

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dong-Hee Kim, M.D., Ph.D.*, § , Jae Hoon Jang, M.D.†, Myungji Shin, M.D.‡, Gu-Hee Jung, M.D., Ph.D.‡, §
, Jae Hoon Jang, M.D.†, Myungji Shin, M.D.‡, Gu-Hee Jung, M.D., Ph.D.‡, §
, Jae Hoon Jang, M.D.†, Myungji Shin, M.D.‡, Gu-Hee Jung, M.D., Ph.D.‡, §
Abstract
The fixation methods that can be used for unstable posterior pelvic ring injuries have undergone many innovative changes due to the recent development of surgical and imaging techniques. After understanding the appropriate indications of first and second sacroiliac screw fixation and spinopelvic fixation, innovative methods, including the trans-sacral screw fixation, posterior tension-band plate fixation, and the S2AI screw, would be chosen and applied. Considering the anatomical complexity and proximity to the surrounding vessels and nerves in the posterior fixation, the safe zone according to the fixation options should be well understood in preoperative planning. Moreover, the functional reduction of the posterior pelvic ring through the reduction and fixation of the anterior lesion should be achieved before placing the implant to reduce the number of malposition-related complications.
Figures and Tables
Fig. 1
(A, B) Sacral dysmorphism represents the acute angulation of sacral ala and reduced the corridor for iliosacral screw fixation. *Cortical perforation of screw.

Fig. 2
(A) Posterosuperior corners of sacrum were connected by imaginary line. Asterisks: body of 1st sacrum. (B) The virtual cylinder for ilio-sacral screw was placed according to the curve point. (C) the curve point could be visualized easily without additional support.

Fig. 3
(A) Lateral radiographs showed the safe zone of 1st and 2nd sacrum. (B, C) The conventional ilio-sacral screw was placed toward the opposite corner of superior endplate.

Fig. 4
(A–C) The trans-sacral trans-iliac screw should be placed transversely just below the ICD line. (D, E) The entry point was placed just anterior to the curve point. (F, G) The screw did not pierce the cortex around the sacral canal and foramen.

Fig. 5
(A) Unstable pelvic ring injury in a 20-year-old male showing the involvement of spinal canal and comminution of upper sacral surface. (B) The trans-sacral trans-iliac screw was performed after the anterior fixation for achieving the functional reduction of sacrum. (C) The radiographs after 12 months showed neither a loss of reduction nor screw back-out.

Fig. 6
(A, B) The variable of basal height could be measured using the three-dimensional biplanar image in the opposite side.

Fig. 7
(A, B) The safe zone of the 2nd sacrum can be observed easily in the lateral radiographs of pelvis and increased inversely according to the sacral dysmorphism.
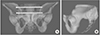
Fig. 8
(A–C) A 63-year-old male sustained an unstable pelvic injury with spino-pelvic dissociation. (B, C) The spino-pelvic fixation was performed and showed the iliac screw, which was used with the connecting rod. (D) The radiograph after 12 months showed the maintenance of pelvic ring.

Fig. 9
(A–C) S2 alar-iliac (S2AI) screw should be toward the AIIS and passed just over the superior rim of the greater sciatic notch, above the greater sciatic notch. (D) The screw trajectory was from the dorsal cortex of the sacrum to the inner ilium by penetrating the sacro-iliac joint.

Fig. 10
(A) A 57-year-old male sustained an unstable pelvic injury with L5 body fracture. (B) First, the pedicle screw of L4 and L5 was placed percutaneously and made the entry portal for the S2 alar-iliac (S2AI) screw. (C) The postoperative radiographs showed the functional reduction of the pelvis. (D) Follow-up radiographs at eight weeks showed the maintenance of reduction adequacy.

Fig. 11
(A) A 71-year-old female sustained of an unstable pelvic injury (sacral fracture). (B–D) The PTB plate fixation was performed and the osseous corridor was used to achieve the maximal screw length. (E–H) The postoperative radiographs showed an acceptable reduction of the pelvis. (I) The follow-up radiographs at 12 months showed the maintenance of reduction.

References
1. Wong JM, Bucknill A. Fractures of the pelvic ring. Injury. 2017; 48:795–802.

2. Gardner MJ, Morshed S, Nork SE, Ricci WM, Chip Routt ML Jr. Quantification of the upper and second sacral segment safe zones in normal and dysmorphic sacra. J Orthop Trauma. 2010; 24:622–629.
3. Routt ML Jr, Simonian PT, Agnew SG, Mann FA. Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: a cadaveric and clinical study. J Orthop Trauma. 1996; 10:171–177.
4. Kleweno C, Bellabarba C. Lumbopelvic fixation for pelvic fractures. Oper Tech Orthop. 2015; 25:270–281.
5. Jeong JH, Jin JW, Kang BY, Jung GH. Can the possibility of transverse iliosacral screw fixation for first sacral segment be predicted preoperatively? Results of a computational cadaveric study. Injury. 2017; 48:2074–2079.
6. Miller AN, Routt ML Jr. Variations in sacral morphology and implications for iliosacral screw fixation. J Am Acad Orthop Surg. 2012; 20:8–16.
7. Kwak JM, Heo S, Jung GH. Successful use of fluoroscopic inlet and outlet views to verify safe screw trajectories when placing Percutaneous iliosacral screws. Med Case Rep J. 2018; 103:7–9.
8. Routt ML Jr, Simonian PT, Mills WJ. Iliosacral screw fixation: early complications of the percutaneous technique. J Orthop Trauma. 1997; 11:584–589.
9. Ziran BH, Wasan AD, Marks DM, Olson SA, Chapman MW. Fluoroscopic imaging guides of the posterior pelvis pertaining to iliosacral screw placement. J Trauma. 2007; 62:347–356. discussion 356.
10. Conflitti JM, Graves ML, Chip Routt ML Jr. Radiographic quantification and analysis of dysmorphic upper sacral osseous anatomy and associated iliosacral screw insertions. J Orthop Trauma. 2010; 24:630–636.
11. Sagi HC, Lindvall EM. Inadvertent intraforaminal iliosacral screw placement despite apparent appropriate positioning on intraoperative fluoroscopy. J Orthop Trauma. 2005; 19:130–133.
12. Kim JW, Oh CW, Oh JK, et al. The incidence of and factors affecting iliosacral screw loosening in pelvic ring injury. Arch Orthop Trauma Surg. 2016; 136:921–927.
13. Gardner MJ, Routt ML Jr. Transiliac-transsacral screws for posterior pelvic stabilization. J Orthop Trauma. 2011; 25:378–384.
14. Wolinsky P, Lee M. The effect of C-arm malrotation on iliosacral screw placement. J Orthop Trauma. 2007; 21:427–434.
15. Mendel T, Noser H, Wohlrab D, Stock K, Radetzki F. The lateral sacral triangle--a decision support for secure transverse sacroiliac screw insertion. Injury. 2011; 42:1164–1170.
16. Chon CS, Jeong JH, Kang B, Kim HS, Jung GH. Computational simulation study on ilio-sacral screw fixations for pelvic ring injuries and implications in Asian sacrum. Eur J Orthop Surg Traumatol. 2018; 28:439–444.
17. Wagner D, Kamer L, Sawaguchi T, et al. Critical dimensions of trans-sacral corridors assessed by 3D CT models: relevance for implant positioning in fractures of the sacrum. J Orthop Res. 2017; 35:2577–2584.
18. Yeo KH, Moon NH, Ahn JM, Jeong JY, Jang JH. Surgical outcome of posterior pelvic fixation using S1, S2 screws in vertically unstable pelvic ring injury. J Korean Fract Soc. 2018; 31:9–17.
19. Elder BD, Ishida W, Lo SL, et al. Use of S2-alar-iliac screws associated with less complications than Iliac screws in adult lumbosacropelvic fixation. Spine (Phila Pa 1976). 2017; 42:E142–E149.
20. Andrade NS, Okafor L, Neuman BJ. Novel technique for sacral alar-iliac (S2AI) fixation. Clin Spine Surg. 2018; 31:373–376.
21. Shabtai L, Andras LM, Portman M, et al. Sacral alar iliac (SAI) screws fail 75% less frequently than iliac screws in neuromuscular scoliosis. J Pediatr Orthop. 2017; 37:e470–e475.
22. Jeong ST, Park YS, Jung GH. Computational simulation of sacral-alar-iliac (S2AI) screw fixation of pelvis and implications for fluoroscopic procedure: a cadaver study. J Orthop Surg (Hong Kong). 2019; 27:2309499019836246.
23. O'Brien JR, Yu WD, Bhatnagar R, Sponseller P, Kebaish KM. An anatomic study of the S2 iliac technique for lumbopelvic screw placement. Spine (Phila Pa 1976). 2009; 34:E439–E442.
24. Yamada K, Higashi T, Kaneko K, Ide M, Sekiya T, Saito T. Optimal trajectory and insertion accuracy of sacral alar iliac screws. Acta Orthop Traumatol Turc. 2017; 51:313–318.
25. Sponseller PD, Zimmerman RM, Ko PS, et al. Low profile pelvic fixation with the sacral alar iliac technique in the pediatric population improves results at two-year minimum follow-up. Spine (Phila Pa 1976). 2010; 35:1887–1892.
26. Acklin YP, Marco G, Sommer C. Double locking plate fixation of sacral fractures in unstable pelvic ring C-type injuries. Oper Orthop Traumatol. 2015; 27:74–79.
 XML Download
XML Download