

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Healthcare providers frequently experience diverse ethical concerns affecting clinical practice, which may cause ethics-related stress if unsolved.12 Clinical ethics support (CES) is a form of preventive ethics that aims to support healthcare providers in addressing controversial ethical issues faced in clinical practice.34 Although various approaches to CES have been adopted in different countries, CES generally includes a clinical ethics committee, clinical ethics consultation, and informal types of ethics support such as moral case deliberation, ethics rounds, ethics forums, and ethics reflection groups.5 Irrespective of the CES approach, it is of primary importance for CES to accurately identify the ethical concerns of the stakeholders and address them in the recommendations.56
There has not been any legal status for withdrawal or withholding of life-sustaining treatment (LST) in Korea by 2018. In 2018, the ‘Act on Hospice and Palliative Care and Decisions on LST for Patients at the End of Life’ (LST Decisions Act) was enforced, which mandated the establishment of institutional ethics committees in healthcare institutions to function as CES for addressing cases of ethical conflicts between stakeholders.7 Prior to the introduction of the Act, there was a viewpoint in Korea that one of the CES, ethical consultation, should be integrated with the institutional ethics committee,89 but the Act makes no mention of the role, function, or composition of ethics consultation.
Before the enforcement of the LST Decisions Act, some national studies reported that healthcare providers in university hospitals encountered serious ethical dilemmas and issues such as withdrawal and withholding LST, doctor-patient relationships, and surrogate decision-making.1011 After the enactment, a survey of physicians working in a large university hospital in Korea indicated the differences in response to a decision on LST implementation in ambiguous cases, which indicates the need for CES in such cases.12 However, to the best of our knowledge, there is a lack of studies investigating the ethical issues faced in clinical practice based on the legal framework of the LST Decisions Act.
Therefore, this descriptive study aims to examine the characteristics of cases that were referred to CES and the resulting ethical issues arising in an affiliated hospital in Korea during three years after the enforcement of the LST Decisions Act.
METHODS
Clinical ethics support at Seoul National University Hospital
The Seoul National University Hospital is a tertiary referral university hospital focusing mainly on acute intervention, comprising 1,793 beds and 37 departments. The hospital has had a functioning hospital ethics committee since 1998, however, it primarily manages disputes between healthcare providers and patients or family members.13 In addition to the hospital ethics committee, since February 2018, an institutional ethics committee has been launched and designated as a functioning CES with the following roles clarified by the LST Decisions Act: 1) deliberation on matters requested by a patient/family or a healthcare provider regarding LST decisions, 2) deliberation on replacing doctors in charge, 3) providing counseling for a patient/family regarding LST decisions. Additionally, the institutional ethics committee manages conflicts related to treatment/care decision-making between stakeholders. Patients, their family members, or any healthcare provider can request to avail the services of CES.
Under the institutional ethics committee of the Seoul National University Hospital, two sub-groups perform the role of ethics consultation—the sub-committee and the ethics consultation team. The sub-committee composes of members including three or four physicians (each majoring in medical oncology, psychiatry, and pediatrics), a lawyer, and a palliative care nurse, who review and deliberate the case and provide ethical recommendations in the form of ethics consultation reply. The ethics consultation team has been formed since August 2019 to respond to urgent cases. The team consists of a palliative care physician, a nurse with advanced training in ethics, and a medical social worker, who also assume the role of secretary of the institutional ethics committee and sub-committee. The ethics consultation team is expected to promptly review the case, meet the stakeholders, and triage the cases. Then, they provide consultation replies for simple cases and speed up discussion regarding complex cases. The ethics consultation team is available from 9 am to 6 pm per day, 5 days per week, and can be contacted during weekends or holidays through electronic consultation requests or by telephone or email. The ethics consultation team were not authorized to vote in the deliberation process of the institutional ethics committee or sub-committee. Regarding the CES process, the responses of CES to the cases were classified into four categories: information provision, operation of the ethics consultation team, operation of the sub-committee, and operation of the institutional ethics committee.
Study design and cases
The present study designed a retrospective cohort composed of cases referred to CES of the Seoul National University Hospital from February 5th, 2018, which is the first full year of the standardized ethics consultation template in the electronic medical records, to February 4th, 2021. Cases were included for analysis if a standardized ethics consultation template was documented via formal format or an ethics consultation request note was made in the medical records or an ethics consultation inquiry was made through telephone or email. Cases requested incorrectly and cases withdrawn due to changes in patient condition before the response of CES were excluded from the study. If a patient was referred to CES multiple times, they were regarded as separate cases.
Data collection
The electronic medical records and filed documents of CES were retrospectively reviewed to collect information on the sociodemographic, clinical, and decision-making-related characteristics of the cases. Most similar overseas studies describe ‘end of life’ as the time from months to years before death, however the LST decisions Act in Korea distinguishes ‘terminal stage’ and ‘end of life process’ as follows: 1) the terminal stage described as having a life expectancy of only a few months due to lack of possibility of recovery and gradually worsened symptoms, and 2) ‘end of life process’ described as a state of imminent death despite treatment.7 According to the LST Decisions Act, LST decisions could be defined as legal only when a patient is at dying with last few days, which indicates the latter. As a legal prerequisite, it was investigated whether a patient is in dying and death at the time of referral. For the patients who were hospitalized and discharged, the length of hospital stay, discharge outcome, and location were collected.
Analysis of ethical issues
To identify the ethical issues reported, we conducted a qualitative content analysis of the narrative portions of the ethics consultation template written by a requestor, an ethics consultation write-up transcribed from committee member discussions, ethics consultation notes containing the committee’s final recommendations and conclusion, and interview notes containing stakeholders and institutional ethics committee secretaries (YK, WC, SHY). First, an initial review of five cases for identifying recurrent themes was performed by two authors (YK, WC). Later, a draft checklist and codebook including the definition and description of terms were developed by three authors (YK, WC, SHY) after conducting a literature review56141516 of common ethics themes and issues in CES (Supplementary Table 1). The checklist and codebook were then revised after five authors (YJ, WH, SHY, MSK, HYP) reviewed and applied the checklist and codebook for the randomized sampled cases (n = 20). At the time of the pilot test, three authors (YK, WC, SHY) reviewed the 20 cases together and two authors (MSK, HYP) reviewed them separately. Three authors (YK, WC, SHY) did most of the analysis but did not have the authority to offer their direct opinions in the write-up and consultation notes. Two non-interviewing authors (MSK, HYP) attempted to assure objectivity and transparency of analysis of the interview notes by comparing individual coding at various locations and times. When the concern addressed by the referral clinicians was what was best for the patient, especially when the patient was unable to express his or her intention, ‘best interest’ was coded as a key ethical issue.17 In the case of quality of life, it was coded as applicable when the referral clinicians inquired about the patient’s quality of life in view of the symptoms of the illness and the side effects of treatment, the patient’s functional ability to perform daily activities, the patient’s subjective experiences of happiness, pleasure, pain, and suffering, and the patient's independence, privacy, and dignity.18 Because issues related to withholding or withdrawal, or futility commonly occurs at the end-of-life, we coded the end-of-life only for issues related to end-of-life care rather than those specific issues. The ethical issues (codes) from each case were recorded on the coding sheet when they were mentioned in the narratives regardless of the counts. The main header categories were selected when a corresponding sub-category was identified in the narratives or without a sub-category. At least one conceptual category and one ‘key ethical issue’ are required to be selected for each case. Due to the complexity of ethical counseling and the various issues that could arise when a case is requested, the five authors who participated in the analysis repeated their discussions until they achieved a consensus on the key issue. After identifying the key issue, similarities and differences were reexamined and reviewed by comparing this instance to others.6151619 After coding all the cases once, the coders (YK, WC, SHY) discussed any disagreement with each coding result and selected the final code together.
Statistical analysis
Descriptive data were used to summarize the demographic and clinical characteristics of the patients. Pearson’s χ2 test or Fisher’s exact test was applied for the categorical variables. In addition, frequency analyses of ethical themes and key ethical issues present in the cases were conducted. A comparison of the ethical issues was conducted between the adult group (aged over 19 years) and the pediatrics group (aged under 19 years) by the judgment of the end-of-life stage at the time of referral. All statistical analyses were two-sided (statistical significance at P < 0.05, 95% confidence intervals [CIs]). All analyses were conducted using STATA version 16.0 (StataCorp LP, College Station, TX, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Hospital (approval No. H-2205-065-1322). Informed consent was waived according to the protocol of the Institutional Review Board due to the retrospective design of the study.
RESULTS
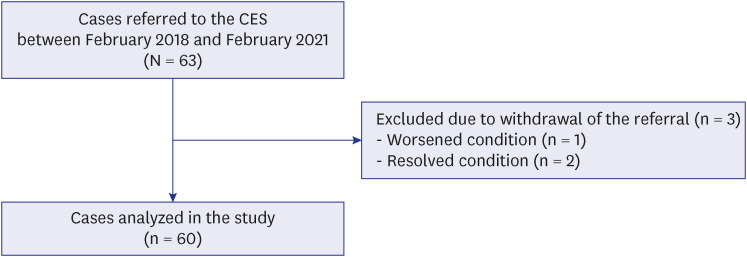
Among the 63 cases referred to CES of the Seoul National University Hospital during the study period, a total of 60 cases were analyzed after excluding three withdrawn cases (worsened condition: n = 1, resolved condition: n = 2) (Fig. 1). Regarding the method of referral, 44 cases (73.3%) were referred through formal documentation, 12 cases (20%) via ethics consultation requests on medical records, and 4 cases (6.7%) via phone or email. Most of the cases (93.3%, n = 56) were referred by the patient’s physicians and others from patients’ families. Of the 60 cases, three were referred for the same patient, and therefore, the number of patients analyzed was 57.
Demographic characteristics of patients
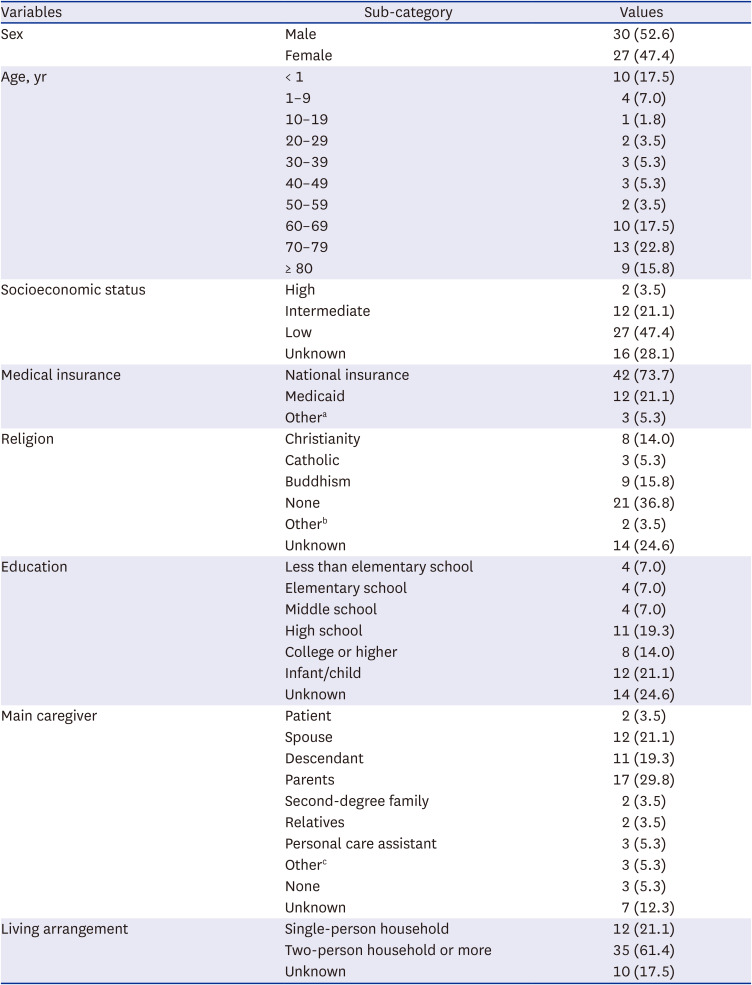
The baseline demographic characteristics of the 57 patients are shown in Table 1. Men consisted of 52.6% and patients over the age of 60 accounted for 56.1% of the total sample. The predominant age group was seventies (22.8%). Regarding socioeconomic status, 47.4% were low-income and 21.1% were medical aid patients. The majority of the patients had their family as the main caregiver, however, 10.6% had non-family caregivers and 5.3% had none.
Table 1
Socio-demographic characteristics at the time of referral (N = 57)
Clinical characteristics of the cases
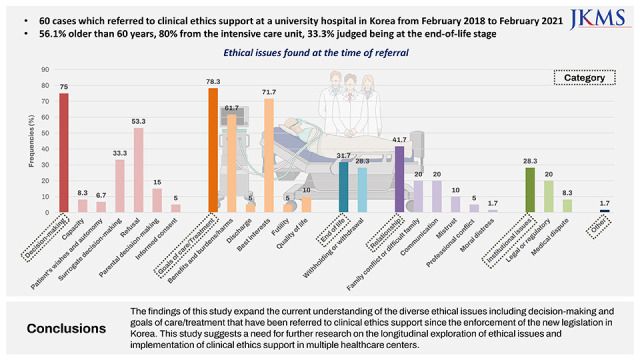
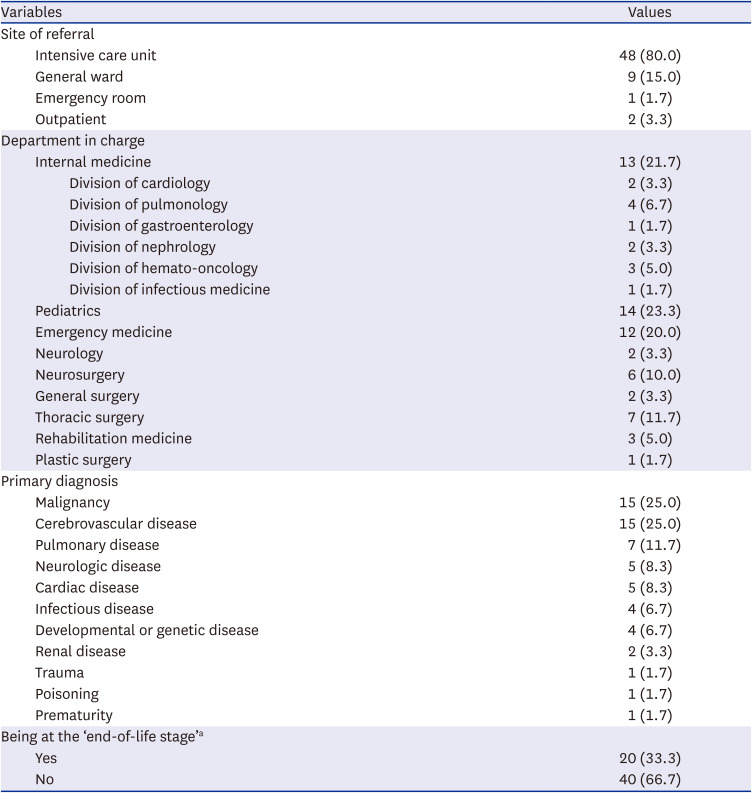
Table 2 depicts the clinical characteristics of the 60 cases at the time of referral. The intensive care unit was the most common site of referral (80.0%). The top five common primary diagnoses were malignancy (25.0%), cerebrovascular disease (25.0%), pulmonary disease (11.7%), neurologic disease (8.3%), and cardiac disease (8.3%). Only 33.3% of the total cases were judged as being at the end-of-life stage at the time of referral.
Table 2
Clinical characteristics at the time of referral (N = 60)
Decision-making-related characteristics of the cases
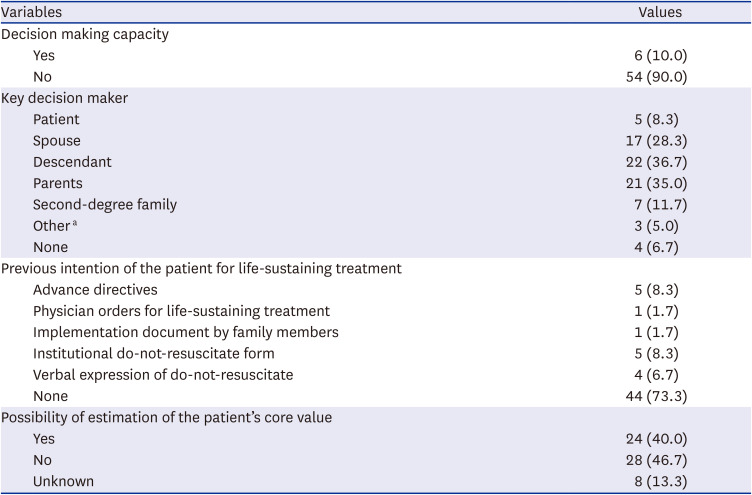
Table 3 presents the characteristics related to decision-making capacity. At the time of referral, 90.0% of the cases did not have a decision-making capacity. Only 26.7% of the cases had a previous intention of the patient’s LST decision. The preference or value of the patients was assumed only in about 40.0% of the cases.
Table 3
Decision making-related characteristics at the time of referral (N = 60)
Ethical issues faced by clinicians at the time of referral
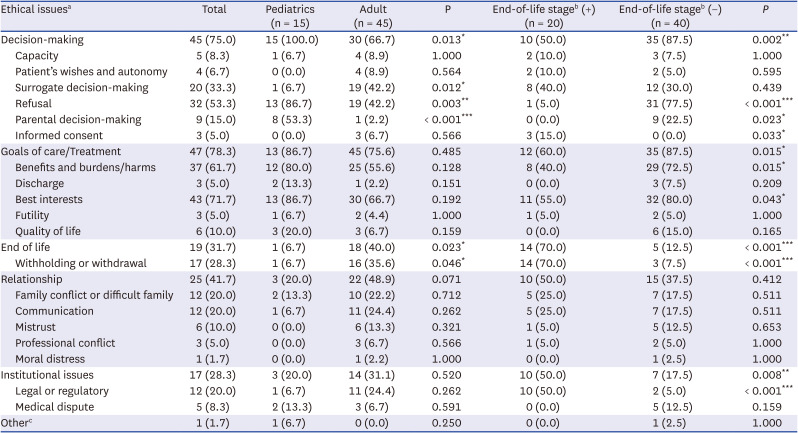
The ethical issues that arose in each case are listed in Table 4. The main header categories of ethical issues identified in order of most to least frequent were goals of care/treatment (78.3%), decision-making (75.0%), relationship (41.7%), end-of-life (31.7%), and institutional issues (28.3%). The most common subcategories of ethical issues were best interests (71.7%), benefits and burdens/harms (61.7%), refusal (53.3%), surrogate decision-making (33.3%), and withholding or withdrawal (28.3%).
Table 4
Ethical issues found at the time of referral by age group and judgment of end-of-life stage (N = 60)
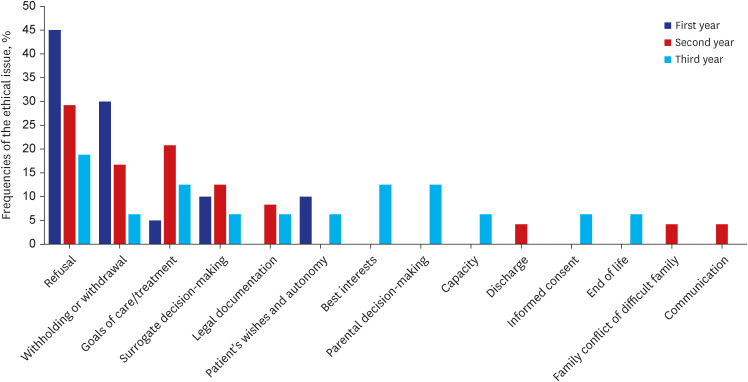
The key ethical issues identified in each case are in line with the distribution of the overall ethical issues (Supplementary Table 2). In the total cases, refusal was the most common (31.7%) key ethical issue. Fig. 2 illustrates the frequencies of each key ethical issue by year. In 2018, refusal (45.0%) and withholding or withdrawal (30.0%) of LST accounted for three-quarters of the key ethical issues, while the proportion of the two issues decreased over time. In contrast, the various key ethical issues were distributed evenly in 2020.
Ethical issues at the time of referral by age group and by judgment of the end-of-life stage
Ethical issues differed between the pediatric and adult groups as shown in Table 4. The category “decision-making” and the subcategories “refusal” and “parental decision-making” were significantly higher in the pediatric group, while the subcategory “surrogate decision-making” was higher in the adult group. In the adult group, the frequency of end-of-life-related ethical issues was significantly higher than in the pediatric group. The distribution of the key ethical issues also differed between the two groups (Fig. 3A).
Fig. 3
Key ethical issues found at the time of referral by age group (A) and by judgement of the end-of-life stage (B).
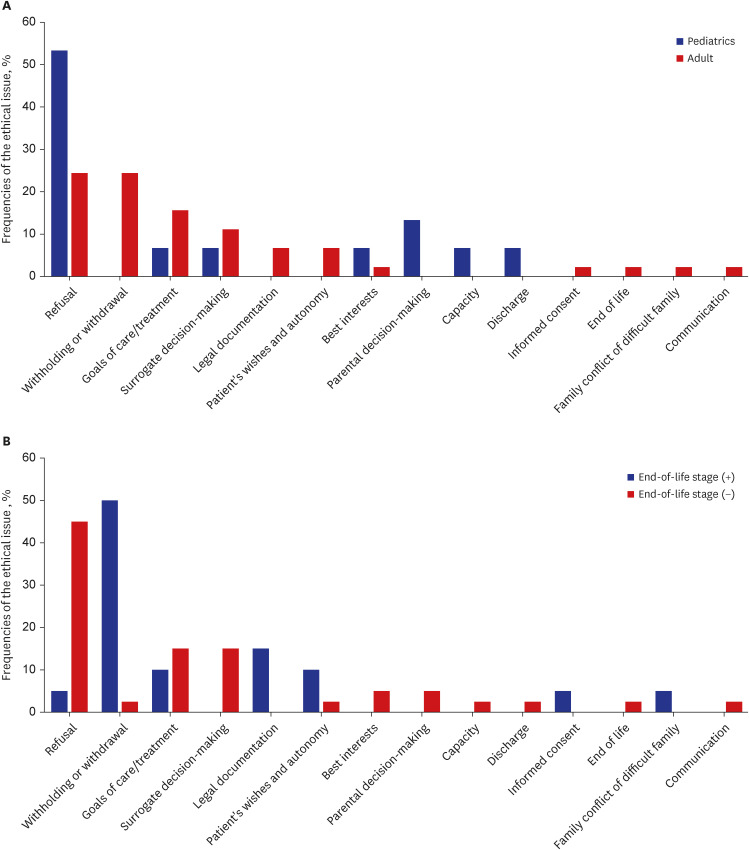
Similarly, ethical issues differed by the judgment of the end-of-life stage at the time of referral (Table 4). While the category “decision-making” and “goals of care/treatment” were more prominent in cases not at the end-of-life stage, the category “end-of-life” and institutional issues were more prominent in cases at the end-of-life stage. Refusal and withholding or withdrawals were the two key ethical issues with the largest difference between the two groups (Fig. 3B).
CES process and post-consultation outcomes
For the 60 cases analyzed, CES responded to them depending on the ethical issues and clinical situations. For three cases (5.0%), the secretary provided the relevant CES information. For 11 cases, the ethics consultation team delivered the consultation reply. Formal ethical recommendation replies were delivered for 16 cases (26.7%) and 30 cases (50.0%) by the sub-committee and the institutional ethics committee, respectively. The average (standard deviation) time from the receipt to the final response of CES was 0 (0), 1.58 (1.74), 5.27 (5.49), and 4.75 (5.02) days for information provision, ethics consultation team operation, sub-committee operation, and committee operation, respectively.
Excluding two patients who were referred from outpatient clinic, a total of 58 cases (55 patients) were hospitalized and discharged. For those 55 patients, the median length of hospital stay and the time from referral to discharge was 40 days (range, 3 to 1,187 days) and 17 days (range, 0 to 784 days), respectively. Among them, 54.5% (n = 30) died during admission, 27.3% (n = 15) were discharged to other hospitals, and 18.2% (n = 10) were discharged to go home. Of the 15 patients who were discharged to other hospitals, 80.0% (n = 12) went to nursing hospitals and 20.0% (n = 3) to other secondary or tertiary hospitals.
DISCUSSION
The current descriptive study investigated the ethical issues identified in the ethical cases referred to CES in a tertiary university hospital in Korea. To our knowledge, this is the first study to demonstrate ethical issues in CES cases after the enactment of the LST Decisions Act in Korea. In this study, decision-making and goals of care/treatment were the commonly identified issues at the time of referral. Regarding specific key ethical issues, refusal, best interest, benefits and burdens/harms, and surrogate decision-making were predominantly identified in the cases, while decision-making capacity and autonomy issues were not dominant. The major ethical issue categories identified in this study are similar to many of the issues identified in previous studies conducted in the United States.614 This finding is not surprising when one considers that CES has only been implemented with the enactment of the LST Decisions Act in Korea and that most of the cases were referred by doctors who mainly manage decision-making and discuss goals of care/treatment with patients and surrogate decision-makers. Regarding the key ethical issues, refusal and withholding or withdrawal accounted for three-quarters of all issues in the first year. This finding implies that despite the enactment of the LST Decisions Act, it might still be difficult and confusing to apply and interpret the Act in clinical practice without CES. However, as the years progressed, the frequency of the two issues (refusal and withholding or withdrawal) decreased, and instead, the diversity of ethical issues has increased. In addition to the capability of the interpretation of the Act, it can be postulated that the stable operation of the hospice palliative care team over the years attribute to a reduction in LST-related concerns, which are typically handled more in palliative care teams than in CES. Similarly, Gorka et al.19 presented that the ethical issues start with end-of-life-related concerns and later move on to various issues in longitudinal changes in the settlement of ethics consultation. Although Gorka et al.19 did not provide a clear explanation for these changes, the diversity of requestors, specialist areas, and underlying diseases of patients may influence the diversity of issues. To validate the associated factors, additional prospective longitudinal investigations are required.
In this study, the ethical issues identified in pediatric cases, which accounted for 25% of the overall cases, were distinct from those identified in adult patients. The category of “decision-making” was more pronounced in pediatric patients while the “end-of-life” category was less observable in pediatric patients than in adult patients. Regarding the key ethical issues, “refusal” was the most dominant issue in pediatric patients. Due to the high level of plasticity and prognostic uncertainty in pediatric patients,20 clinicians may face challenges in judging the end-of-life stage and regard the refusal of medical procedures in critically ill patients as a disagreement in treatment decision making rather than withdrawal of LST and end-of-life issue. Regarding this unique situation, further research is required on identifying optimal CES approaches toward pediatric cases in Korea.
The results of this study further indicated that two-thirds of the cases were not at the end-of-life stage at the time of referral. Considering that 75% of the overall cases comprised non-cancer patients with difficulty in making judgments at the end-of-life stage due to relatively high prognostic uncertainty compared to cancer patients in general, the findings can be explained based on this factor.21 According to a survey of Korean doctors after the implementation of the LST Decisions Act, high prognostic uncertainty may influence the decision-making of patients and their families.12 End-of-life issues and institutional issues were predominant in the cases assessed at the end-of-life stage, whereas goals of care/treatment and decision-making were the prevalent ethical issues in cases not at the end-of-life stage. Although the institutional ethics committee should mainly address issues related to the LST decision implementation in cases at the end-of-life stage according to the LST Decisions Act,7 the current findings suggest that CES may need to be consulted for cases beyond the LST Decisions Act in clinical practice.
In addition to the ethical issues identified, the characteristics of the cases referred to CES can provide further insight into the development of a robust CES system in healthcare facilities. First, several cases analyzed in this study indicated the lack of decision-making capacity or the inability to identify or estimate the patient’s wishes. Regarding the manner of surrogate decision making on their behalf, Korea has a different stance than countries such as the United States, the United Kingdom, and Taiwan.22 The two specific distinctions are whether the Act permits the designation and intervention of legal representatives in LST decisions and if clinicians or ethics committees may participate based on the best interests of patients. Korea restricts both, and only closest family members can act as proxies. However, the fast changes in family structure23 illustrated here indicate that these restrictive constraints do not reflect reality. In addition to existing literature demonstrating that LST decisions for unfriended patients are still in a gray area,242526 the authors propose regulatory changes to allow the ethics committee to make stronger recommendations than simple advice in cases where patients’ autonomy is difficult to appreciate.2425
In addition, in this study, 80% of the cases were referred from the intensive care unit, which is a complex healthcare setting characterized by ethically burdensome decision-making and high levels of uncertainty and conflicts.27 Integration of CES in the intensive care unit is often more challenging than that in general wards or outpatient clinics because of unstable patient status that requires urgent medical processes28 despite the positive effect of ethics consultation on resource utilization and user experience.29 Therefore, CES aimed at rapid response, such as employing the ethics consultation team or consultant, may be useful in the intensive care unit setting.30
We found that the time from referral to response varied depending on the type of CES response. It suggests that, depending on the pace with which problems must be resolved, CES may have to respond differently. Furthermore, the committee or subcommittee’s response to three-quarters of the cases is seen as a significantly more positive outcome when compared to the fact that most of them were difficult to bring before the committee prior to the LST Decision Act.13 Nearly half of the requested patients died during hospitalization, which is similar with findings of early phase of ethics consultation in the United States19 and is mostly attributable to the request for end-of-life-related issues.
Although the present study reveals important findings, it has several limitations. First, the data were collected from a single tertiary hospital and the small sample size produced low statistical significance. Therefore, future multi-center research with more cases is required for better generalizability. Second, this study analyzed CES cases for three years, which may not be sufficient for drawing conclusions applicable in clinical practice. The ethical issues referred to CES analyzed in this study may not represent the ethical issues raised by clinicians of a university hospital after the enactment of the LST Decisions Act. Third, possible selection bias inherent to the retrospective design of the study may affect the interpretation of the results.
Regardless of these limitations, this study is significant in that it provides valuable insight into the ethical issues referred to CES in Korea, which faces a paucity of data1631 in this regard since most of the studies on CES have been conducted in Western countries such as the United States and European countries.461419 Furthermore, the ethical issues referred to ethics consultation or clinical ethics committees have tended to increase and have become diversified,19 which may be in line with societal changes, changes in hospital management, and legislative events. To examine the ethical issues emerging in CES longitudinally, these issues and concerns should be prospectively investigated using consistent coding methods such as codebooks across multiple hospitals operating clinical ethics committees in Korea.
In conclusion, this study found that diverse ethical issues including decision-making, and goals of care or treatment have been referred to CES and these issues differ depending on age and the judgment of the end-of-life stage. The findings of this study aim to expand the current understanding of ethical issues since the enforcement of the LST Decisions Act in Korea and suggest a need for further research on longitudinal examination of ethical issues and implementation of CES in multiple healthcare centers.
 XML Download
XML Download