

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Decreased saturation level of blood oxygen in the acute and subacute phase of stoke might damage the ischemic penumbra and worsen clinical outcome [1]. Furthermore, patients with acute and subacute stroke frequently develop arterial oxygen desaturations. There is even a research that continuous monitoring is needed to detect drop oxygen saturation and to titrate oxygen administration for the stroke patients [2]. For that reason, there have been many studies that considerable differences in oxygen saturation are seen at the time before and after insertion of nasogastric tube, changes of body position, before, during, and after meals, and sleep-disordered breathing [34567]. The data of studies above were measured by portable pulse oximeters, in addition to its limitation toward carboxyhemoglobinemia and/or methemoglobinemia, its accuracy toward the old is getting unreliable [8].
Therapeutic exercise is important in rehabilitation of stroke patient however, there has been a lack of study how the oxygen saturation is changing before, during and after the exercise. For that reason, we directly analyzed metabolic state and changes of oxygenation (O2 saturation, PaO2, PaCO2, O2 content, HCO3−, pH, and anion gap) via arterial blood gas analysis (ABGA) in pre- and post-exercise status for acute and subacute stroke patients. Moreover, we examined the changes above were correlated with age, the time after stroke onset, and the severity of stroke.
MATERIALS AND METHODS
This research was approved by the Institutional Review Board of Kwangju Christian Hospital, and carried out at a single medical center. All the subjects were recruited prospectively, and the documents of written informed consent were obtained. The subjects were post-stroke of non-brainstem lesion patients within 24 months of onset. Patients were excluded if: 1) the stroke lesion involved around brainstem; according to the preliminary study that brainstem stroke patients used to experience hypoxia even under the resting state so they do not follow the instructions that we planned exercise protocol, 2) onset was over 24 months prior to assessments, 3) considerable cardiopulmonary diseases (e.g., coronary artery disease, valvular heart disease, chronic obstructive pulmonary disease, asthma, pneumonia, and lung cancer). In order to evaluate unnoticed diseases, all subjects were checked by electrocardiography, 2-dimensional transthoracic echocardiography, chest multidetector computed tomography, and pulmonary function test.
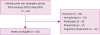
From January 2016 to May 2016, 85 hospitalized subjects were first enrolled to the study though, 12 subjects of atrial fibrillation and other arrhythmias, 8 subjects of atelectasis, 3 subjects of pneumonia, and 10 subjects of cognitive impairment who were not able to follow exercise instructions were excluded. Finally, 52 subjects were participated in this study (Fig. 1).
The maximal heart rate (HRmax) = 220 − age formula was used to objectify the moderate exercise intensity, monitored by pulse oximetry (SPO 7500; SPO medical, Simi Valley, CA, USA) to maintain 70% of HRmax during exercise [91011]. 20 minutes of stationary cycling with resistance (ShinGwang 3000; SGMED, Seoul, Korea) (Fig. 2) is commanded for the exercise under the supervision of physicians not to be strayed from the protocol mentioned above. Moreover, 5 minutes of non-resistant pedaling was done on pre- and post-cycling by for the warm ups and cool downs.
Fig. 2
Exercise of moderate exercise intensity by stationary cycling with resistance (ShinGwang 3000; SGMED, Seoul, Korea).

ABGA and vital signs (blood pressure, pulse rate, and respiratory rate [RR]) were measured by physicians 10 minutes prior to exercise, and 10 minutes after the exercise, those were rechecked by the same physicians in the same way. ABGA was performed by collecting blood from a single arterial puncture [12], and subjecting it to analysis on a blood gas analyzer (pHOx Ultra; NOVA Biomedical, Boston, MA, USA) (Fig. 3). All the machines and devices were regularly followed by standard quality control measures. Statistical analysis was performed using the SPSS ver. 21.0 software program (IBM SPSS Inc., Armonk, NY, USA). A paired t-test, Pearson correlation analysis, and one-way analysis of variance (ANOVA) were done to assess the effectiveness and the difference between pre- and post-exercise. A p value of < 0.05 was regarded as statistical significance.

RESULTS
Table 1 presents demographic and clinical information for the 52 patients. The study group was composed of 27 men and 25 women.
Table 1
Demographics and clinical characteristics of subjects (n = 52)

| Demographic factors | Value | |
|---|---|---|
| Age (yr) | 60.40 ± 15.13 | |
| Sex (male:female) | 28:24 | |
| Stroke etiology | ||
| Ischemic:hemorrhagic | 30:22 | |
| Onset (mon) | 5.84 ± 5.09 | |
| Cortical:subcortical | 27:25 | |
| NIHSS | 12.51 ± 6.92 | |
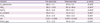
Table 2 presents the changes of O2 saturation, PaO2, PaCO2, O2 content, HCO3−, pH, and anion gap between pre- and post-exercise. O2 saturation, PaO2, O2 content, anion gap, pulse rate, and RR were increased, PaCO2 and HCO3− were decreased, and pH was not changed. There was statistical significance on both the increase of O2 saturation, PaO2, anion gap, pulse rate, and RR and the decrease of PaCO2 and HCO3−. Moreover, increase of O2 content showed significance (p = 0.001) however, change of pH was not revealed meaningfulness (p = 0.255).
Table 2
Changes of O2 saturation, PaO2, PaCO2, O2 content, HCO3−, pH, and anion gap between pre- and post-exercise (n = 52)
Then, we analyzed the data changes with age and the time after stroke onset in Pearson correlation. As age more increased, we found more decreased HCO3− (correlation coefficient r = 0.450, p = 0.001) and more increased RR (correlation coefficient r = 0.432, p = 0.001) (Fig. 4). Those were revealed statistical significance.
Fig. 4
(A) The decrease of HCO3− (mEq/L) and (B) the increase of RR (breaths per minute) were proportional to age.
RR, respiratory rate.

The patients were classified into the 3 group on the basis of National Institutes of Health Stroke Scale (NIHSS) as having very severe neurologic impairment (NIHSS > 25: the group was excluded due to cognitive impairment not to follow the exercise protocol), severe impairment (NIHSS 15–24: group A), mild to moderately severe impairment (NIHSS 5–14: group B), and mild impairment (NIHSS < 5: group C) [13]. Therefore, we studied that measured data changes (O2 saturation, PaO2, PaCO2, O2 content, HCO3−, pH, anion gap, blood pressure, pulse rate, and RR) after the exercises were correlated with each group through one-way ANOVA. There was not statistical significance between stroke severity and the data changes.
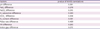
In addition, there were not statistical significance between NIHSS and the data (O2 saturation, PaO2, PaCO2, O2 content, HCO3−, pH, anion gap, blood pressure, pulse rate, and RR), either (Table 3).
Table 3
The correlations of between NIHSS and the pH, PaO2, PaCO2, O2 saturation, HCO3−, O2 content, pulse rate, RR, and anion gap
DISCUSSION
Whole animal and in vitro studies indicate that ventral and dorsal respiratory group on medulla oblongata and pneumotaxic center on pons regulate respiration according concentrations on chemoreceptors of CO2 and hydrogen ions, those are distributed throughout the brainstem [14]. Peripheral chemoreceptor system is also involved in respiration by detecting lack of O2 on carotid and aortic bodies, then it makes respiration center in brain excited [15]. In this study, we excluded the patients with brainstem lesions in computed tomography and magnetic resonance imaging.
Nevertheless, some studies reported that respiration center is not only controlled by brainstem, but also regulated by other brain area [161718]. Accordingly, we hypothesized that even the patients with other brain lesions (cortex, basal ganglia, cerebellum, and any lesions other than brainstem) were decreased respiratory control reaction during exercise. The goal of this study was to figure those things out.
In the healthy athlete, arterial PO2, PCO2, O2 saturation, pH, and anion gap remain almost exactly normal during strenuous exercise [15]. Our patients (non-brainstem stroke) were not strayed from normal ranges [19] before and after the exercise, either. There are several possible explanations for it. First, adaptation or neuroplasticity of respiratory center on brainstem to decreased signal of it. Several studies reported that the neuroplasticity of respiratory center on brainstem [20], even if signal decreased or absent from other brain areas to respiratory center on brainstem, it is supposed compensatory neuroplasticity occurred to maintain respiratory homeostasis. Second, we guess that carotid and aortic bodies increase its respiratory drive by detecting decreased oxygen level [21]. It is statistically significant that the increase of RR after the exercise of our patients. Among 52 patients, 5 of them, relatively lower scores of NIHSS with higher physical functions, did not show the increase of RR after the exercise. We assume that further study is needed by setting healthy people as a control group.
We excluded the patients with cognitive impairment not to follow the exercise protocol before we had initiated this study. They were mainly NIHSS > 25 that the effects of the exercise may not be objectively evaluated. Besides, patients with history of considerable cardiopulmonary diseases were also excluded. Therefore, it is not reasonable that our results may be extended to the patients with brainstem disorders and/or cardiopulmonary diseases.
We deduce the decrease of HCO3− was the result of buffering effect toward increased lactic acid after the exercise. Consequently, respiratory alkalosis, we observed through the increase of PaO2 and the decrease of PaCO2, and metabolic acidosis, caused by the increase of lactic acid (increased anion gap) were counterpoised each other and maintained normal range of pH. We supposed that this buffering system was considered properly activated in non-brainstem stroke patients.
It was interesting that as age more increased, more decreased HCO3− and more increased RR were seen. It may be explained that age more increase, the exercise ability is more decrease that makes lactic acid production and RR more increase.
The limitations of our study were that the lack of parametric approach toward each subgroup of brain lesions, the 10 minutes before and after the blood ABGA might not reflect real-time blood status, and lack of data toward direct measurements of carboxyhemoglobin or methemoglobin.
In conclusion, statistically significant results were observed in the change of O2 saturation, PaO2, PaCO2, O2 content, HCO3−, pH, and anion gap 10 minutes before and after the exercise of moderate intensity for the non-brainstem stroke patients, and the data were not strayed from normal ranges. Only increase of HCO3− and decrease of RR were proportional to increase of age, whereas age, the time after stroke onset, and the scores of NIHSS were not correlated with the aforementioned statistically significant results. These suggest that it is relatively well preserved that the respiratory compensation to maintain metabolic homeostasis for the non-brainstem stroke patients.
 XML Download
XML Download