other previous studies explained that functional improvement can be achieved in the elderly [14151617]. O'Brien and Xue [18] also showed functional benefits in elderly patients over 85 years of age who were admitted to an inpatient rehabilitation facility for post care of a stroke. Considering the results of the previous studies, our study implies that elderly patients in an aging society should be actively rehabilitated to improve their daily activities. On the other hand, our age-classification criteria of the group was 70 years old; the cutoff is usually 65 or 75 years old in concurrent studies. In future study, consideration of the patients' age range or use a continuous-variable analysis would be needed.
It is well known that improvements in disability and impairment measurements occur during the first month, and there is still considerable room for improvement in the following 3 months. It also has been reported that most people get the maximum improvements on the score for the basic ADL in the first year after the onset of a stroke [19]. However, our study showed that ADL and functional status kept improving when the patient continued rehabilitation even after a year or two past the stroke onset. Such a result implies that chronic patients who had had a stroke more than a year should continue rehabilitation to further improve their independent daily activities.
One factor affecting ADL after rehabilitation is the initial K-MMSE score in this study. The previous study shows that cognitive impairment was significant and an independent factor associated with functional outcome in post-stroke patients. [14202122] Oneş et al. [12] reported that there was a significant positive association between Mini-Mental State Examination (MMSE) at admission and the functional discharge measure. They compared patients with a MMSE score of 24 or below to patients with a score above 24 for their total functional improvement; there were significant differences between the 2 groups. Also, Massucci et al. [20] reported that an MMSE score ≥ 24 was significantly associated with independent gain (Barthel Index score ≥ 18). Han et al. [22] compared the initial MMSE score with the Modified Barthel Index (MBI) score at the beginning of rehabilitation and at discharge. They concluded that the initial MMSE scores correlated well with the functional outcome of stroke patients, especially on the memory and language sub-items. They divided participants into 3 groups according to their initial MMSE score, low (19 or less), middle (20 to 25), and high (26 or more). In our study, we subdivided the lower K-MMSE group into 2 groups, less than 10 and 10 to 19, to assess patients with severe cognitive decline. Jakavonytė-Akstinienė et al. [23] also reported that the degree of cognitive impairment according to the MMSE scale (age and education are not considered) is as follows: 21–24 points, mild cognitive dysfunction; 11–20 points, moderate cognitive dysfunction; 0–10 points, severe cognitive dysfunction [2425]. Our study results show that the patients with a K-MMSE score of 10 or greater showed improvements in ADL after 3 months of rehabilitation, whereas those with very severely impaired cognition, having a K-MMSE score of less than 10, did not do as well.
In the univariate analysis, age, K-MMSE, ability to roll over, sit up, stand up, ambulation, stair climbing, sitting balance and standing balance were significant factors which was associated with K-MBI score after 3 months of rehabilitation. The multivariate analysis of this study showed that the initial cognitive function, which was assessed by K-MMSE and the ability to sit up were both significant independent factors affecting the ADL outcomes after 3 months of rehabilitation. In previous study, it was revealed that standing up from a seated position was one of the most frequently performed functional tasks, and it was an essential pre-requisite to walking. Also, it was thought that the ability to stand up without assistance is important for independent living [2627]. In the current study, however, to conduct ADL ability, sitting up was more important than standing up, perhaps because the subjects included in this study were relatively severely disabled patients who required rehabilitation for more than 3 months and who could not walk independently. This is related to changes in the components of the K-MBI after three months of rehabilitation, and is why other components showed significant improvements, but the ‘walking’ category did not. Among the components, the improvement of ‘stair up’ was also statistically significant. However, the pre- and post-rehabilitation scores showed 0 on the point scale, so there seemed to be almost no functional differences. Therefore, in a relatively severe disability group requiring in-patient rehabilitation, ‘sit up’ is more important than ‘stand up’ as a factor that affects the daily living activities.
The significance of sitting and standing up in functional outcome may be consistent with previous studies, that the training of core stability and trunk balance leads to a significant improvement in mobility and the ADL in subacute post-stroke patients [28]. This is because the anticipatory postural adjustments of trunk muscles play a major role in maintaining antigravity postures like sitting and standing when a reaching task is executed [29]. In addition, recent evidence supports the idea that the trunk control test and the Trunk Impairment Scale were important predictors for functional outcome at discharge after a stroke [27303132].
This study has several limitations that should be noted. First, we used only one tool, the K-MBI, to measure the improvement in daily activities. If we could have used 2 or more measurements, a better outcome would have been found. In addition, the more variables predicting functional outcomes such as severity of stroke at admission, neglect, nutritional status or depressive mood could be included in future studies. A patient with aphasia, as a factor affecting ADL, had been excluded from the current study for exact evaluation of cognitive function, but it should be considered in following studies. Also, the measurement of FA was not a validated tool, although it was similar to PASS. In future studies, a validated tool should be used to properly assess FA. Finally, it is common to set a cutoff value of 70 for age, so future studies should use a standard category for age or could consider statistical analysis of age as a continuous variable. This study showed that regardless of age or duration of stroke, the ADL outcomes were improved after 3 months of rehabilitation in post-stroke patient, especially in patient with an initial K-MMSE score of more than 10. Therefore, active rehabilitation could also be needed in patients older than 70, chronic patients after a year from onset, and patients with impaired cognitive function. Furthermore, the ability to sit up should be evaluated thoroughly, since it is an independent factor along with the K-MMSE score, which can predict the ADL after rehabilitation in severely disabled post-stroke patient. These results imply the importance of sitting-up exercises in ADL rehabilitation. Any patients with an K-MMSE score of more than 10 needs more attentive ADL training.
 XML Download
XML Download