

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Childhood obesity has reached global epidemic levels. According to the latest report by the World Health Organization, almost one in 5 children and adolescents aged between 5 and 19 yrs worldwide were obese or overweight [1]. Compared to other regions of the world, children in the United States (US) have some of the highest obesity rates with one in every 5 children being obese [23]. In addition to the 2-fold increase in the prevalence of US childhood obesity in the past 20 yrs, obesity rates disproportionately impact children with underprivileged socioeconomic backgrounds and those in minority racial/ethnic groups [45]. A previous meta-analysis of a nationally representative sample of children showed that children from low-income households are more prone to being overweight and obese than their high-income counterparts [4]. Families from low-income backgrounds are often unaware of their child’s obesity as being obese has become normalized or do not think that changing/improving their child’s food and exercise habits would be necessary [6]. Isong et al. [5] conducted a longitudinal study on nationally representative data to investigate racial/ethnic disparities in early childhood obesity. Results of this study showed that risk factors, such inadequate intake of fruit and vegetables and high amounts of television viewing, are the most prevalent in African American children from age 9 mon through kindergarten entry, while Asian children have the lowest prevalence [5].
Texas is the second-largest state in the US and is home to more than 29 million individuals. In Texas, about one in every 5 children under the age of 2 is overweight (“85th to 95th percentile for body mass index [BMI]-for-age”) or obese (“≥ 95th percentile for BMI-for-age”) [7]. The population of Texas is projected to reach over 50 million people by 2040, growing at a rate twice as fast as the national average [8].
Obesity in children can have a severe impact on their physical and psychosocial health [9]. Children who are overweight have almost twice the risk of death later in adulthood than their peers with healthy childhood weights [10]. In addition, children who are overweight are more prone than their peers with healthy weights to face a variety of psychosocial issues, which may be adversely influenced by weight stigma that causes bullying, teasing, and victimization [11]. Additionally, obesity is linked to children having a reduced health-related quality of life [12]. These findings warrant the urgent need for early childhood health promotion to prevent obesity in Texas, considering its large population growth.
Childhood obesity is multi-layered in origin, resulting from a dynamic interaction between genetic, behavioral, and social-environmental factors [13]. According to the ecological systems model, described by Davison and Birch [14], inadequate food intake, physical inactivity, and sedentary behaviors are the main risk factors for childhood obesity. This qualitative study focuses on poor dietary choices and increased sedentary behaviors (e.g., television viewing) as childhood obesity risk factors.
The coronavirus disease 2019 (COVID-19) pandemic shifted dietary habits of many families. Since COVID-19 has been declared a global pandemic, many people were challenged by the economic and physical access to sufficient and nutritious food. Financial struggles related to COVID-19 may have pushed more low-income families to consume affordable calorie-dense foods in order to pay for other basic needs, such as housing. Many studies have also found increased consumption of unhealthful foods among older children and adolescents during the COVID-19 yr [15]. Less attention has been given to younger children (< 5-year-old) or explored in the context of the pandemic-related impact on diet and sedentary behavior. To address this gap, this study conducted individual in-depth interviews with low-income families of children under the age of 3 to explore how the COVID-19 pandemic and its subsequent economic challenges have changed eating, mealtime, and sedentary behaviors. Based on the identified nutrition and health challenges, the present study also analyzed parents’ views and preferences regarding nutrition education programs.
SUBJECTS AND METHODS
Research design
This qualitative study was conducted as a needs assessment to a larger intervention study [16]. A generic qualitative approach was chosen to collect data. Individual in-depth interviews with families of children under the age of 3 were used to gain insight into nutrition and health challenges since the beginning of the COVID-19 pandemic.
Sample
Participants were recruited from an Early Head Start program, using a purposeful sampling technique. Inclusion criteria for interviewed parents were being (1) 18 yrs or older, (2) a primary food preparer in the home, (3) able to speak English, and (4) willing to participate and talk about experiences in a one-on-one interview via Zoom.
Digital flyers were created for recruitment and distributed among parents at the study site through existing online platforms, such as storyboards and newsletters. If parents were interested in an interview, they were first asked to complete an online Qualtrics survey with questions about their sociodemographic characteristics and household food security levels. Then, email addresses or phone numbers were collected to schedule an interview for those who showed interest. Given the qualitative nature of the study design, study subject recruitment stopped at the point when additional interviewing would not be further beneficial to the depth and diversity of data collection.
Instrumentation
Before the interview, each participant was provided an informational written handout about the study, which explained the aim, benefits, and risks associated with the study. In addition, the research team provided verbal explanations on the informational handout to all participants. Six multiple-choice and open-ended questions asked about sociodemographic characteristics, such as race/ethnicity, marital status, age, relationship with child, and household yearly income. Household food security levels were measured, using 22 questions on a 4-point Likert scale, based on the US Department of Agriculture’s validated screening tool [17]. The household food insecurity scale includes occurrence questions, asked with a recall period of last 4 weeks preceding the survey. If the participant answers “yes” to an occurrence question, a follow-up questions assesses the frequency of the condition (almost every month, some months but not every month, or in only 1 or 2 mon). Based on answers to each question, each household was classified as high food security, marginal food security, low food security, or very low food security [17].
A semi-structured interview was conducted with participants on Zoom. Semi-structured interviews are the most widely utilized method in health research [18]. A semi-structured interview guide was developed, derived from a literature review. Social Cognitive Theory (SCT) informed the development of the semi-structured interview guide because of its common use and validity for analyzing people’s dietary and physical activity behaviors [1920]. The interview guide focused on 3 constructs of the SCT: self-efficacy, perceived barriers, and social support. Such constructs are considered as evidence-based key factors for changing health behaviors [21]. Interviewed parents in our study were asked to discuss their challenges to various aspects of healthy eating, such as family mealtimes, grocery shopping experience, and nutrition assistance programs. In addition, the researcher asked parents open-ended questions regarding health benefits and harms of screen viewing among children. Finally, parents were asked about supportive interventional strategies that would enhance their current health-related behaviors. Prior to actual data collection, mock interviews were performed among a similar population to ensure that the semi-structured questions were understandable by participants.
Data collection
Prior to the study, the research team obtained written informed consent from all participants. Data were collected between January 2021 and June 2021. The researcher first asked permission to interview and record each participant and then conducted one-on-one in-depth interviews. A moderator and 2 facilitators took detailed field notes simultaneously. Each interview was video- and audio-recorded, lasting between 60 and 90 min. Introductions were followed by ice-breaker questions to establish rapport and open-ended questions to guide additional discussion on the primary research question. The study was given ethical approval by Texas Tech University’s Institutional Review Board (IRB#: IRB2020-541). Only the research team had access to the passcode-protected interview recordings. Participation was maintained voluntarily throughout the interview process. All participants received a $20 gift card for taking time to complete the Qualtrics survey and an additional $20 gift card for participating in the interview.
Data analysis
Data from the Qualtrics survey were exported to IBM SPSS Statistics for Windows, version 25 (released 2017; IBM Corp., Armonk, NY, USA) for analysis. Descriptive statistics were used to assess the level of sociodemographic and household food security levels. All interviews were audio-taped and then transcribed and verified by 3 independent reviewers. Two trained coders analyzed qualitative data throughout a process of generating and reviewing themes in a systematic manner [22], using MaxQDA (VERBI Software, 2021). Both deductive and inductive approaches were utilized to complete the thematic analysis.
RESULTS
Participant and household characteristics
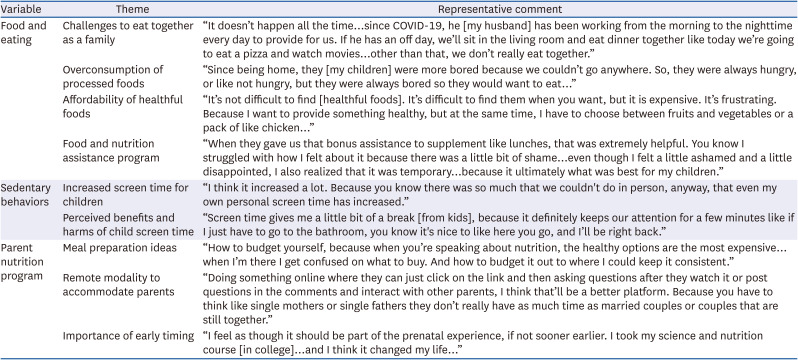
The final sample included 11 parents of children under the age of 3 yrs (Table 1). More than half of the children in this study were male (54.5%), aged between 18 mon to 26 mon (63.6%). Of participating children, 45.5% were Black or African American, followed by Hispanic (18.2%), Non-Hispanic White (18.2%), and Mixed race (18.2%). The majority (63.6%) of households were from low-income backgrounds and reported living in single-parent households, headed by a mother. More than one-third (36.4%) of households reported being food insecure, indicating that food intake for adults in the household had been reduced to such an extent that they had repeatedly experienced the physical sensation of hunger. Results of in-depth interviews resulted in 3 main themes with 9 subthemes (Table 2).
Table 1
Participant and household characteristics (n = 11)
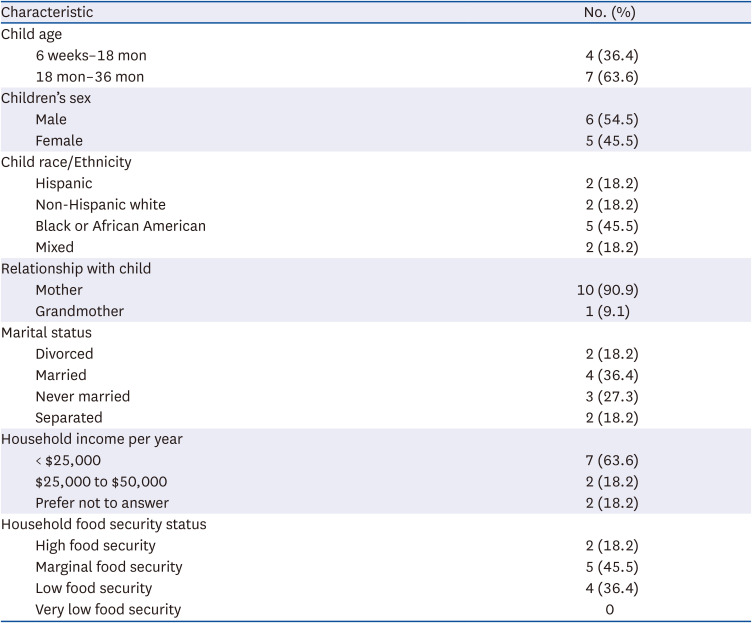
Table 2
Results of individual in-depth interviews
Theme 1: food and eating
Subtheme 1a: challenges to eat together as a family
The majority of the participants said it was crucial for family bonding to have meals together. They valued this time and viewed it as an opportunity to see how each other’s day went and to see how everyone was doing. Typical quotes from this theme were: “You can know how each other’s day went and you can tell when there’s something wrong like if they [my kids] are sad or frustrated. When you have a chaotic day, you don’t necessarily notice kids’ behaviors until you all come together [to the table]. Whenever you are at the table [together], I can see those things.”
Others also thought eating together as a family would strengthen connections within their family. As a single head-of-household mother described, “[Eating together as a family] is a big deal for us. Dinner time has always been important to us because it’s kind of a way to close out the day as a family and give my kids the idea that we are a team, and we are all in this together. We wake up together, we leave the house together, and we may be separate during the day. But when you come home, you still have your family that is here for you, no matter what.”
Participants were asked about what made family meals important to them. A single mother explained that the absence of any meaningful mealtime interactions during her own childhood had an impact on her own parenting, making it something essential for her to have family meals with her children. As she put it: “I didn't get it very much growing up. I was raised by a single mom, and we never just sit down for dinner…There was a brief period of time, where I had to live with my godparents during my later teenage years from about 15 to 19. My godparents always sat down for dinner, and they had a family holidays like Thanksgiving and Christmas dinners and I had never had that before. When I did experience that for a brief period, I saw how valuable it [coming together and sharing a meal] was for bonding and making memories, and it was something that I always wanted to give my children if I ever had children, whether I was married or not.”
Others viewed family meals as the cornerstone of their cultural traditions. One mother emphasized the ways in which family meals convey social and cultural norms. She further illustrated that family meals are important for passing down family traditions to the next generation: “I’m Hispanic and in the Hispanic culture [family meal] is vital to have. Families carve it out like Sunday dinners or at least once a week or special occasions, we get together, and we celebrate…it’s so much more than [meals]. It’s about the time together. It’s about the building of the community and the support of one another…If you don’t want to eat, just come sit at the table, but we’re having dinner you know you can make dinner time, so this is what we do, and my girls are very supportive and understanding because that’s what they grew up doing.”
While all participants recognized the importance of family meals, eating together as a family was a challenge for many families since COVID-19. The majority of participants noted that juggling lots of daily activities to complete (such as work or house chores) and having unpredictable work schedules made it difficult to sit down to a family meal. An immigrant mother said: “Before the pandemic, I had a family that helped me take care of my toddler from 8 am to 5 pm. But then when the pandemic happened, everyone had the fear of I don’t want to catch COVID-19. So, I was forced to look for alternatives. Early Head Start program is that alternative, but then they close by 2 pm. So, I have to plan everything that I am doing to be able to go pick her up at 2 pm and most times, not even sometimes…I have to cut things short…because I don’t have that usual support that I use to have. A barrier to eating together as a family] is just timing. Sometimes it’s as if you’re not so much in control of that. I think it’s mainly because I feel like I have a lot on my plate. With the dinner, sometimes I feel like I need these children to be in bed right now [because] I need to work on my paper…Yes, I love to see that we are eating together and sometimes that happens, but I don’t have special circumstances to make that happen.”
After COVID-19 lockdowns, others struggled to have family mealtimes due to overwhelming parenting responsibilities: “Before the COVID-19 pandemic, dinner was very important. It was a one time that we always come together after the full day. But…during the day, that wasn’t my focus [because] I still had housework to do, especially cleaning up after a toddler, making sure he kept a routine like naps and activity. So, there was a lot going on to where the day meals were not like [my focus] and I wasn’t going to kill myself…I normally do not provide breakfast and lunch [because] they were provided at the daycare center, and I used to only provide dinner. So, it was already taking me out of my comfort zone. I said to myself, I want to survive so I’m not going to make myself crazy about it.”
Some families had irregular mealtimes, as a result of changes in parent’s working arrangements happened during COVID-19: “[Eating together as a family] is important to me, but it doesn’t happen all the time. The only time we’ll eat together is like if their dad is off from work. Because like since COVID-19, he has been working from the morning to the nighttime every day to provide for us. If he has an off day, we’ll sit in the living room and eat dinner together like today we’re going to eat a pizza and watch movies because he’s off work. Other than that, we don’t really eat together.”
A mother of a 2-year-old son and a 2-month-old daughter described financial struggles that prevent families from eating together. Since COVID-19, she became unemployed and was unable to get her family the help they required. She then described the challenge of eating together as a family: “We haven’t really been able to do that [eating together]. The only table we have is her [my toddler’s] little table that I bought for her. So, the next thing I want to do is get a table. That way we can all just sit down and eat together…at least eating one meal together, whether it’s breakfast or dinner.”
Subtheme 1b: overconsumption of processed foods
The majority of participants said that since COVID-19, snacking in their household had increased, which they frequently attributed to stay-at-home orders and remote working. Because they were bored, children snacked more: “Since being home, they were more bored because we couldn’t go anywhere. So, they were always hungry, or like not hungry, but they were always bored so they would want to eat. So, like every so often they’re like what’s in the fridge and they want to snack on something and I’m like stop eating…Trying to keep the kids from eating so much just out of boredom that was a that was a challenge. Because them being kids, they’re not as worried as adults, and they think oh mom can just go buy more and I’m like well I don’t really…we are in a very unique situation and we need to really make our choices, and when and what we eat.”
Some participants reported increase in snacking habits for both adults and children in the household: “Lots of grazing and lots of snacks, instead of actual meals. Like maybe one meal a day like dinners [was actual meals] and the rest was like cereal. Sandwiches very simple and fast. And we were at home, so I don’t understand why. But maybe dinner was full meals and everything else was like what I would consider a snack.”
In addition to snacking, many participants noted that they increased consumption of processed foods such fast food meals, like Wendy’s or McDonald’s: “Before the COVID-19 pandemic, I would always make sure that she [2-year-old toddler] ate at 7 o’clock because she needs to be in bed by 8:30. But with the pandemic and not having a consistent employment, sometimes I’ll have to pull up to McDonald’s and get her something real quick, because I have to make enough money that day, so you drive around for the rest of the day.”
Most participants linked greater consumption of processed foods to time restraints to complete all of their responsibilities in a day. However, this was not the case for all participants. For example, a single head-of-household mother of a 2-year-old encapsulated eating out to support local business: “You know, I have been a little concerned about the local economy like local businesses and restaurants. They were losing money, so we started ordering from a few local places anywhere from one to 3 nights a week, just to sort of help and give them the business. It’s also taken a little bit of stress off me because I don't have to cook every single night, you know and the cleanup and all that.”
Subtheme 1c: affordability of healthful foods
While accessing healthy foods was not identified as a barrier, almost all participants agreed that purchasing healthy foods is expensive. A single head-of-household mother of 2 children indicated that she relies on their extended families for foods when low on budget: “I really try to do like $60 to $70 a week…sometimes like my parents will help me, if I’m short [on budget], you know they’ll kind of help me out to buy what we’re lacking. With 2 kids…we have to keep it cheap…to make it stretch.”
Environmental change was also identified as having a detrimental effect on food security. A mother of 4 recently relocated to Texas from California emphasized ‘food deserts’ and asserted that the cost of healthy foods is high in the neighborhood: “It's not difficult to find. It’s difficult to find them when you want, but it is expensive. It’s frustrating. Because I want to provide something healthy, but at the same time, I have to choose between fruits and vegetables or a pack of like chicken. Though it’s either or I can’t do both…I'm like in a food desert in a way, because I mean we’re from California…so a lot of the fruit that we used to buying California was all the time inexpensive. So, we get here [to West Texas] and it’s like what you’re telling me that grapes are like $3 a pound like, what, you’re telling me I can’t buy strawberries in December? So for me we had to get used to the different seasons that are available because I wasn't used to that. And even on top of that, it is expensive, because I guess we’re considered in like a [food] desert or whatnot.”
Similarly, an immigrant mother from Nigeria stated: “It is expensive, back in Nigeria it was cheap to cook a pot of vegetables. What I mean about vegetables I mean like you have spinach those kinds of green leafy vegetables and then make it into a soup and then eat it. It was way cheaper. But coming here I found out that it costs you almost triple the amount to buy fresh spinach than to just get the frozen spinach. So, the first time I tried to cook fresh spinach I was disappointed by the quantity of soup I got. I spent over ten dollars, look at this soup!… So, yes I have the opinion of eating healthy or eating fresh vegetables, all of that is more expensive to do that.”
Subtheme 1d: food and nutrition assistance program
All participants reported having used food and nutrition assistance programs, such as Supplemental Nutrition Assistance Program (SNAP), Women, Infants, and Children (WIC) program, and the local school district meal program, to support the need to feed their children during COVID-19. Many parents reported utilizing food assistance programs as a result of financial difficulty brought on by unemployment during the pandemic.
A single head-of-household mother of a 24-month-old was temporarily unemployed and used SNAP to help feed her own children during COVID-19: “I was using SNAP during the period of time that I was unemployed, and that was extremely helpful because I mean it covered everything that we needed.”
Another mother said: “I was on unemployment in December, January, February and March during COVID-19. We were not working, and so we had to apply for SNAP because we were running out of food.”
The majority of participants found it challenging to stretch their meal budget during COVID-19. Some people viewed the advantages of food assistance programs as a means to purchase healthy foods and avoid household food insecurity: “I guess relief because you stress out as a parent to not be able to feed your kids…[The food assistance program] it keeps me on track, and I’m just happy I have that resource and that I was able to obtain that resource.”
Another mother shared mixed feelings of relief and shame at the same time: “When they gave us that bonus assistance to supplement like lunches, that was extremely helpful. You know I struggled with how I felt about it because there was a little bit of shame. I have to ask the government to help me feed my own children, and this is this embarrassing. But then I had to stop and look and realize that this was a temporary help for me during a transitional time…With all the circumstances, even though I felt a little ashamed and a little disappointed, I also realized that it was temporary, and it was okay, because it ultimately what was best for my children.”
Theme 2: sedentary behaviors
Subtheme 2a: increased screen time for children
Nearly all parents felt that their children’s screen usage drastically increased, compared to pre-pandemic times. A mother from a dual head-of-household reported increased family TV viewing time during the COVID-19 pandemic stay-at-home orders: “It has been increased since the pandemic. I mean when you’ve been stuck in a house nothing to do so, you got no choice but to either be on your tablet watching something entertaining or watching television. I believe, it has been increased for a lot of people.”
Due to changes in work modalities, a mother from a single head-of-household reported increasing her child's screen time and acknowledged that technology is now an essential part of our society: “I think it increased a lot. Because you know there was so much that we couldn’t do in person, anyway, that even my own personal screen time has increased. You know Zoom meetings for work and other personal [things], even the church stuff we've done online, and so everything's been increased. Technology is such a huge part of our lives now that I wouldn’t want to completely cut it [child screen time] out and I want to give them some exposure. As they get older, that time will increase naturally on its own, when they eventually get their own cell phones and stuff like that.”
Subtheme 2b: perceived benefits and harms of child screen time
The main advantage parents cited for their children’s screen use was improved educational opportunities. A mother from a single head-of-household stated: “What I do with the kids is on both of the tablets that they have access to everything is like closed captions at the bottom. And with my son, and that was one of the ways that he really learned how to read and because he would look at the words popping up on the screen. My child started to identify words so much faster. I never thought that closed captioning on technology would actually make my child be interested in words and vocabulary so that’s been a big help surprisingly.”
Many parents reported benefits of screen devices as tools to soothe their children: “Screen time gives me a little bit of a break, because it definitely keeps our attention for a few minutes like if I just have to go to the bathroom, you know it’s nice to, like ‘Here you go, and I’ll be right back.’ I guess just keeping her [my toddler] calm.”
Parents who were asked why they would be concerned about their children’s screen usage mostly concentrated on visual problems and poor social development. Interestingly, they rarely recognized the potential risk of screen time associated with child obesity. A mother from a single head-of-household stated: “I worry about if it's okay for their vision and I worry about ‘Is my child going to get a brain tumor someday’ because you know everyone panicking about that. So those are my biggest concerns. I also worry about them [not] being in touch with reality, because the face-to-face interaction with people is just different than on a screen.”
Theme 3: parent nutrition education program
Subtheme 3a: meal preparation ideas
The majority of parents indicated their desire to participate in nutrition education. They were most interested in learning how to cook and how to prepare healthy meals on a budget: “How to budget yourself, because when you’re speaking about nutrition, the healthy options are the most expensive…[At the] grocery store, nutritious foods and healthy foods [are] there. It’s just a matter of when I’m there I get confused on what to buy. And how to budget it out to where I could keep it consistent.”
They also wanted to learn how to involve young children in the kitchen: “Some ideas about bringing children into the kitchen or families into the kitchen, how to incorporate them into the meal planning and preparation. Snack ideas that at least can bring everybody into the kitchen and make together or pick a meal, that they can make together. And even down to what role goes to who, like age wise they [kids] are appropriately able to do. So, they [kids] are as much a part of the planning and preparation as you want.”
A few parents also stated that they would like to engage in interactive and hands-on cooking activities over merely learning about recipes: “They were giving a nutritional cooking class [in a church], so she [a chief] was cooking in front of us. And she was showing us how to do it and then she passed around the sample…and she gave out the recipe of how to make it, and so I still make that [cauliflower rice] to this day. She had all the ingredients and had pre-printed out like cards. Like index cards, but a little bit bigger with the recipe on it, and she has showed us how to do and then she passed out…I did it at home, and it was so good, and I still do it!”
Subtheme 3b: remote modality to accommodate parents
Participants were asked questions about practical aspects of attending nutrition education classes, such as the best time of day and the ideal delivery modality. Parents felt that online materials in the form of online videos would be a desired platform to fit information into their busy schedules.: “Picking a good time is important because a lot of times they [some parents] only want to do it on the weekend, or they only want to do it late at night, and sometimes it doesn’t work with every parent…So, if it’s a recording then if I’m free earlier today or if I’m on my way to work, I can just go ahead and watch it or listen to it, rather than having something to read.… Doing something online, where they [parents] can just click on the link and then asking questions after they watch it or post questions in the comments and interact with other parents, I think that’ll be a better platform. Because you have to think like single mothers or single fathers, they don’t really have as much time as married couples that are still together.”
Subtheme 3c: importance of early timing
The majority of participants agreed that such parent nutrition education is urgently needed for parents of young children. The sooner parents receive nutrition education, the more they can improve the nutritional and physical well-being of their children. A mother of 2 children stated: “From when they [my children] are little because we [parents] are the one providing those [food] choices to them. And the more knowledge, the more in control the parent feels. When I was fresh out of high school, I didn’t know [about child nutrition]. You know, like my [older] daughter’s 10 now and if I would have known what I know now about parenting, grocery shopping on budget, or cooking, I would have been golden back then, when she was born, but I was so young. I was trying to figure out as a first-time mom. At the time it felt impossible. If I knew then what I know now, it would have made life so much easier.”
A mother from a single head-of-household specifically mentioned the parental influence on eating behaviors during toddlerhood, “I think you know right when they start eating solid foods, you know from that moment forward until they get into their school years. Like my daughter (18-month-old) is a big time to have that support as far as variety of foods, giving her options, but really exposing her to the healthiest foods possible. Because I think that’s when they kind of develop the taste for it and moving forward it’s not hard to feed them healthy foods, because they're used to it by then.”
A few participants expressed that nutrition lessons should be a part of childbirth classes especially for first-time and pregnant mothers, “Like parenting classes, you know, sometimes they give you the birthing classes of what to expect when you’re going to give birth…because I took those classes when I first had my son…but now that I think about it, there was never nutrition lessons, where there were, like hey, ‘These are the stages of babies grow, these are the stages of babies nutritional growth. This is when they're supposed to eat solids, this is what you should introduce first. This is how much amount they should eat.’ Like none of that was ever taught and I feel like when we’re doing the birthing classes, maybe they should consider doing a nutrition class, that would have really helped me out.”
Females of childbearing age were also identified as a target audience for parent nutrition programs: “I feel as though it should be part of the prenatal experience, if not sooner earlier. I took my science and nutrition course [in college]…and I think it changed my life…so I feel like that that’s right there, where someone hopefully pre-having children, that information affects them and changes their life.”
DISCUSSION
The results of this qualitative study provide insights into the impact of COVID-19 on eating habits and physical activity of families with young children. In the study, most families reported being marginally and low food secure. Households with marginal food security reported worrying about their food running out before they were able to afford more. Households with low food security indicated that they sacrificed quality of foods by eating less diverse meals or unfavorable foods, sometimes or often, and/or reducing quantity of foods. Most parents reported that the frequency of family meals had declined, while they also reporting consuming more processed foods. Almost all parents agreed that fresh and nutritious food is accessible but is expensive for families to afford, which limits their consumption of healthy meals. Some parents used food and nutrition assistance programs, such as WIC and SNAP, to buy food for their families during COVID-19. In addition, all participants reported increased screen time among their children.
Although almost all participants recognized the importance of family mealtimes, they found it unattainable to eat together regularly compared to pre-COVID-19 times. A previous meta-analysis study showed that children and adolescents with a fewer frequency of having meals together as a family were more likely to be overweight than their peers who had more than 3 family meals per week [23]. Another study found that eating family meals was associated with improved diet quality, such as less intake of sugar-sweetened beverages [24]. Parents in this study associated increased snacking in their children with boredom eating because of stay-at-home orders. This finding aligns with results of a study by Philippe et al. [25], which discovered that feelings of boredom in children contributed to increased snack patterns. Emotional overeating, food enjoyment, and food responsiveness are referred to “food approach” behaviors [26]. Children may have craved more foods due to boredom, inability to interact with friends and other feelings related to stay-at-home orders. This would be in line with studies demonstrating how an emotional void is linked to increased snacking [27]. Over time, these behaviors would be expected to lead to an increase in obesogenic behaviors and weight gain.
During COVID-19, low food security levels increased worldwide. Many single parents in the study cited a lack of financial resources as a main barrier to afford healthy diets. Earlier studies have shown that single-parent households with children are especially vulnerable to low food security during and before COVID-19 [2829]. Furthermore, a decrease in the number of single parents who are employed was particularly high among those with children under the age of 5 in 2020 [30]. With an increase in unemployment rates, the risk of low food security may have been exacerbated for single-parent households with young children during the COVID-19 pandemic. In this study, a participant particularly mentioned “food deserts” to describe her food environment because she did not have access to supermarkets or other food retailers that sell affordable healthy foods. Low-income families from such environments may be more susceptible to low food security if they can only afford nutrient-dense foods with a high cost [31]. This is of concern because low food security is correlated with poor diet quality and obesity [32]. A national survey study found a significant increase in food insecurity during COVID-19 and a decrease in intake of healthy foods such as fruits and vegetables [33]. In the same study, more than one-third of low-income households with children reported that their fruit and vegetable intake decreased during COVID-19.
Numerous studies have shown that food and nutrition assistance programs play an important role in helping to alleviate low food security. In fact, the current study found that most families utilized government- and state-administered food assistance programs, such as SNAP, WIC, and local school meal services. Parents viewed such programs in a largely positive light in order to help mediate the negative effects of hunger and food insecurity in their children during COVID-19. Yet, a few participants in this study also reported feelings of shame, anxiety, and stigmatization related to obtaining free foods for their children through food assistance programs. Similarly, a previous study pointed out that the fear of being judged and devalued was one of the common challenges to participate in food and nutrition assistance programs among low-income households [34]. Fang et al. [35] also found no evidence that food assistance programs reduced relative emotional distress, such as anxiety or depression, in families with children. While such programs may alleviate economic hardships on parents, they might not lessen emotional burdens due to the perceived stigmatization and shame associated with participation in such programs. Such shame and perceptions of stigmatization can lead to greater food insecurity as families are less likely to enroll in such programs when needed.
Almost all parents reported that their child increased daily screen time compared to pre-COVID-19. Parents also noted using children’s screen time to ‘get things done’ in correspondence to balancing work and other parenting responsibilities. Similarly, a recent survey study in the US reported that older children’s screen time doubled during COVID-19 to 7.7 h per day, a number excluding school-related work [36]. In the current study, most parents described that although they make sure that their children watch age-appropriate media, they do not have guidelines or rules in place for child screen time. However, Lampard and colleagues found a strong association of less child screen time with high parental restriction of child screen time [37]. While all parents in our study expressed a concern of impaired vision and social development related to screen viewing, they rarely recognized the link between screen time and weight gain in children. These findings highlight the need to educate parents on the potential risk of screen viewing on obesity and advise them to limit their children’s screen time, as recommended by American Academy of Pediatrics [38].
This study provides deeper insights into low-income families with young children during COVID-19. In-depth individual interviews enabled us to gain novel insights into the experiences of low-income parents with young children during COVID-19. These results can be used to inform a larger study on the best resources for parents to improve dietary habits and reduce sedentary behaviors in children at home. Families need improved options and resources when under the stress and challenges of a worldwide pandemic and will certainly benefit from support as society moves beyond COVID-19 social isolation. In addition, the scientific literature has mostly focused on families with school-aged children to explore nutrition and health challenges. However, interventions are more likely to be effective when they are provided earlier in life (from birth to 3 yrs of age) than later. This qualitative study yields a greater understanding of key factors related to nutrition and health behaviors in infants and toddlers, as well as potential barriers, all of which are critical for successful early intervention development. However, there are several limitations that should be acknowledged in this study. The use of virtual interviews could have compromised participants’ abilities to express themselves, and capturing non-verbal cues was less possible. In addition, this study did not measure other important key factors related to obesity and overweight, such as weight status and gain and eating patterns among children and their parents. The sample for this study was recruited from Early Head Start programs and most participants were single parents. Thus, results may not be generalized to other populations in different programs or from different socioeconomic backgrounds.
This study provides key information on the needs of parents of young children, which can be addressed in post COVID-19, highlighting the importance of supporting families to improve eating behaviors and reduce screen time for young children. Families need support to develop healthy and affordable meal ideas and establish manageable rules around snacks and screen time without adding a significant burden to parents. Using an online or distance modality of educational programming was acceptable to the population and future interventions should consider these along with traditional in-person methods.
 XML Download
XML Download