

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension (HTN) is a prevalent disease worldwide, affecting over 10 billion people.1 As HTN is a leading cause of death and a major risk factor for the prognosis of various cardiovascular diseases, blood pressure (BP) measurement is a fundamental component of clinical care.23 Accurate and timely measurement of BP is necessary for identifying individuals with HTN, monitoring the response to therapy, and preventing the development of associated complications.
Traditionally, BP has been measured using auscultatory or oscillometric semi-automatic or automatic sphygmomanometer. While these methods are considered standard for BP measurement,45 they can be time-consuming, require multiple visits to the clinic, and are subject to measurement errors due to various factors.6 Moreover, conventional non-invasive BP measurement by a sphygmomanometer has limitations in obtaining continuous BP and its variability in daily life, which is known to be a better predictor of cardiovascular outcome than office BP.78910 Although ambulatory BP measurement provides accurate and comprehensive data about an individual’s BP over a 24-hour period, it also has limitations in terms of accessibility and discomfort or interference with daily activities.1112
Recently, a ring-type BP measuring device has been developed as an alternative to traditional cuff-based devices. This device is designed to be worn on the finger, and the BP is measured by utilizing photoplethysmography (PPG). The ring-type BP measuring device is more convenient, portable, and user-friendly compared to the traditional cuff-based device, allowing individuals to monitor their BP easily and frequently. In this study, we aim to evaluate the accuracy and reliability of the ring-type BP measuring device and compare it with the traditional cuff-based sphygmomanometer.
METHODS
Study design and subjects
This was a prospective, single-center, single-arm, pivotal clinical trial to evaluate the accuracy of BP measurement of ring-type smart wearable BP monitoring device, CART-I plus (Sky Lab Inc., Gunpo, Korea), compared to the reference BP reading with an auscultatory sphygmomanometer. The inclusion criteria included the following: 1) subjects with age 19 years or older; 2) those who voluntarily decided to participate in this study, and; 3) those who are willing to comply with the study protocol. Subjects meeting any of the following exclusion criteria were excluded: 1) those in whom the Korotkoff sound (K5) could not be heard during BP measurement using the auscultatory method; 2) individuals with unstable heart conditions (myocardial infarction within one week before the screening date, ventricular arrhythmia, atrial fibrillation, premature ventricular contractions, or pulmonary edema); 3) individuals with an arm circumference greater than 42 cm; 4) individuals with a history of hypersensitivity to the medical device raw material for the clinical trial (polycarbonate); 5) individuals with physical limitations for the application of the clinical trial medical device (e.g., inappropriate ring size, or other physical limitations that prevent the application of the ring-shaped clinical trial medical device); 6) those in whom normal signal acquisition is deemed difficult when wearing CART-I plus on fingers other than the thumb or index finger (e.g., when there is no CART-I plus model that fits the subject's fingers); 7) pregnant women; 8) individuals currently participating in another clinical trial or who have participated in another clinical trial within 30 days prior to the screening date; 9) those in whom the investigator deems participation in the clinical trial inappropriate for ethical or clinical reasons.
CART-I plus
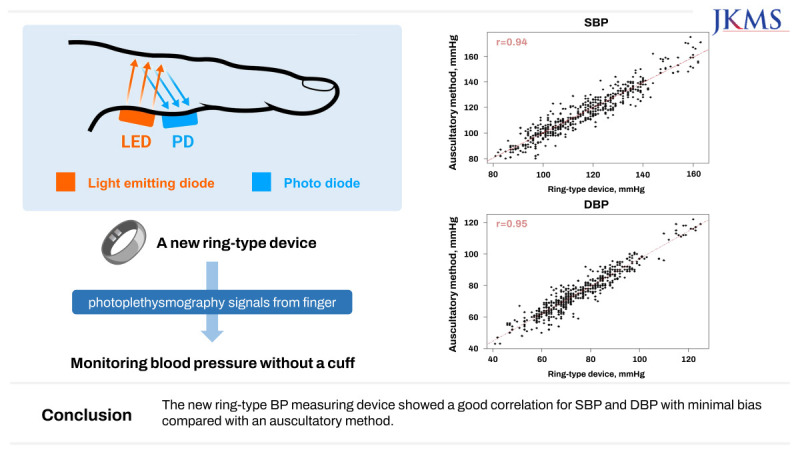
The ring-type smart wearable BP monitoring device, CART-I plus, measures PPG signals from the proximal phalanx and transmits the data wirelessly to a connected smartphone for monitoring BP (Fig. 1). In addition to BP, this device can record electrocardiogram, pulse wave, heart rate, and functional oxygen saturation of hemoglobin in arteries (SpO2). The device wirelessly transmits and stores data through Bluetooth for signal analysis and displaying results.
Fig. 1
The ring-type BP measuring device. The ring-type smart wearable BP monitoring device measures and analyzes PPG signals from the proximal phalanx and transmits the data wirelessly to a connected smartphone.
LED = light emitting diode, PD = photo diode, BP = blood pressure, PPG = photoplethysmography, SYS = systolic, DIA = diastolic.
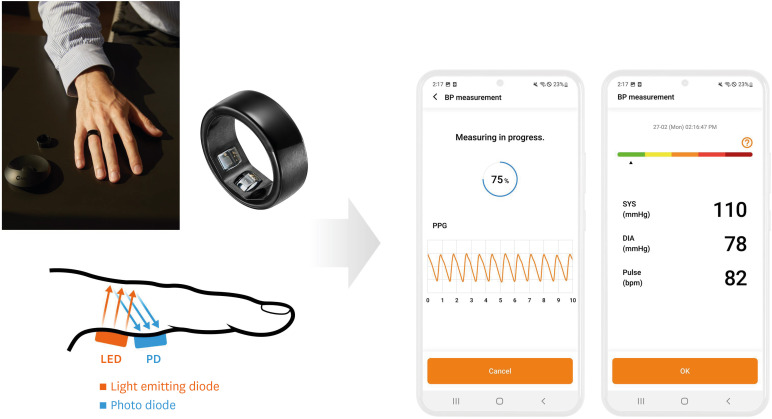
The principle of PPG is to detect changes in light intensity caused by changes in blood vessel volume due to heartbeats. The PPG sensor consists of light-emitting diodes that emit light and photodetectors that detect the emitted light, and it can be measured in reflective mode. The PPG waveform closely resembles the arterial BP waveform in shape and morphology, and changes in response to BP variations. Therefore, BP can be estimated by analyzing changes in the shape of the PPG waveform using a Convolutional Neural Network (CNN) after calibration.1314 Collected raw PGG signals are preprocessed and filtered by algorithm on the server, and raw signals that are difficult to recognize are automatically discarded or undergo a preprocessing stage to transform them into a visually discernible form.
Study protocol and reference measurement
A cuff was placed on the upper arm to check the reference BP by auscultation, while the test device (CART-I plus) was worn on the finger of the opposite arm to simultaneously check the test BP. Before the main test for accuracy evaluation, we conducted two sets of BP measurements using both the reference and test device and entered the results into the application (CART-App) linked with the ring for calibration. After completing the calibration of the test device, the participant received a BP test for accuracy evaluation. At this time, the arm used for the BP test remained the same for both test device calibration and accuracy evaluation. The BP test for each set was conducted simultaneously. The BP test using the auscultatory method was performed by two members of the reference standard examination committee, while the participants performed the BP test using the test device. During the test, the two examiners were blinded to each other’s BP test results. After conducting three sets of tests, the independent examiner checked the test results of the two members of the reference standard examination committee to determine whether a retest was necessary based on the predefined criteria. After completing the accuracy evaluation, the cuff worn on the arm and the test device worn on the fingers were switched. Then, the BP test was performed again, starting from the calibration of the test device to the accuracy evaluation. The detailed study protocols are presented in Supplementary Table 1.
Accuracy evaluation
The accuracy evaluation analyzed the results of the valid sets (up to three sets per arms) of the BP test to evaluate the BP accuracy of the test device. The mean and standard deviation (SD) of differences between the systolic BP (SBP) and diastolic BP (DBP) test results obtained through auscultation and those of the test device were checked. The mean and SD of differences were also evaluated at the sample and participant levels. According to the recommendations by Korean Food and Drug Administration, June 2007 (11-1470000-001459-01) and the International Organization for Standardization (ISO) 81060-2:2018, the acceptable range was 5 mmHg or less and 8 mmHg or less for the mean difference and for SD of differences between the test device and reference, respectively.
Adverse events were classified into those occurring before and after the application of the test device for this study.
Statistical analysis
According to the ISO 81060-2:2018, the minimum number of subjects was 85. Considering a dropout rate of 15%, a total of 100 subjects were recruited. The minimum number of subjects required based on baseline characteristics are presented in the Supplementary Table 2. The primary analysis was based on the full analysis (FA) set which was defined in Supplementary Table 3.
For continuous data, the number of observed subjects, mean with SD, or median, minimum, and maximum values were presented. For categorical data, frequency and proportion were presented. Correlation of BP values between the test device and reference was analyzed using univariable linear regression. The Bland-Altman method was used to present the ‘bias’ (mean difference) and ‘limits of agreement’ (LOA, the mean difference ± 1.96 × 2 SD of difference) between the test device and reference.
Subgroup analysis was performed according to age, sex, body mass index (BMI), and skin color classified by Fitzpatrick scale. All statistical tests were two-sided tests conducted at a significance level of 5%. Statistical analysis was conducted using SAS version 9.4 or more (SAS Institute, Cary, NC, USA).
Ethics statement
The study was approved by Samsung Medical Center Institutional Review Board (reference number: SMC 2022-03-165-010). Informed consent was submitted by all subjects when they were enrolled. This study was conducted in accordance with the Declaration of Helsinki and the ethical standards of the institutional committee on human experimentation.
RESULTS
Baseline characteristics
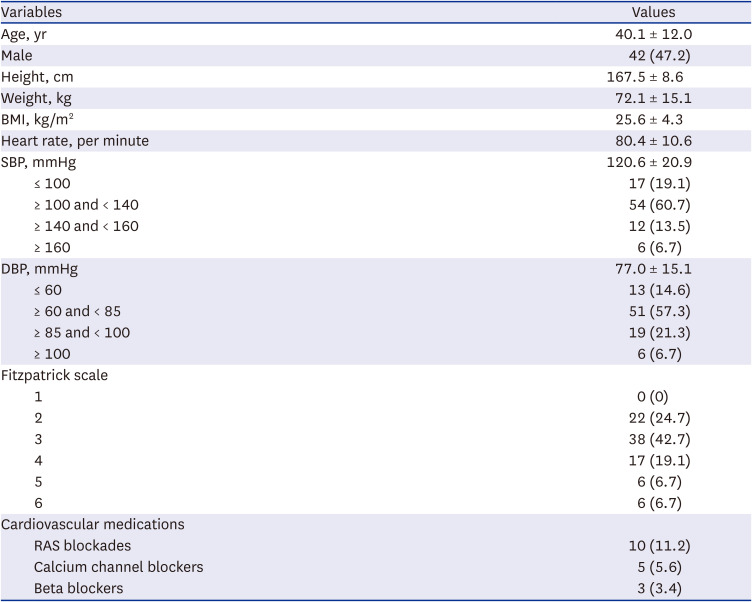
Out of 100 enrolled participants, 89 were included in the FA set (Fig. 2) with a mean age of 40.1 ± 12.0 years and 42 (47.2%) males (Table 1). The mean SBP and DBP were 120.6 ± 20.9 mmHg and 77.0 ± 15.1 mmHg, respectively. Of the 89 participants included in the FA set, SBP ≥ 160 mmHg was in 6 (6.7%), 140 ≤ SBP < 160 mmHg in 12 (13.5%), and ≤ 100 mmHg in 17 (19.1%). DBP ≥ 100 mmHg was in 6 (6.7%), 85 ≤ DBP < 100 mmHg in 19 (21.3%), and ≤ 60 mmHg in 13 (14.6%).
Fig. 2
Study flow.
BP = blood pressure, SBP = systolic blood pressure, DBP = diastolic blood pressure, FA = full analysis, PP = per-protocol.
aThese criteria are based on the International Organization for Standardization 81060-2.
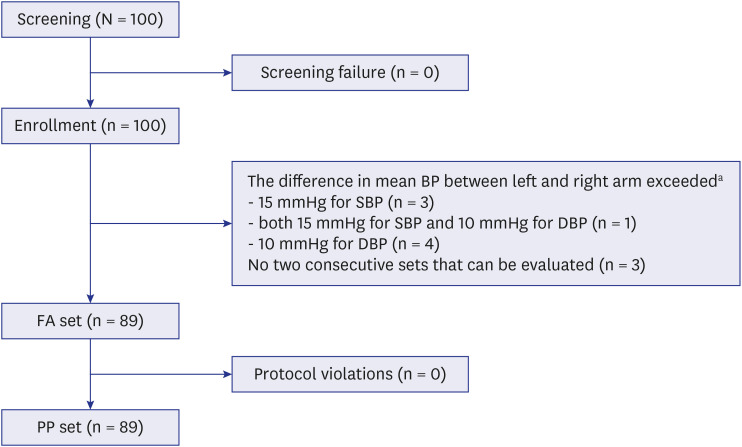
Table 1
Baseline characteristics of subjects in the full analysis set (N = 89)
Accuracy of test device compared to auscultatory method
Of the 89 participants, we obtained 526 samples of SBP and 513 samples of DBP. The mean difference in SBP and DBP between the test device and the reference, in sample-wise comparison, was 0.16 ± 5.90 mmHg and −0.07 ± 4.6 mmHg, respectively. The mean difference in SBP and DBP, in subject-wise comparison, was 0.17 ± 3.67 mmHg and 0.02 ± 3.21 mmHg, respectively (Table 2).
Table 2
Sample- and subject-wise comparison of blood pressure measured by the ring-type device and the reference auscultatory method

When comparing the test device to the reference, the absolute difference was 5 mmHg or less in 353 (67.1%) and 393 (76.6%) for SBP and DBP, respectively, in sample-wise comparison. The absolute difference was 5 mmHg or less in 76 (85.4%) and 77 (86.5%) for SBP and DBP, respectively, in subjects-wise comparison (Table 3).
Table 3
Absolute differences in blood pressure measurements between the ring-type device and reference auscultation method

Correlation of BP measurement
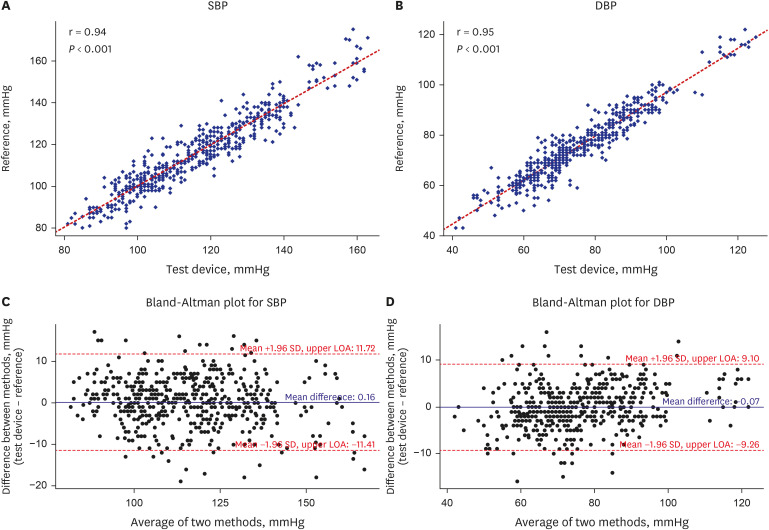
Among 526 samples of SBP and 513 samples of DBP, the correlation coefficient between the test device and reference was 0.94 for SBP and 0.95 for DBP (Fig. 3). The 95% LOA was −11.41 to 11.72 for SBP and −9.26 to 9.10 for DBP.
Fig. 3
Correlation of blood pressure measures between the ring-type device and auscultatory method. (A) Correlation for SBP between the test device and reference, (B) correlation for DBP between the test device and reference, (C) Bland-Altman plot for SBP between the methods, (D) Bland-Altman plot for DBP between the methods.
SBP = systolic blood pressure, DBP = diastolic blood pressure, LOA = limits of agreement, SD = standard deviation.
Subgroup analysis
The test device showed a strong correlation with the reference in subgroup analysis according to age, sex, BMI, and skin color. The detailed mean differences with 95% LOA are presented in Supplementary Table 4.
DISCUSSION
The results of this prospective, first-in-human study demonstrate that the new ring-type device can provide accurate BP measurements compared to the standard auscultatory method without any significant adverse reactions. BP measured by the new device showed a consistent and strong correlation with those by the auscultatory method across various subgroups and BP strata.
Since its introduction in early 20th century, the auscultatory method has been the standard method for BP measurement.6 This technique involves applying an inflatable bladder cuff to the arm and listening to Korotkoff sounds during cuff inflation and deflation to determine BP. While this technique is standard, its application in the general population is limited as it necessitates a clinic visit and requires trained individuals for measurement.615 On the other hand, the oscillometric method utilizes the amplitude of cuff pressure oscillation to detect two transitions during cuff deflation for BP measurement. A semi-automated or automated oscillometric method has become a preferred technique in clinical practice due to its simple measurement process and fewer observer-related errors associated with auscultation.16 Nonetheless, both the auscultatory and oscillometric techniques are difficult to apply in measuring BP during daily activity, which are closely related to cardiovascular outcomes.
PPG is one of the non-invasive methods that can replace the auscultation or oscillometric methods by measuring the speed of the blood flow, commonly known as pulse wave velocity.1718 PPG enables cuffless BP measurement, allowing for easy and automated BP measurement while monitoring BP for a long period of time. PPG is currently gaining attention as a convenient and cost-effective non-invasive method for BP measurement.19 This technique has been implemented and tested in various mobile and wearable health devices, such as wristbands, armbands, mobile phone cameras, finger probes, and wristwatches.20 However, many studies or devices in this field have limited validation attempts, with small sample sizes or a focus solely on healthy individuals.21
Recently, a smart ring that can collect PPG signals from the finger without the need for a cuff, allowing for long-term monitoring of SBP and DBP, was developed. The BP measuring algorithm model was developed to accurately measure BP based on a 1D-CNN structure with intraoperative BP vital records from 4,185 cases.14 In our prospective validation study, the accuracy of BP measurement using the smart ring across various BP ranges was assessed. The mean differences in BP measurements between the smart ring and standard auscultatory method were less than 1 mmHg for both SBP and DBP. More than 90% of the smart ring BP measurements showed a difference of less than 10 mmHg compared to the auscultatory measurements for both SBP and DBP. While previous studies have reported a correlation between their algorithms and reference methods, the reported values were mostly modest and focused on SBP alone.20 The BP measured by the smart ring in this study exhibited a strong correlation with that measured by the auscultatory method, with a Pearson’s correlation coefficient exceeding 0.9 for both SBP and DBP. Additionally, the 95% LOA between the smart ring and auscultatory method were comparable to or lower than those reported in previous studies on wearable devices.2223 We enrolled not only healthy individuals but also individuals with various medical disorders, resulting in approximately 27% of study subjects having underlying medical conditions, and 15.7% with a history of HTN. The measurement accuracy of the smart ring was consistent regardless of subgroups based on age, sex, BMI, and skin color. Only three individuals failed to obtain two or more BP measurements for comparison.
The above-mentioned findings demonstrate the feasibility of using the smart ring in clinical practice for accurate BP measurements. The ring also enables noninvasive and beat-to-beat monitoring of BP variability throughout both awake and sleep periods, empowering people to take control of their own healthcare with minimal disruption. It is well known that 24-hour BP monitoring is more effective in predicting cardiovascular outcomes compared to measurements taken in an office setting, thus providing valuable insights for physicians to adjust treatment plans as necessary. Given its ability to gather BP data for a duration exceeding 24 hours, the ring holds the potential to uncover diverse, yet undiscovered, clinical insights associated with BP.
This study, however, has several limitations. First, the sample size was relatively small. While the smart ring met the predefined international accuracy criteria, it is necessary to validate its accuracy in larger samples with a wider range of BP values. Second, this study was conducted on Korean and African populations. Although favorable results were observed in subgroup analysis based on skin color, validation in Western populations is required. Third, it is known that BPs can vary depending on the measurement site, including the aorta, upper arm, and lower arm, as well as between cuff-measured BP and intra-arterial BP.2425 Therefore, it is important to note that in our study, we assessed the accuracy and agreement of BP measurements obtained with the ring-type device compared to cuff-measured BP at the upper arm. Nevertheless, our study represents the first demonstration of a ring-type wearable device for BP measurement, showcasing its potential application in various cardiovascular diseases.
In this prospective, first-in-human study, the smart ring exhibited a high level of accuracy in BP measurement in comparison with the standard auscultatory method. This device has the potential to provide accurate long-term BP monitoring in daily life.
 XML Download
XML Download