

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of metabolic syndrome (MS) is increasing worldwide, and it can create a burden on national economies. In South Korea, MS has increased significantly from 23.6% in 1998 to 28.0% in 2001.[1] However, currently, it has trend to decrease to 18.8% according to a report of the Ministry of Health and Welfare in Korea.[2] Although there are a number of risk factors, such as age, obesity, smoking, dietary habits, and exercise, that affect MS as a predictor of cardiovascular disease, low skeletal muscle mass related to a high prevalence of cardiovascular disease emerged as a spotlighted factor among them.[3]
Menopause-related hormonal changes influence the redistribution of body fat and the loss of muscle mass and strength, independently of aging.[45] Menopause is clinically defined as a cessation of menstruation entirely for 1 year, which is reported to occur, on average, in Korean women in their fifties. Women generally tend to gain weight (Wt) due to sudden hormonal changes.[6]
Hence, low skeletal muscle mass and high fat mass may have a synergistic impact on both metabolic impairment and physical disability,[7] especially in postmenopausal women.
Given the scarcity of studies about the relationship between sarcopenic obesity (SO) and MS in postmenopausal women, Lim et al.[8] suggested that SO was more closely associated with MS in women aged 65 or older. This was measured by dual energy X-ray absorptiometry (DXA) scans (Hologic Inc., Bedford, MA, USA). In contrast, Peppa et al.[9] investigated the traditional belief that lean body mass without fat and bone mass is favor associated with cardiometabolic risk factors in healthy postmenopausal women. It was found that women with a high arm lean mass index (LMI) displayed a significantly higher prevalence of MS compared to women with a low arm LMI when the central fat distribution was taken into consideration. Therefore, emerging evidence has shown that the relationship between SO and MS in postmenopausal women clearly was yet to be established.
In the present study, according to the recent interest in health and various dietary behaviors in the elderly, we in-vestigated the prevalence of sarcopenia and SO in Korean women with the natural decline of estrogen during the menopausal period and its relevance to MS, and whether there are significant changes after controlling multiple variables in postmenopausal women.
MEHTODS
1. Data collection
The sampling units of the Korean National Health and Nutrition Examination Survey (KNHANES) were households selected through a complex, stratified, multistage, and probability-cluster design. It represents the entire Korean population by a complex sampling analysis through sampling Wts. We analyzed postmenopausal women who underwent DXA scans from July 2008 to May 2011. The DXA scans were used to measure whole and regional body compositions. Appendicular skeletal muscle mass (ASM) was calculated as the sum of skeletal muscle in the arms and legs measured by DXA scans, assuming that all non-fat and non-bone tissue was skeletal muscle. To determine cut-off point for sarcopenia, previous studies showed various formulae such as ASM/height2 and ASM/body mass index (BMI).[1011] We identified the sarcopenic group defined as an ASM divided by Wt (ASM/Wt) that was less than 1 standard deviation (SD) below the mean of the reference group (20-39 years), which was modified from the studies of Janssen et al.[12] and Baumgartner et al.[13] The cutoff point of BMI for obesity was greater than or equal to 25 kg/m2 on the basis of the Asian Pacific criterion. According to the above definitions of sarcopenia and obesity, our study categorized MS into four groups: normal, obesity, sarcopenia, and SO. MS was diagnosed according to the criteria of the American Heart Association, the National Heart, Lung, and Blood Institute, and the criteria of the International Diabetes Federation.[1415] This definition was fulfilled by the presence of at least three of the following five criteria: (1) waist circumference as central obesity ≥90 cm in males or ≥85 cm in females; (2) serum triglyceride (TG) concentration ≥150 mg/dL (1.7 mmol/L); (3) serum high density lipoprotein cholesterol (HDL–C) concentration <40 mg/dL (1.03 mmol/L) in males or <50 mg/dL (1.3 mmol/L) in females; (4) average blood pressure ≥130/85 mmHg; and (5) fasting serum glucose ≥100 mg/dL (5.6 mmol/L).
The KNHANES protocols were approved by the Institutional Review Board of the Korean Center for Disease Control and Prevention (IRB No. 2010–02CON–21–C, 2011–02CON–06–C).
2. Statistical analysis
In this study, all probability samples were calculated taking sampling Wts into account with the complex sample design of KNHANES to represent the total population of Korea. Categorical variables were used Pearson's chi-square test in complex sampling and were presented as percentages; continuous variables were used as descriptive statistics in complex sampling and expressed as mean and standard error. To work out the association between them and MS in postmenopausal women, we estimated the odds ratio (OR) of MS in the postmenopausal group by logistic regression analysis in complex sampling after adjusting for confounding factors to determine whether or not sarcopenia and obesity could be independently associated with MS. Menopausal age, hormonal treatment, drinking status, smoking status, physical activity, chronic disease, and economic status were designated as confounding factors. All statistical data were analyzed using the IBM SPSS software version 22.0 (IBM Corp., Armonk, NY, USA). A P-value of less than 0.05 was regarded as statistically significant.
RESULTS
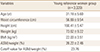
Among the 37,790 subjects who underwent the health examination and interview, the number of postmenopausal women was 7,431 (53.7%). After excluding 3,248 subjects for missing the adjustment values, the final 4,183 participants were included in the study (Fig. 1). The characteristics of the young reference group as healthy women aged 20 to 39 years were presented with mean and SD (Table 1). It indicated that the cutoff value for sarcopenia was 23.76% as ASM/Wt (%).
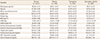
The normal population group was the most common with 2,071 (49.5%). In sequence, the SO group was 855 (20.4%), the obesity group was 700 (16.7%), and finally, the sarcopenia group was the lowest with 557 (13.3%). Mean ASM/Wt (%) was lower in SO (21.94%) than in sarcopenia (22.37%) (Table 2). In the chronic disease category, the prevalence of hypertension was the largest overall. The prevalence of MS was 23.47% for the normal group, 33.75% for sarcopenia, 58.71% for obesity, and 67.84% for SO (Table 3). The logistic regression analyses were used to determine the OR of MS for four groups of postmenopausal women controlling for menopausal age, hormonal treatment, drinking status, smoking status, physical activity, chronic disease, and economic status (Table 4). In an unadjusted model, the sarcopenia group had an OR of 1.94 (95% confidence interval [CI] 1.52-2.49), and the obesity group had an OR of 4.55 (95% CI 3.63-5.71). Both groups had a higher risk of MS than the normal group. The SO group had an OR of 6.26 (95% CI 5.10-7.70), which was the highest risk category for MS. After adjusting for all variables, including chronic disease and economic status, the SO group had an OR of 5.56 (95% CI 4.49-6.90).
DISCUSSION
The total fat mass tends to increase in women during the menopause period of their lifetime. It is related to hor-monal changes—the decline of estrogen production—as well as normal aging, which contribute to an increase in central fat accumulation and a reduction in lean body mass following the increasing prevalence of MS in postmenopausal women.[1617] In addition, the aging process accelerates a reduction in muscle mass, which can decrease up to 8% every 10 years in women aged approximately 40 to 80 years, then decreases up to 15% every 10 years from then on.[181920]
We examined the effect of sarcopenia and obesity on the risk of MS in postmenopausal women with controlling confounding factors. The results showed a definite relationship between SO and MS in postmenopausal women based on the 2008 to 2011 KNHANES. The OR for MS was approximately twice as high in the sarcopenia group as in the normal group, and six times higher in the SO group. One study suggested that the prevalence of MS in women aged 60 or older was 32.4% in the normal group and 71.1% in the SO group; therefore, the SO group had MS 2.1 times greater than the normal group.[16] Another study found that the SO group was 3.24 times than normal group according to the skeletal muscle mass index after adjusting for age.[21] Therefore, this study proposed that the prevalence of MS for the SO group was approximately twice as high when compared with the previous research when targeting postmenopausal women.
Several limitations should be considered in the interpretation of this study. First, with the cross-sectional nature of this study, it is difficult to clarify the causal relationships between each other. Second, unfortunately, due to the absence of questions on the Questionnaire form regarding menopausal duration, an equivocal boundary between the perimenopausal group and the postmenopausal group could facilitate from premenopausal to postmenopausal status. Third, the definition of sarcopenia has not been uni-versally confirmed, neither has its mensuration and indicators.[22] Fourth, we did not include participants who took medication for hypertension, diabetes, and hyperlipidemia in the diagnosis of MS, as it would underestimate the prevalence of MS. Despite these limitations, this study analyzed the relationship between SO and MS with a complex sampling analysis on the great number of postmenopausal women in South Korea. Therefore, the results were representative in reflecting their relationship in postmenopausal women including early menopause.
In conclusion, this study suggests that the prevalence of MS has increased in postmenopausal women compared with results of previous research.[162123] This is due to the sudden hormonal changes that influence the redistri-bution of body composition, such as central obesity and the loss of muscle mass as independent risk factors that cause MS. Therefore, we further recommend that the morbidity rate of chronic disease be decreased through the prevention and management of modifiable detrimental factors in postmenopausal women.



 XML Download
XML Download