

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since the first case was identified three years ago, the virus responsible for coronavirus disease 2019 (COVID-19), severe acute respiratory syndrome-coronavirus-2, has swiftly spread globally. Confirmed cases of COVID-19 were 768,983,095 and 6,953,743 deaths were reported globally as of August 2, 2023.1 During public health crises, such as infectious disease outbreaks, mental health issues such as depression, anxiety, and post-traumatic stress disorder tended to increase in prevalence, even though the primary focus is on physical health consequences.2 Stress, anxiety, and depression have become alarmingly prevalent in the general population during the COVID-19 pandemic, with rates reaching as high as 29.6%, 31.9%, and 33.7%, respectively.3 Moreover, previous research has examined the distinct psychological effects of the COVID-19 pandemic on groups that are particularly vulnerable during such times, including healthcare workers, individuals with physical comorbidities, children and adolescents, and the elderly.4
In this pandemic, healthcare professionals suffer from work-related stress. Due to their essential role on the frontlines of the pandemic, they are a group that has been significantly affected by the COVID-19 pandemic. They are responsible for diagnosing and treating patients, which inevitably exposes them to their patient’s pain and suffering, leading to physical exhaustion and severe psychological conditions. According to the literature, healthcare workers, including physicians, nurses, and allied health workers, are experiencing higher levels of depression, anxiety, and post-traumatic stress disorder than the general population.5 Among the hospital personnel, fear-related symptoms, diminished wellness, substandard quality of life, and acute stress were the most commonly reported.6 Fear of contracting and transmitting the virus,5 adds to the challenges faced by healthcare workers during this pandemic in addition to their already demanding workload.
One of the growing concerns for healthcare workers’ mental health is the grief reaction, a relatively neglected research topic. The grief resulting from COVID-19 demands greater attention and consideration. According to a study, the intensity of grief following a COVID-19-related death is higher than that following other types of loss, such as natural causes death.7 This finding is particularly concerning because acute grief responses during the initial months of mourning can increase the likelihood of experiencing prolonged grief.8910
A report highlights how healthcare workers are grieving over the deaths of patients during the COVID-19 pandemic.11 According to the study, the pandemic has created unprecedented fear and anxiety among healthcare workers and intensified pre-existing clinician “professional grief” issues in several ways (e.g., the sheer number of COVID-19 deaths, the tasks, and situations in which they were unprepared, the circumstances under which patients are dying that limit the availability of in-person care). Notably, these factors increase the likelihood that healthcare workers will experience complicated or prolonged grief.11 The prevalence rates of grief among healthcare professionals demonstrate its significance. The pooled prevalence rate of grief symptoms and disorder was determined to be 45.1% (95% confidence interval: 32.6% to 57.5%) and 46.4% (95% confidence interval: 37.4% to 55.5%), respectively. However, a significantly higher prevalence of grief symptoms and disorder was observed among healthcare workers, amounting to 56.6% and 57.0%, respectively,121314 and 57.6% of the study’s subjects were identified as experiencing complicated grief during the pandemic.15
As part of the COVID-19 pandemic, the Pandemic Grief Risk Factors (PGRFs) were developed as a self-report tool to examine the composite severity of distinctive grief risk factors among people who had experienced their loved one’s death.16 However, there is no rating scale for the experience of healthcare workers who witness the deaths of patients they cared for. Although the developers of the original PGRF used the term “loved” as well as “significant,”16 according to the paper that described characteristics of the study participants,17 they were individuals who had lost “a significant person” due to COVID-19. Moreover, 15.3% and 13.0% were acquaintances and close friends, respectively.17In this context, we believed that this scale could be applied to a group of individuals who had lost people in a relationship, not only those they loved but also those with generally deep emotional connections. In this study, we examined the reliability and validity of the PGRF scale among healthcare professionals who witnessed patients’ deaths during the COVID-19 pandemic. In addition, we explored the relationship between PGRF, work-related stress, and pandemic grief reactions.
METHODS
Participants and procedure
An online survey was conducted among healthcare workers at Asan Medical Center between June 2nd and 10th, 2022. This is a continuation of the previous study.18 We distributed the survey link via the hospital’s intranet to recruit doctors and nursing professionals who witnessed the deaths of patients they cared for during the last two years. They voluntarily participated in this anonymous online survey, and we rewarded their participation with a five-dollar gift coupon. The survey form included questions on participants' demographic information about age, sex, occupation (doctors or nursing professionals), years of employment, marital status, and shift work status. In addition, questions on COVID-19-related experiences, such as infection, quarantine, and vaccination, were included. We also asked whether they witnessed the deaths of the patients they cared for and if they were related to COVID-19. The survey form was developed per The Checklist for Reporting Results of Internet E-Surveys (CHERRIES), and its functionality reviewed by the investigator (S.C.) before implementation.
The sample size was estimated to be 300 based on Central Limit Theorem, with 30 samples allocated to 10 cells (doctors vs. nursing professionals X five groups of ages).19 However, we collected 293 respondents and analyzed them using responses from 267, excluding 26 who had not witnessed patients’ deaths in the past two years.
Symptom assessment
To rate each rating scale based on the time participants witnessed death, they were asked to recall their psychological status during the first two weeks following witnessing the patient’s death.
PGRF scale
The PGRF is a self-report scale that explores the risk factors for dysfunctional grief following a COVID-19-related loss.16 Originally, the PGRF was developed among adults (N = 831) who had lost significant others to COVID-19. It contains 10 items that can be rated on a 4-point scale, from zero (not at all) to three (nearly every day). The Korean version of the PGRF was developed using translation and back-translation methods. A bilingual expert translated the original PGRF scale into Korean from English. A second bilingual expert reverse-translated the Korean text back into English. A third party then compared the original and back-translated versions of the PGRF scale and verified them.
Pandemic Grief Scale (PGS) for healthcare workers
Initially, a PGS was developed to assess the effects of grief on individuals during the COVID-19 epidemic,17 and it was later adapted for healthcare workers.20 The PGS comprises four items rated on a 4-point scale, ranging from zero (not at all) to three (almost every day), based on recent experiences. An overall PGS score of seven indicates probable dysfunctional grief associated with COVID-19. This study, applied the Korean version of the PGS for healthcare workers21; The Cronbach’s alpha in this sample was 0.842.
Stress and Anxiety to Viral Epidemic-3 items (SAVE-3)
The SAVE-3 rating can be used to assess healthcare workers’ work-related stress due to the COVID-19 viral epidemic.22 It is a subscale of the SAVE-9 scale developed to measure work-related stress and viral anxiety among healthcare workers during this pandemic.23 It consists of three items that can be rated on a 5-point scale ranging from 0 (never) to 4 (always). Higher total scores indicate that healthcare workers are more stressed due to viral infections. The Cronbach's alpha for this sample was 0.746.
Patient Health Questionnaire-9 items (PHQ-9)
The PHQ-9 rating scale was developed to measure depression.26 The nine items are rated on a 4-point Likert scale (0: not at all, 3: nearly every day), with a higher score indicating a more severe level of depression. In this study, we used the Korean version of the PHQ-925; This sample’s Cronbach’s alpha was 0.900.
Statistical analysis
First, we conducted a Confirmatory Factor Analysis (CFA) to explore the validity of the PGRF. Using the Kaiser-Meyer-Olkin (KMO) value and Bartlett’s test of sphericity, sampling adequacy and data suitability were assessed. As a single-factor model of the PGRF, a satisfactory model fit of the CFA was defined by a standardized root-mean-square residual (SRMR) value ≤ 0.05, a root-mean-square error of approximation (RMSEA) value ≤ 0.10, and comparative fit index (CFI) and Tucker Lewis index (TLI) values ≥ 0.90.2728 Multigroup CFAs were conducted to examine whether the PGRF can measure the risk of dysfunctional grief in the same way regardless of gender (male vs. female), occupation (doctors vs. nursing professionals), or having depression (PHQ-9 ≥ 10). Cronbach’s alpha and McDonald’s omega was used to examine the reliability. Using Pearson correlation coefficients (r), convergence validity with other pre-existing rating scales was assessed.
Second, we investigated whether the PGS and SAVE-3 were correlated with other rating scales using Pearson’s correlation analysis. A Linear regression analysis with enter methods was performed to explore expected variables for the pandemic grief of healthcare workers. Finally, to determine if the influence of work-related stress on pandemic grief is mediated by depression, anxiety, or grief risk factors, a mediation analysis was done with 2,000 resamples using the bootstrap method. For statistical analysis, SPSS version 21.0, AMOS version 27 for Windows (IBM Corp., Armonk, NY, USA), and Jamovi 2.3.25.0. were used.
Ethics statement
The study protocol (2022-0740) was reviewed and approved by the Asan Medical Center Review Board. The need for written informed consent was waived by the Institutional Review Board and the online survey was conducted only for those who consented to participate in the research through e-mails.
RESULTS
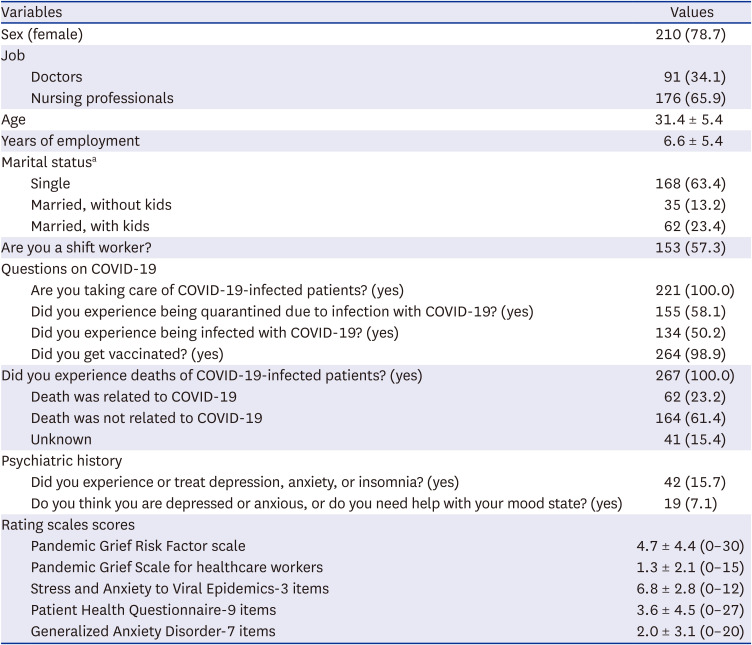
Table 1 shows the demographic characteristics of 267 healthcare workers who witnessed patients’ deaths within the past two years.
Table 1
Clinical characteristics of participants (N = 267)
Reliability and validity of the Korean version of the PGRF scale
The sampling was adequate and the data were suitable for CFA based on the KMO value of 0.898 and significant Bartlett’s sphericity (P < 0.001). Table 2 displays the item-level characteristics of the PGRF scale. According to the results of the CFA PGRF can be well-fit by a single-factor model (CFI = 0.924, TLI = 0.902, RMSEA = 0.085, SRMR = 0.051, Table 3). The range of factor loading values was between 0.503 and 0.692 (Fig. 1 and Table 2). Multigroup CFAs showed that the PGRF scale could measure risk factors for dysfunctional grief in the same way regardless of gender (male vs. female), occupation (doctors vs. nursing professionals), or having depression (PHQ-9 ≥ 10, Supplementary Table 1).
Table 2
Item properties of the PGRF among healthcare workers who witnessed patients’ death
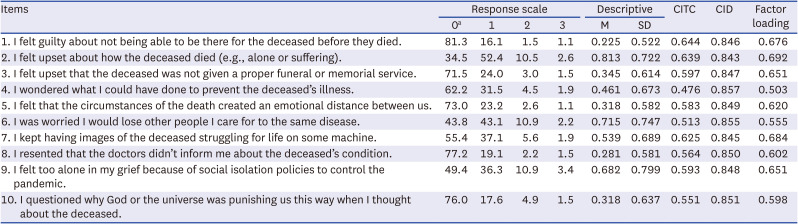
Table 3
Scale-level psychometric properties of the PGS for healthcare workers
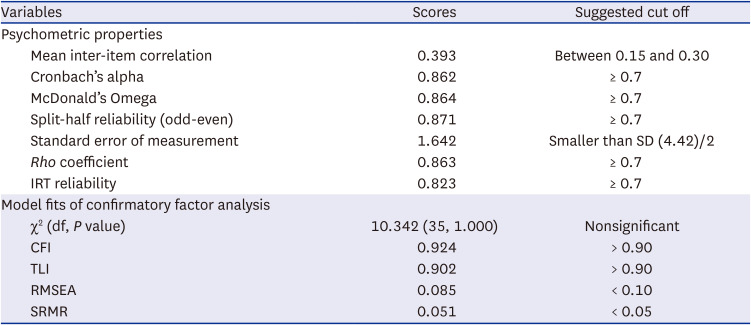
Fig. 1
Factor structure of the PGRF among healthcare workers who witnessed patient’s death.
PGRF = Pandemic Grief Risk Factor.
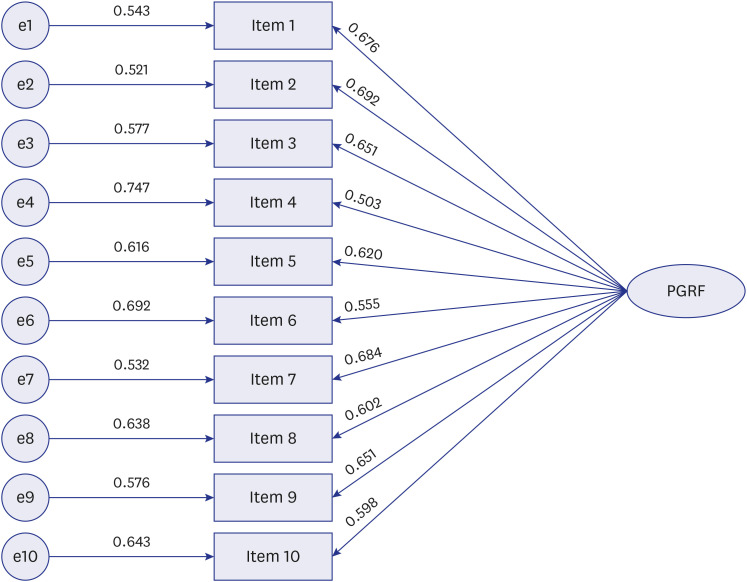
The PGRF showed good reliability of internal consistency based on Cronbach’s alpha of 0.862 and McDonald’s omega of 0.864 (Table 3). Concerning PGS (r = 0.77, P < 0.001), SAVE-3 (r = 0.038, P < 0.001), PHQ-9 (r = 0.62, P < 0.001), and GAD-7 (r = 0.065, P < 0.001), the good convergent validity of the PGRF was shown. Those with depression (PHQ-9 ≥ 10, t(265) = 7.07, P < 0.001) or generalized anxiety (GAD-7 ≥ 10, t(265) = 7.08, P < 0.001). had significantly higher PGRF total scores
Pandemic grief and work-related stress
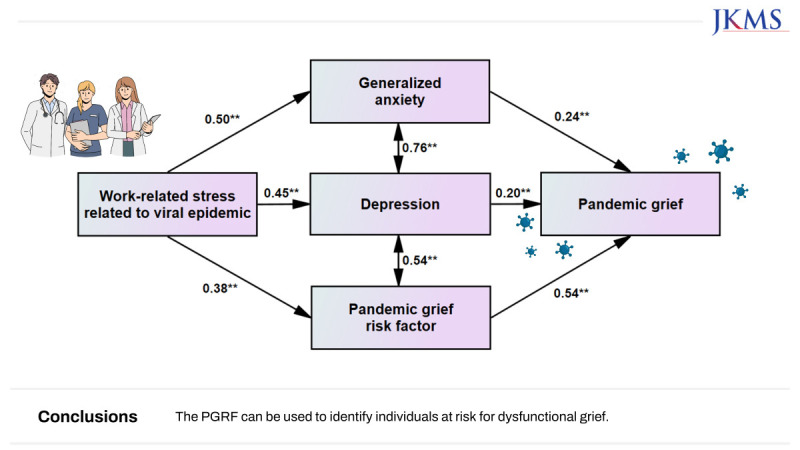
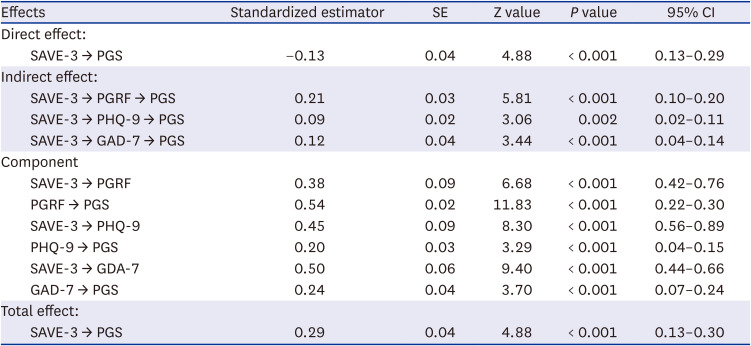
Significant correlations were found between the PGS and the SAVE-3 (r = 0.29, P < 0.001), PHQ-9 (r = 0.45, P < 0.001), and GAD-7 (r = 0.50, P < 0.001). The SAVE-3 was significantly correlated with PHQ-9 (r = 0.54, P < 0.001) and GAD-7 (r = 0.54, P < 0.001, Table 4). In linear regression analysis, the PGS was expected by PGRF (β = 0.54, P < 0.001), SAVE-3 (β = 0.13, P < 0.001), PHQ-9 (β = 0.20, P = 0.001), and GAD-7 (β = 0.24, P < 0.001, Table 5). In the mediation analysis, work-related stress of healthcare workers who witnessed patient deaths due to COVID-19 had a negative influence on their pandemic grief reaction. However, this association was mediated by PGRF, depression, and anxiety. Consequently, the mediation effect of work-related stress positively influenced pandemic grief (Fig. 2 and Table 6).
Table 4
Correlation coefficients of each variable among healthcare workers who witnessed patient’s death

| Variables | Age | PGRF | PGS | SAVE-3 | PHQ-9 |
|---|---|---|---|---|---|
| PGRF | 0.05 | ||||
| PGS | 0.03 | 0.77** | |||
| SAVE-3 | −0.11 | 0.38** | 0.29** | ||
| PHQ-9 | −0.05 | 0.62** | 0.45** | 0.54** | |
| GAD-7 | −0.08 | 0.65** | 0.50** | 0.54** | 0.81** |
Table 5
Linear regression analysis to explore variables that expect grief reaction of healthcare workers who witnessed a patient’s death (N = 267)

| Dependent variables | Included parameters | β | P value | Adjusted R2 | F, P value |
|---|---|---|---|---|---|
| PGS | Age | 0.02 | 0.593 | 0.67 |
F = 109.6 P < 0.001 |
| PGRF | 0.54 | < 0.001 | |||
| SAVE-3 | −0.13 | 0.002 | |||
| PHQ-9 | 0.20 | 0.001 | |||
| GAD-7 | 0.24 | < 0.001 |
Fig. 2
Mediation model showing the pathway from the effect of work-related stress in response to the viral epidemic (independent variables) on pandemic grief reaction (outcome) through pandemic grief risk factor, depression, and anxiety (mediator).
**P < 0.01.
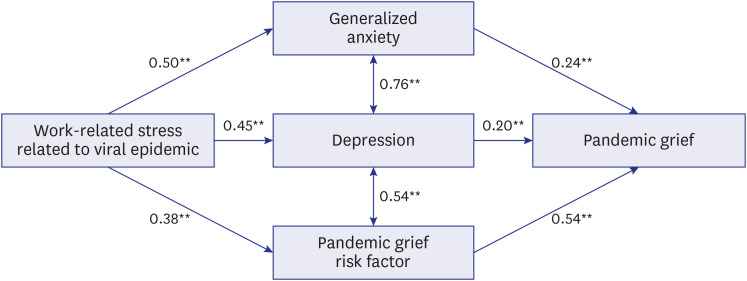
Table 6
Results of direct, indirect, and total effects on mediation analysis among healthcare workers who witnessed a patient’s death (N = 267)
DISCUSSION
We found that the Korean version of the PGRF can assess the risk of dysfunctional grief among healthcare workers who have witnessed the deaths of patients they cared for. The PGRF is a valid and reliable rating scale that can measure dysfunctional grief in the same way across sex, role, or psychiatric symptoms. A linear regression analysis found that their work-related stress reduced pandemic grief; however, it was also found that work-related stress aggravated pandemic grief by mediating grief risk, depression, or anxiety.
Due to the fact that PGRF was initially validated as a single-factor model,16 the CFA was conducted on the Korean version in the same manner. In this study, we observed that factor loading values of all items were greater than 0.5, so a single-factor model of the PGRF is deemed acceptable. The PGRF was developed to assist clinicians and researchers in identifying those risk factors that contribute to the development of dysfunctional grief symptoms and functional impairments due to COVID-19 loss. These risk factors correlate significantly with dysfunctional grief symptoms.16
In the mediation analysis, we observed that work-related stress in response to the viral epidemic influenced pandemic grief reactions with the mediation of PGRF, depression, and generalized anxiety. Healthcare workers who witnessed patients’ deaths during this pandemic might experience work-related stress in response to the viral epidemic, which influenced their grief reaction while witnessing patients’ deaths. Based on the SAVE-9 which evaluates work-related stress and viral anxiety, our previous study on nursing professionals working in COVID-19 inpatient wards revealed that work-related stress was positively associated with their grief reaction.23 Consistent with the previous finding, the SAVE-3 was significantly positively correlated with the PGS in a correlation analysis, and the SAVE-3 had a positive indirect influence on the PGS via the mediating effects of PHQ-9, GAD-7, and PGRF. Unexpectedly, however, SAVE-3 turned out to be a variable with a negative association to PGS, and SAVE-3 also had a direct negative influence on PGS. This seemingly contradictory relationship between the SAVE-3 and the PGS can be explained by multicollinearity or conditional dependence. In the first scenario, where there is a high correlation between two independent variables, the variables may have an opposite association with an independent variable. In the latter, the relationship between two variables changes depending on a third variable. The SAVE-3 is significantly correlated with the PHQ-9, the GAD-7, and the PGRF (Table 4), which may indicate multicollinearity or conditional dependence.
Our findings that greater work-related stress is related to increased depression or anxiety are in close agreement with those from the literature.2930 Furthermore, depression partially mediates the relationship between work-related stress and pandemic grief reactions among the subject participants. The study above showed that depression increased both direct and indirect grief reactions.31 Similarly, another study revealed that pandemic grief is higher in the group of people with depression than those without depression.21 Besides, generalized anxiety partially mediated the association of work-related stress with pandemic grief. The finding aligns with the previous study’s result, which showed that viral anxiety directly increased pandemic grief.31 Those with generalized anxiety were found to experience more severe pandemic grief than those without generalized anxiety.21 In our study, depression and generalized anxiety seem to interfere with the normal grieving process. Given that acute grief response during the initial stages of mourning can elevate the risk of prolonged grief,8910 it is crucial to address depression and generalized anxiety, particularly among individuals facing higher levels of work-related stress.
Only one study examined the relationship between work-related stress and pathologic grief, which addressed nursing professionals. The authors showed that the frequent exposure to patients’ deaths during the COVID-19 pandemic and its aftermath increases the risk of healthcare professionals experiencing complicated grief.15 It was found that those who served both as floor nurses and in a COVID-19 intensive care unit had a higher likelihood of experiencing complicated grief, primarily due to their increased exposure to patient deaths.15 Besides, the present finding that general risk factor severity of PGRF increases pathological grief in the pandemic corresponds with the result from a previous study.16 As the general risk factor severity of PGRF partially mediated the relationship between work-related stress and pathological grief, the current finding highlights the importance of identifying those with heightened risk for pathologic grief based on the PGRF for timely intervention.
The current study has several limitations. First, although the PGRF is meant to evaluate grief risk factors from the loss of their patients during the COVID-19 pandemic, the working environment in which the study subjects worked in a tertiary hospital inevitably experienced deaths from various causes; not only COVID-19 could have affected their responses. Second, because this study was conducted two years after the beginning of the pandemic, healthcare workers could have adapted to the pandemic, which may have influenced the study’s findings. Third, because the study was performed in a single tertiary hospital in Korea, generalizations to healthcare workers in other settings should be made cautiously. This study has strengths despite its limitations; it is the first to present a measure for evaluating the severity of generic PGRF in Korean language.
We showed that the PGRF scale for healthcare workers is a psychometrically sound instrument. The scale was valid and reliable for measuring pandemic grief risk. Additionally, work-related stress intensified the pandemic grief, mediated by the general severity of PGRF, such as depression or anxiety. The PGRF can be used to identify those who are likely to develop dysfunctional grief.
 XML Download
XML Download