

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Knowledge of craniocervical junction (CCJ) abnormalities and their morphology is essential for clinicoradiological studies. The ponticulus, a bony bar arising from the lateral mass of the atlas, when fully developed, transforms the groove of the vertebral artery (VA) into a canal (arcuate foramen). These dysmorphisms may be clinically silent7). However, in asymptomatic individuals, they may become dangerous in the context of trauma6), or provoke slight troubles during specific diagnostic or surgical procedures1339). Occipitalization of the atlas (also known as atlanto-occipital assimilation) is thought to be a manifestation of so-called occipital vertebrae (i.e., incomplete segmentation between the atlantal and occipital bones)11). Occipitalization is the most common anomaly of the CCJ, with a prevalence of 0.08–3.63% of the population21436). Because of the rare prevalence of occipitalization of the atlas, the anatomical changes associated with this condition have not yet been fully explored. Congenital defects of the posterior arch of the atlas are uncommon, but their characteristics have been well described. In emergency departments, it is important to distinguish this variant anatomy from fracture and/or dislocation. Although X-ray imaging or computed tomography (CT) findings of congenital defects of the posterior arch of the atlas have been reported, 3-dimensional (3D) CT features of this anomaly have not been described in detail.
Understanding the anatomical basis of CCJ anomalies is important when performing CCJ region surgeries. In this report, we describe the incidence and anatomical features of arcuate foramina, occipitalization of the atlas, and congenital defects of the posterior arch of the atlas. We review and discuss these anomalies in the context of surgical treatment.
MATERIALS AND METHODS
We conducted a retrospective review of cervical 3D CT. We excluded 3D CT of patients from outside the catchment area of the hospital, including foreigners. These included patients who presented at our hospital due to cervical problem (cervical trauma, neck pain, degenerative cervical disease) between November 2011 and August 2014. An Aquilion Prime 160-slice CT scanner (Toshiba Medical Systems Corporation, Otawara, Japan) was used for 173 patients and an Aquilion CXL edition 128-slice CT scanner (Toshiba Medical Systems Corporation, Otawara, Japan) was used for 856 patients. In total, 1029 scans comprising those of 639 male patients and 390 female patients were reviewed. The age of the patients ranged from two years and two months to 88 years (49.03±15.55).
Parameters for the 3D CT acquisition were as follows : 140 mm field of view, 120 kVp, 150 mA, 0.5 mm section thickness, and 0.3 mm interval. The scan range was from the mid-body of the T2 vertebra to the base of the occiput. Axial and sagittal images (window level 60/window width 320) with 2 mm or 3 mm section thickness and a bone axial and sagittal images setting (window level 350/window width 2700) with 2 mm or 3 mm section thickness were transferred to a picture archiving and communication system (PACS). A series of 12 3D surface rendering reconstruction images around the vertical rotational view at every 20° was generated using software provided with the Aquilion Prime or Aquilion CXL edition scanners.
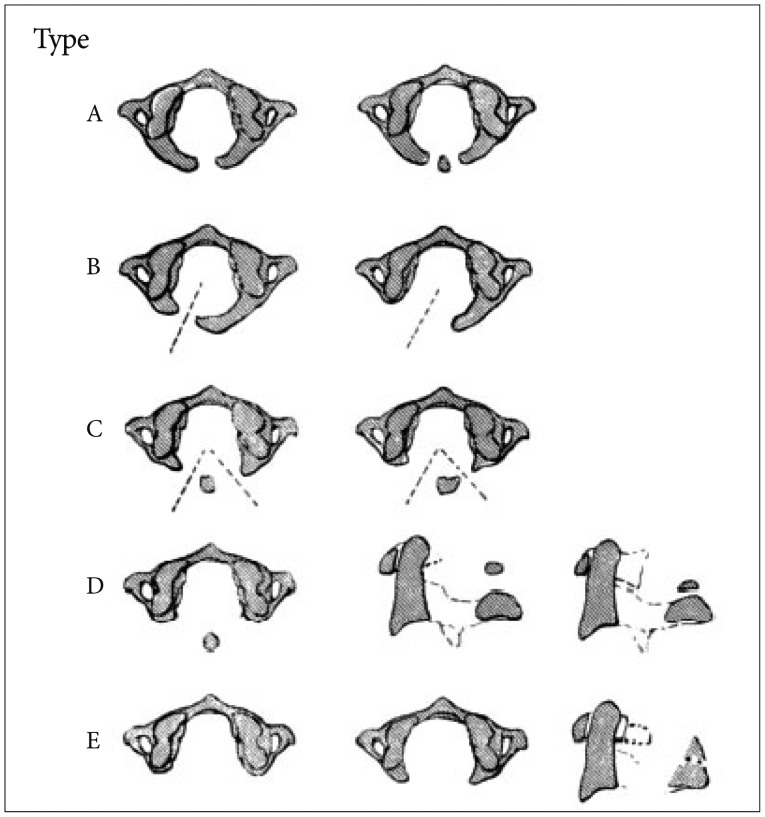
Arcuate foramina were classified as either partial or complete and left and/or right. We did not include bony protrusion due to noticeable impression for VAs as partial type. Partial type was considered as partial arcuate foramen which was noted as a distinct bony spicule extending from the superior articular facet overhanging the dorsal arch. Assimilation of the atlas was classified in accordance with criteria specified by Mudaliar et al.23). Zone 1 fusion involves the anterior arch of the atlas in front of the lateral masses. Zone 2 fusion primarily involves the lateral processes. Zone 3 fusion involves the posterior arch of the atlas behind the lateral masses. The final type involves a combination of zones. Posterior arch defects of the atlas were classified in accordance with the criteria specified by Currarino et al.5), who classified aplasia and cleft into five forms : A) a fissure or small gap because of failure of posterior midline fusion of the two hemiarches, B) cleft or absence of one or two arms of the posterior arch, C) bilateral defects with preservation of the most dorsal part of the arch, D) absence of the posterior arch with a persistent posterior tubercle, and E) absence of the entire arch, including the tubercle (Fig. 1).
RESULTS
Arcuate foramen
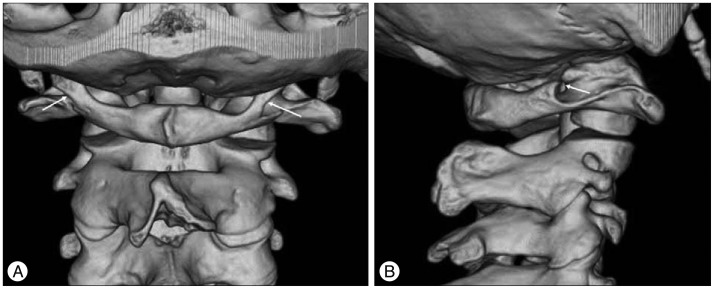
One hundred and eight vertebrae (108/1029, 10.5%, 78 males, 30 females, age 16–81 years, 48.28±14.69 years) showed the presence of a bony exostosis from the posterior margin of the superior articular facet (Fig. 2). Bilateral arcuate foramina were found in 41 vertebrae, and in the remaining 67 vertebrae the occurrence was unilateral (right 31, left 36). Right-side arcuate foramina were partial on 18 sides and complete on 54 sides. Left-side arcuate foramina were partial on 24 sides and complete on 53 sides.
Occipitalization of the atlas
There was one case of atlas assimilation. The type of this assimilation included a combination of zones. An anomalous odontoid process and foramen magnum were observed. C2 and C3 fusion was associated with this anomaly (Fig. 3).
Defect of posterior arch of the atlas
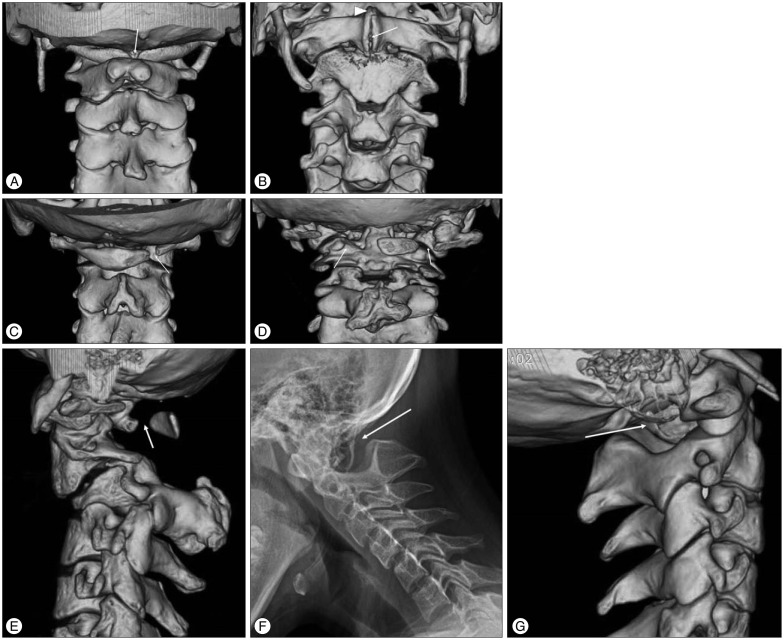
In our study, a defect of the atlantal posterior arch was found incidentally in 12 patients (1.17%, nine male patients and three female patients, range 14–69 years) (Fig. 4). Nine of these patients (9/1029, 0.87%) had a type A posterior arch defect. We also identified one type B, one type D, and one type E defect. One patient with a type A posterior arch defect had an anterior arch defect.
DISCUSSION
Arcuate foramen
The ponticulus posticus (arcuate foramen), or "little posterior bridge," is an ossification of the oblique atlanto-occipital ligament superior to the VA groove of the atlas. An arcuate foramen has been reported with an incidence of from 1.14% to 37%202224353638). In this study, one hundred and eight vertebrae (108/1029, 10.5%) showed the presence of a bony exostosis from the posterior margin of the superior articular facet.
An arcuate foramen is usually regarded as a simple anatomical variant. However, compression of the nervous and vascular structures passing through the foramen may result in a combination of symptoms forming a picture of vertebrobasilar insufficiency17). This consists of cervical migraine37), neurosensory-type hearing loss16), neck pain, vertigo, shoulder/arm pain and, in some instances, even loss of postural muscle tone and consciousness432). Surgical excision of such an arcuate foramen appears to alleviate these symptoms18). Penning25) considers that there is more to the mechanism than pure arcuate foramen compression, identifying trauma as a trigger factor. However, whether such trauma leads to direct VA injury and musculoskeletal compromise, which in turn leads to VA compression, is unclear37).
Cushing et al.6) found an arcuate foramen in 8 of 11 patients with VA dissection and occlusion. The site of arterial injury was at the level of this bony variation in all cases. Because more than 50% of head rotation occurs at the atlantoaxial joint, the VA is most vulnerable to compression and stretching at this level. Therefore, additional compression/tethering of this vessel by an arcuate foramen may increase its predisposition to injury. During flexion of the neck, the VA glides superiorly and anteriorly relative to the posterior arch, and this is more likely to occur on the posterior lateral masses of the atlas than at more caudal sites in the neck19).
When the VA courses above the posterior arch of the atlas, the placement of lateral mass screws is relatively safe10), however, the risk may increase significantly with any anomalous course of the VA. Indeed, the abovementioned arcuate foramen would place the VA in the path of any atlas lateral mass screw. Young et al.39) have commented that the arcuate foramen may be mistaken for a widened posterolateral aspect of the posterior arch of the atlas, so that placement of lateral mass screws at C1 can be difficult. When an arcuate foramen is found, screw fixation through the lateral mass of the atlas is not feasible, and other modalities of internal fixation must be pursued13). For example, C1–2 transarticular screw fixation, the C1 dorsal arch as an entry point for C1 screw placement, and skip C1 screw fixation and to extend the level of fixation proximally or distally can be alternative method12). Because arcuate foramina are not rare, the need for identification of this anomaly on preoperative radiographs and, particularly, high-resolution CT cannot be overemphasized1).
Occipitalization of the atlas
Occipitalization of the atlas (also known as atlanto-occipital assimilation) is thought to be a manifestation of so-called occipital vertebrae (that is, incomplete segmentation between the atlantal and occipital bone)11). Occipitalization of the atlas is caused by failure of segmentation between the fourth occipital sclerotome (proatlas) and the first cervical sclerotome during embryonic development21). The incidence of occipitalization of the atlas ranges from 0.08% to 3.63%21427). In this study, the incidence of occipitalization of the atlas was 0.097%. The synostosis has been classified into four types based on the zones of the atlas fused with the occiput23). Zone 1 fusion involves the anterior arch of the atlas in front of the lateral masses (20% of cases). Zone 2 fusion primarily involves the lateral processes (17%). Zone 3 fusion involves the posterior arch of the atlas behind the lateral masses (13%). Combinations of zones were seen in over 50% of patients. In our patient, combinations of zones of atlanto-occipital fusion were seen (Fig. 2).
Occipitocervical synostosis results in a shift of the first mobile segment between the skull and spine to the C1–2 junction. This causes stress and a restricted range of movement, as a result of which there may be overstretch failure of the supporting myoligamentous structure, leading to a gradual loosening of the atlantoaxial joint with progressive atlantoaxial subluxation23). Compression of the spinal cord or the brain stem because of occipitocervical synostosis can produce signs and symptoms varying from a simple headache to a full blown neurological syndrome31). Compression of the VA can compromise blood flow to the brain. Our patients demonstrated no symptoms associated with occipitalization of the atlas.
Atlantal occipitalization per se requires no treatment; however, when symptoms of neural compression or spinal instability develop, surgical intervention, such as CCJ decompression and/or fusion, may be required26). Most patients with occipitalization of the atlas probably remain asymptomatic and undetected. For those that develop symptoms, the onset is usually in the third or fourth decade. The surgeon should also recognize that manipulation of the cervical spine during surgical positioning may place patients with atlantal occipitalization in greater jeopardy of suffering VA occlusion1929). According to Wang et al.36), anomalies of the VA occur more often in cases with occipitalization of the atlas. Wang et al.36) reported four distinct types of VA at the CCJ with occipitalization of the atlas. Type 1 : the VA courses medially after leaving the transverse foramen of the axis, enters the spinal canal below the occipitalized C1 posterior arch, and enters the foramen magnum. The course of the VA is below the occipitalized C1 lateral mass. Type 2 : the VA courses medially after leaving the transverse foramen of the axis, enters the spinal canal below the occipitalized C1 posterior arch, and enters the foramen magnum. The course of the VA is on the posterior surface of the occipitalized C1 lateral mass, or forms a curve on it. Type 3 : the VA ascends laterally after leaving the transverse foramen of the axis, passes through the transverse foramen of the atlas (if present), enters an osseous foramen created between the fused atlas and occiput, and then reaches the cranium. The anomalous pathway has its internal opening at the external edge or anterior part of the occipitalized C1 lateral mass. Type 4 : the VA is absent on one side of the CVJ. In our patients, we could not identify the type of either VA.
Congenital defect of the posterior arch of the atlas
The atlas normally develops from the three primary ossification centers : one midline anterior center, which forms the anterior arch, and two lateral centers for each lateral mass. It develops during the seventh week of gestation334). Two centers at the lateral masses extend posteromedially to form the posterior neural arch by year 4. Ossification of the anterior neural arch occurs posterolaterally from the midline anterior center to the lateral mass and is complete at 7 years of age8). Rarely, in only 2% of the population, a fourth center appears, which results in the posterior tubercle of the atlas and unites with the lateral masses of the atlas. Posterior atlantal arch defects are attributed to the defective or absent development of the cartilaginous preformation of the arch rather than a disturbance of the ossification9). This is supported by findings at autopsy or intraoperatively where connective tissue bridges the bony defect27). Isolated posterior arch clefts are relatively common, and are reported in 1.5–5% of the population359). In this study, the incidence of congenital defects of the posterior arch of the atlas was 1.17%.
Developmental anomalies of the posterior arch of the atlas range from simple clefts to absence of the entire arch. In 1994, Currarino et al.5) classified aplasia and cleft in five forms : A) a fissure or small gap because of failure of the posterior midline fusion of the two hemiarches, B) cleft or absence of one or two arms of the posterior arch, C) bilateral defects with preservation of the most dorsal part of the arch, D) absence of the posterior arch with a persistent posterior tubercle, and E) absence of the entire arch, including the tubercle. Currarino's classification is used in most of the literature. Type A clefts according to Currarino's classification occur in proximately 4% of the population. Over 90% of defects are Type A. Currarino et al.5) estimated that 0.69% of the general population harbor Types B–E.
Patients are most commonly asymptomatic, although the defect can cause chronic cervical pain, headache, and Lhermitte's sign28). Cervical myelopathy is also possible, and has been reported in several cases1528), especially with types C and D of Currarino's classification, which are both associated with the presence of a free-floating posterior osseous fragment. In these cases, the presence of a posterior tubercle may cause impingement on the cord, which may result in myelopathy or possibly cord contusion. Richardson et al.27) suggested that the symptoms were secondary to compression of the cord by the inward mobility of the isolated posterior bony fragment during extension of the cervical spine. Sharma et al.30) were the first to document true movement of the bony tubercle with neck extension. Torreman et al.33) reported that stenosis of the atlas and axis was observed because of slight abnormal movement and hyperostosis of the persistent posterior tubercle and hypertrophy of the posterior ligaments between the atlas and axis. Moreover, Torreman et al.33) suggested that this might explain the delayed occurrence of symptoms of this congenital partial agenesis. The cumulative effects of minor cervical traumas may cause myelopathy. In our study, all 12 cases with defects of the atlantal posterior arch were found incidentally. Flexion and extension X-ray films of the cervical spine in one patient with a Type D defect revealed no movement of the posterior tubercle of the atlas. In this study, one case with defects in both anterior and posterior atlantal arches, anterior arch have incomplete arch defect (Fig. 4A, B). We think that this anatomical feature may contribute to asymptomatic presentation in patient with defect of both atlantal arches.
CONCLUSION
An arcuate foramen is not an uncommon anomaly. The presence of this anomaly should be carefully assessed before screw insertion into the lateral mass of the atlas. Preoperative 3D CT should be conducted before atlas lateral mass screw insertion. Occipitalization of the atlas considerably changes the anatomy of the upper cervical spine and CCJ. Preoperative diagnosis using 3D CT is of paramount importance for detecting these changes and avoiding neurovascular injury during surgery. Despite the low incidence of defects of the posterior arch of the atlas, we recommend that surgeons keep the possibility of its existence in mind when considering traumatic atlantoaxial subluxation and atlas fracture.

 XML Download
XML Download