

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As populations are aging, the cost and implications of osteoporotic fractures are increasing.[1] A diagnosis of osteoporotic fracture is defined as a fracture occurring at a site associated with low bone mineral density (BMD), but BMD might not fully capture the osteoporotic fracture risk.[2] The conventional way of diagnosing and treating osteoporosis using BMD is also limited by its subjective properties and the expected time span needed in order to detect changes.[3]
Numerous bone turnover markers (BTMs), products of bone cell activity, have been developed and this has led to a marked improvement in drug development for osteoporosis and to the understanding of fast bone losers.[4] They are generally subdivided into three categories: bone resorption markers (BRMs), bone formation markers (BFMs), and osteoclast regulatory proteins. Biochemical BTMs have long been used because of their attractive features (easy sample and a variety of assays) to complement the radiological assessment of patients, and their implementation in clinical practice has been helpful in the selection of optimal treatment.[5678] However, there are uncertainties for their routine use due to the inherent limitations, including large variability between individuals, age, physiological maturity, and multiple methodologies used for analysis.[9]
The aim of this paper is to review the clinical effectiveness of BTMs in the management of osteoporotic fracture, in terms of 1) fracture risk prediction; and 2) prediction of non-union fractures.
CONTRIBUTION OF BTM TO THE ESTIMATION OF RISK OF PRIMARY OSTEOPOROTIC FRACTURE
In general, many postmenopausal women at risk of fractures are assessed according to their risk based on BMD assessment alone or fracture-risk assessment tool (FRAX).[210] However, BMD measured by dual energy X-ray absorptiometry (DXA) or FRAX cannot detect all osteoporotic fractures, so several tools have been developed to improve the assessment of individual risk of major osteoporotic fracture in elderly patients.[1112] In patients who were not diagnosed with osteoporosis by DXA, but suffered from fragility fractures, an irregular endosteal margin with semilunar defects were detected by high-resolution peripheral quantitative computed tomography.[131415] Increased endosteal remodeling will impose structural damages due to trabecular thinning, disappearance and loss of connectivity, cortical thinning, and increased intracortical porosity.[16] This cellular activity can be estimated by biochemical bone BTMs, thus, it is possible to consider that the level of BTMs might predict fracture and such prediction may improve if BTMs are assessed along with BMD and other factors.[17]
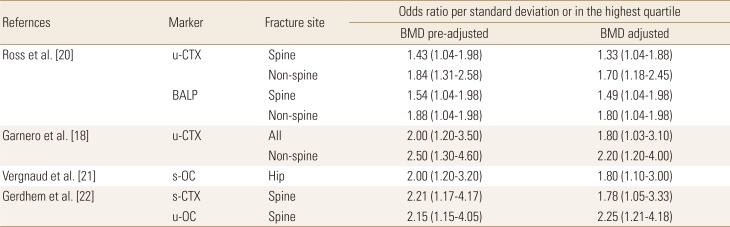
Several prospective studies have reported the presence of increased BRMs as having an additive effect on fracture risk in women with a low BMD. Representative studies are the EPIDOS [5] and OEFLY studies [18] which found a significant relationship between the values of BRMs and the risk of osteoporotic fractures in large populations. Women with both a femoral BMD value of 2.5 standard deviation (SD) or less, and either high C-terminal telopeptides of type I collagen (CTX) or high free deoxypyridinoline (DPD) levels, were at greater risk of hip fracture, with an odds ratio of 4.8 and 4.1, respectively, than those with only low BMD or high bone resorption among 126 female hip fracture patients.[5] Similarly, the contribution of urinary CTX (u-CTX) to hip fracture probability and its independence from BMD was reported.[19]
The predictive value of BTMs appears to be independent of bone mass in that the risk persists even after adjustment for BMD (Table 1).[18202122] These studies indicate that indices of BTMs give information on fracture risk independently of BMD and might therefore complement and augment fracture risk assessment by BMD. Additionally, the risk of fracture might be predicted using a combination of history of fractures and BTM, if DXA is not available.[18]
Although several long-term prospective studies show that combining BMD and BTMs may be useful for improving the assessment of osteoporotic fracture risk, some study results do not support the routine use of BTM to assess fracture risk. Higher bone turnover was associated with faster cortical and trabecular bone loss at the proximal femur but not with fracture risk in these studies.[2324] From a pathophysiological point of view, in addition to BMD, other factors may also contribute to bone fragility during aging, including osteocyte deficiency, changes in matrix composition, and increased fatigue damage.[1325] In given studies which showed significant association, too many different BTMs and different fracture sites such as spine, hip, non-spine, and all fractures, were investigated, which raises the possibility of false positive results.
The most relevant criticism is that there is difficulty in the clinical use of BTM in terms of the predictive value of BTMs. In many studies, a common approach to statistical analyses with results is expressed as odds ratio per SD of increase in BTM, e.g., the risk of fracture in those with high measurements is compared with that in patients with lower values. For example, in one study, the risk of hip fracture increased by 1.4 for each 1 SD increase in urinary free DPD and by 1.3 for u-CTX.[18] However, the use of odds ratios is not ideal for clinical decision-making in predicting fractures. This is because such analyses studied a proportion of the population in each cohort so the results cannot be applied to the general population.
For this reason, further researches are needed in this regard. First, the measurement of absolute risks, such as 10-year probabilities, are appropriate for future studies. One study using a Swedish Patient Register demonstrated ten- and 15-year risks for all types of osteoporotic fractures that can be used for decision-making to illustrate a means for transforming information from odds ratios to probabilities.[26] Second, uncertainties over the clinical use of BTMs can be resolved in part by adopting international reference standards. Collaborative efforts are ongoing in order to standardize their measurement as appropriate and for reporting values.[27] Recently, the International Osteoporosis Foundation (IOF) and the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) have designated procollagen type I N-terminal propeptide (PINP) and serum βCTX (s-βCTX) in blood as reference standard for BTM.[2728]
FOR EARLY DETECTION OF FRACTURE HEALING DISTURBANCES
The diagnosis and follow-up of nonunion rely predominantly on the interpretation of radiologic findings; however, it is not early detection but is just a diagnosis, which is established only after several months' post-injury.[29] The development of additional methods to monitor bone healing is therefore needed in clinical practice. During the fracture healing process, an earlier increase in BRMs generally occurs after the fracture, due to the osteoclastic removal of the necrotic tissues and a subsequent increase in BFMs derived from the osteoblastic activity, which are formed during the different stages of osteoblast proliferation.[30] BTMs are easy to measure and the changes in biomarker levels can be detected earlier than changes in bone mass and density.[31] Thus, many studies investigated whether the BTMs are useful as a supplemental or replacement diagnostic method in monitoring the fracture healing process.
With regard to molecules that regulate the function of osteoclasts, early changes in BRMs could reflect the initial process of successful fracture healing and may be used in clinical practice to monitor the healing process.[3233] Tartrate-resistant acid phosphatase 5b proved to be one of the most promising markers of bone resorption was significantly decreased in the 4th and 8th week of delayed healing group among 248 long bone fracture patients.[32] Similarly, a large difference in serum osteoprotegerin levels was observed between patients who had developed an atrophic non-union and those that had progressed towards normal fracture healing.[33] However, other BTMs including CTX, N-terminal telopeptides of type I collagen (NTX), DPD which also indirectly determine the osteoclast activity were not lower than the normal healing group in these studies. These imbalances in BRMs suggest that there was no inhibition of osteoclastic activity in impaired union patients.
Several studies had investigated the effect of BMD on the change of BRM during fracture healing.[343536] The levels of NTX, CTX and DPD during fracture healing in osteoporotic patients showed significantly higher during fracture healing despite low BMD compared to non-osteoporotic patients.[3436] This is different from our general thinking that low BMD results in decreased levels of bone markers during fracture healing and might suggest that preexistent elevated bone turnover in patients with osteoporosis. In addition, the concentration of BRM is higher in females than males/in hip fractures than in other fractures.[343637] Therefore, the relationship between patient's various factors and the level of BRM remains unclear.
BFM, including bone alkaline phosphatase (BALP), osteocalcin (OC), PINP and carboxy-terminal propeptide of type I procollagen (PICP) are expected to be capable of reflecting the healing process.[38] The serial measurement of BFM concentration showed their potential following human studies in patients with tibial or femoral shaft fractures.[7394041] One study showed lower levels of BALP in patients with delayed union at an early time point during the fracture healing process compared to patients with normal bone union at the 4th week after the fracture occurrence.[7] In a poor healing response in tibial shaft fractures, there is serological evidence of deficient osteoblast response, as indicated by normal levels of BALP and PICP.[41] One recent prospective observational study of 168 patients with tibial fractures showed significantly lower levels of BALP, OC, and PINP in patients with delayed union.[40] One study suggested that PINP is more reliable BFM in reflecting bone formation processes when compared with other markers (PICP, ALP, and OC) because PINP shows minimal diurnal variation.[42]
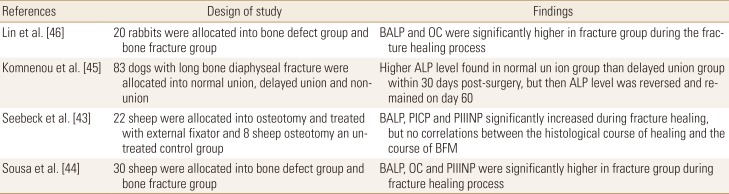
However, the evidence that we can use biochemical markers of bone turnover in the prediction of nonunion is still less convincing. Nevertheless, evidence form animal experiments still differ between studies (Table 2).[43444546] Additionally, one of the major limitations of some of these studies is the loss of statistical power because the included patients number was too small, and the results were mainly related to the small number of patients included in each group.[73441] Apart from the variety of bone markers, the site of fracture and the degree of fracture stability still too heterogeneous between studies. Many confounding factors may affect bone healing (e.g., age, gender, ethnicity, smoking status, and other comorbidities), hampering the comparison of the results between different laboratories.
CONCLUSION
This review supports the role of BTM in the prediction of future fractures. We believe that the relationship between BTM and fracture risk improves the prognostic approach and we might be able to include BTMs in our fracture prediction models. The adoption of reference analyses and standardization of their measurement would assist in the accumulation of trial data on BTMs in order to expedite their incorporation into clinical practice. Although BTM levels are possibly being associated with the different stages of the bone fracture healing process, their clinical effectiveness in predicting impaired fracture healing processes at an early stage is unclear. More work is needed to enhance the use of BTM, with an ongoing collaboration between the laboratory and clinical professions.
 XML Download
XML Download