

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is the third most frequently diagnosed cancer and the second leading cause of cancer-related death worldwide.1 In Korea, CRC has the second highest incidence rates.2 Annual cancer statistics in Korea in 2019 reported that the age-standardized incidence of CRC ranked third among all carcinomas in both men and women, accounting for 38.4% and 22.5%, respectively. Importantly, in men aged 15–34 years, CRC incidence rate in Korea was the highest among those of all carcinomas except for thyroid cancer.3 In other words, CRC is a high-risk disease with a strong possibility of occurrence in young individuals than other carcinomas.
CRC begins as polyps in normal epithelial cells. The tumor size gradually increases and evolves into a non-advanced adenoma (< 1 cm, with tubular or tubulovillous histology), worsens to advanced adenoma (≥ 1 cm, with villous histology), and finally progresses to cancer. This transition process takes approximately 10–15 years.4 In Korea, CRC incidence rapidly increases among individuals aged > 50 years; therefore, to maximize prevention success, it is necessary to detect polyps using early screening before the 10-year period from polyp formation to cancer occurrence elapses. Early detection is important since treatment prognosis in the early stage is favorable (the 5-year survival rate of stage I CRC is 94.0%).5
For early CRC detection, colonoscopy and fecal occult blood tests (FOBT; Guaiac-FOBT and immunochemical-FOBT; also called fecal immunochemical test, FIT) are commonly used as screening methods. Colonoscopy results in accurate outcomes but is expensive and requires highly skilled endoscopists.6 FOBT, contrastingly, is a non-invasive method of collecting blood from feces,7 and its low cost reduces the examinee’s financial burden. Nevertheless, because FOBT’s sensitivity remains low, annual or biennial screening is recommended. Recently, FIT, which is based on the detection of globin antigen of human hemoglobin and its immune response, has been suggested for implementation in national screening programs because of its superior diagnostic performance.8 There are two types of FIT distinguished by the inspection method: quantitative and qualitative. Although no international standard screening method has been established, quantitative methods are more frequently used in Korea for national cancer screening due to high false positive rates of the qualitative method estimated from the conjunct dataset of cancer screening database of the National Health Insurance Service (NHIS) and the cancer registration database of the Korea Central Cancer Registry (KCCR).
In the National Cancer Screening Program (NCSP) for CRC in Korea, those aged ≥ 50 years undergo FIT annually. However, the incidence rate in patients aged 20–49 years was 12.9/100,000 population, which was the highest among the 42 surveyed countries,9 indicating that CRC is frequent even in ages that are not subject to NCSP. Early detection at a young age is more challenging because healthcare professionals do not suspect cancer even with CRC symptoms such as bloody stool, constipation, or tenesmus. Therefore, the need to adjust the age for CRC screening initiation has been highlighted. In response, a revised recommendation of the Korean guideline for CRC screening was published in 2015 to lower the initiation age of screening to 45 years.10
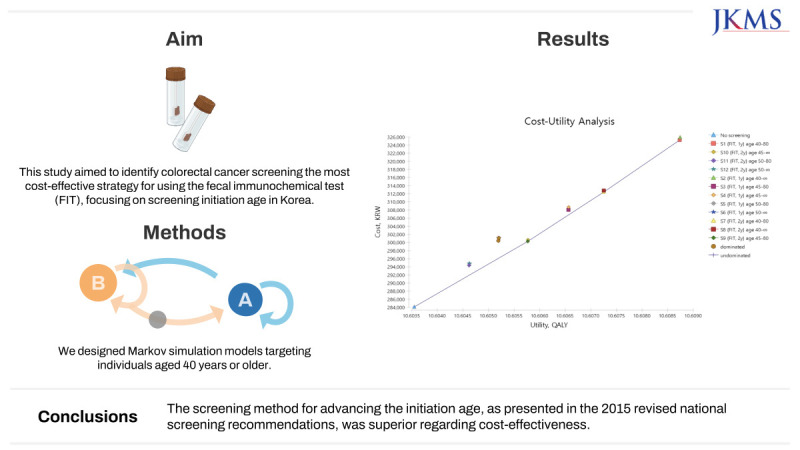
The 2015 recommendation had been established considering several domestic and foreign clinical studies, but cost-effectiveness had not been evaluated in these studies. Since NCSP is implemented for the whole nation with a limited national budget, economic aspects should be considered. In this study, we implemented cost-utility analysis to evaluate the validity of the initiating age for screening suggested by the recommendation by constructing scenarios for an initiating age of 45 ± 5 years.
We used “quality-adjusted life years (QALY)” as an outcome variable. QALY measures an individual’s quality of life over a lifetime and is frequently used as a utility indicator in cost-utility analyses of healthcare. When performing economic evaluation studies, utility can be acquired either using direct surveys or from previous studies.
Along with the basic analysis, a scenario analysis was implemented to compare the cost-effectiveness among methods of FIT being used. According to the National Health Insurance Corporation’s cancer screening database, the implementation rate of quantitative methods in the NCSP has exceeded that of qualitative methods since 2015 and has more than doubled by 2020 (qualitative, 31.78%; quantitative, 68.22%). In our scenario analysis, we aimed to clarify whether the quantitative method is superior in terms of cost-effectiveness.
In summary, this study aimed to design various strategies and determine the most cost-effective alternative screening method to determine the age of initiation and termination and screening interval, thus verifying the cost-effectiveness of the currently recommended NCSP strategy for CRC in Korea.
METHODS
Population
A hypothetical population was men and women aged ≥ 40 years, and the baseline point was 2021. If data could not be collected, the most up-to-date values were incorporated. The study assumed that only asymptomatic patients received NCSP and analyzed the cost-effectiveness of strategies by estimating the lifetime cost of screening and treating CRC, and utility.
Model construction
Herein, we constructed 12 Markov models: a combination of the ages of FIT screening initiation (40, 45, or 50 years) and termination (80 years or no limit), and the screening interval (1 or 2 years). Within this Markov model, the cohort begins at age 40 years and continues until death or 120 years, which is 81 cycles. Supplementary Fig. 1 shows a part of the model.
The model has two major assumptions. 1) Transitions from one state to another in a current cycle in Markov simulation is independent with the past cycle, and 2) after 5 years of follow-up treatment, returns to the state of high-risk general population. The second assumption is based on the conventional view in medical society that if a patient survives without recurrence after a 5-year follow-up period, the survival curve becomes almost flat, and the patient is considered cured.
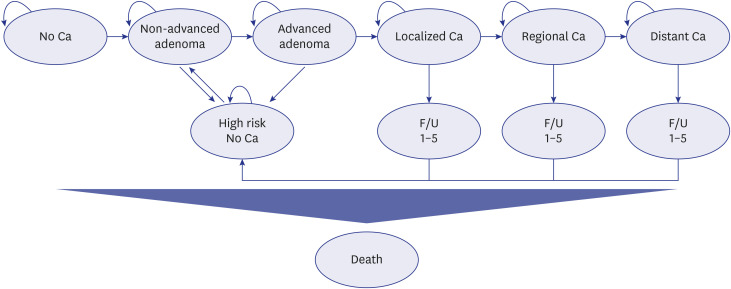
Cohorts begin either “no cancer” or “adenoma” according to the prevalence rates. They were allowed to go through the states of non-advanced adenoma and advanced adenoma sequentially, and when worsened, they could develop into local, regional, and distant cancers. All states could be transformed to death at any time (Fig. 1).
Fig. 1
Natural history of colorectal Ca. Colorectal Ca develops sequentially through non-advanced adenoma and advanced adenoma. In this model, reverse metastasis is not included, and follow-up treatment for up to 5 years is considered at the onset of Ca. For those who are cured after 5 years of treatment, patients are assigned to the no Ca but high-risk group, where non-advanced adenoma may recur. All transition states can lead to death.
Ca = cancer, F/U 1–5 = follow-up for 1–5 years.
The discount rate was 4.5%, and various range adjustments (± 1.5%) were performed in the sensitivity analysis. The healthcare system perspective was selected, which meant only direct and indirect expenses related to examinations and treatments were included in the cost indicator.
Variables
Epidemiological indicators
1) Incidence rate
The non-advanced adenoma incidence rate was referenced in the National Health Screening Statistical Yearbook (NHIS, 2021) and input into the age group of five. According to the statistics, the incidence rate was increased from 0.98% in individuals aged 50–54 years to 1.69% in those aged 75–79 years, before going down to 0.99% in those aged ≥ 85 years. The incidence rate of 40–49 years was replaced with that of 50–54 years owing to data source limitations, since CRC screening is only targeted for patients aged ≥ 50 years.
2) Transition probability
The annual transition probabilities from one status to another were used as the input. For the annual transition probability of CRC, we referred to the value reported by Ren et al.11 and Li et al.12 (from non-advanced adenoma to advanced adenoma, 2%; from advanced adenoma to local cancer: 4.4%; from local to regional cancer, 30% [25–35%]; and from regional to distant cancer, 50% [45–55%]).
3) Mortality rate
The age-specific mortality rate in the general population was calculated using the middle-year resident registration population data of the 2021 Korean Death Statistics, excluding deaths due to CRC.
Stage-specific mortality rates due to CRC were also incorporated at the 5-year age unit. Mortality rates from the first year of occurrence to the fifth year of follow-up treatment were acquired from the observation survival rate data of the cancer registration data (2002–2018). The mortality rate was the highest in the first year of occurrence, which decreased as the treatment was performed over the years.
4) Symptom rate
Once entered into the Markov cohort, patients with symptoms were immediately moved to the treatment stage without screening. Only patients with no symptoms were included in the NCSP. Therefore, we set the value of symptom rates referenced from Hassan et al.13 for local, regional, and distant cancers (12%, 27%, and 100%, respectively).
Screening indicators
1) Screening rate
The annual FIT screening rate was approximately 30% in 2021, according to data from the 2004–2021 screening rate for implementing NCSP investigated by the Cancer Screening Test Behavior Survey. Furthermore, according to data from the National Cancer Screening Information System, the CRC screening rate in a 2-year cycle from 2018–2019 was approximately 1.3 times higher than that in the 1-year cycle. Therefore, in this study, we used a 40% biennial FIT screening rate. In the case of colonoscopy, which was performed when the FIT result was positive, the age-specific screening rate was referenced from the 2019 Cancer Screening Database of the NHIS. The screening rate reached pick up to 33.37% in patients aged 65–69 years and was decreased thereafter.
2) Sensitivity and specificity
The age-specific sensitivity and specificity of FIT for CRC were measured based on the 2019 Cancer Screening Database of the NHIS and the cancer registration database of the KCCR. Sensitivity and specificity in all age groups were approximately 60% and 95%, respectively. In the case of adenomas, 15.2% sensitivity, referenced from Lew et al.,14 was input, and the specificity was the same as that of CRC. For colonoscopy as a secondary examination, both sensitivity and specificity were assumed as 95%. The screening rate, sensitivity, and specificity data could only be obtained from the national cancer screening dataset, conducted for people aged 50 years or older. Therefore, values of those aged 40–49 years were substituted with data from 50-year-old individuals.
Cost indicators
1) Screening cost
For screening cost, examination cost as direct cost, and round-trip transportation expenses as indirect cost were input. Costs were derived from “2021 National Cancer Screening Guideline” published by the Ministry of Health and Welfare. A total of KRW 17,866 was input as the FIT screening cost.
Colonoscopy cost was KRW 212,052, which included KRW 115,810 for examination, KRW 22,324 for biopsy, and KRW 68,462 for the sedation unit cost, and transportation costs. Sedation unit cost was derived from average cost surveyed by National Cancer Center among medical institutions participating NCSP in Korea. This cost was separated from the screening cost and entered into the sensitivity analysis using minimum and maximum values.
2) Treatment cost
A total of KRW 424,388 for adenoma treatment included all colonoscopy screening costs as proposed above, the cost of endoscopic polyp resection, initial and re-visit cost based on the clinical standard in 2021, and transportation costs for two visits.
We obtained data on the costs of CRC treatment by summary stage and the number of years of follow-up from the 2010–2016 NHIS database. Hospitalization, outpatient, and drug expenses were included as direct costs, and transportation and nursing expenses were included as indirect costs. For transportation and nursing expenses, the unit price was multiplied by the annual average number of outpatients, hospitalizations, and days of hospitalization. For medical expenses, the average cost was calculated by dividing the total annual medical expenses (outpatient, hospitalization, and pharmacy costs) by the number of survivors. The direct and indirect costs were added, reflecting the 2021 price index.
The treatment expenses for colonoscopic complications are as follows: according to reviews of previous studies on colonoscopy in Korea, the cost of medical disputes ranged from KRW 1.3 million17 to up to KRW 3 million.18 In this study, KRW 2.5 million was input as the treatment expense for perforation. For the treatment of bleeding, the unit price of Colonoscopic Bleeding Control specified by the Health Insurance Review and Assessment Service (2021) was calculated (KRW 131,210).
Utility indicators
In this study, the average general population utility weights of adults were calculated with an EQ-5D index using data from the 2020 National Health and Nutrition Survey, excluding those who had been diagnosed with CRC, and we input 5-year units. Consequently, the utility weights were ≥ 0.85 in all age groups and tended to decrease as the age increased. In the model, general population utility weights were applied to the adenoma and high-risk groups.
For CRC status, utility weights were obtained from Lee et al.19 and previous domestic report.20 Jo et al.20 From the year of CRC diagnosis to the fourth year of treatment, utility weights of 0.680 for local cancer and 0.592 for regional cancer were input, and the general population utility weights were applied to the fifth year for both cancers. For distant cancers, a weight of 0.445 was applied from the first year of occurrence until the fifth year after treatment.
Analysis
Base case analysis
We conducted a cost-utility analysis of various CRC screening scenarios. We diversified the starting ages to 40, 45, and 50 years, and additionally, termination age (80 years or no limit) and screening interval (one or two years) were included. A cost-utility analysis was implemented to compare the cost-effectiveness among the 12 strategies. The incremental cost-utility ratio (ICUR) values between the strategies and no screening were estimated to derive the most cost-effective strategy within the ICUR threshold. In this study, the threshold was set at KRW 50 million based on two pieces of evidence: 1) the current implicit recommendation that 2 GDP (approximately KRW 40–million) was accepted as the ICUR threshold for the treatment of severe diseases such as cancer and 2) a published study stating that the public was willing to pay an average of KRW 40,280,000 for a 1-year extension of life against severe diseases.21
Sensitivity analysis
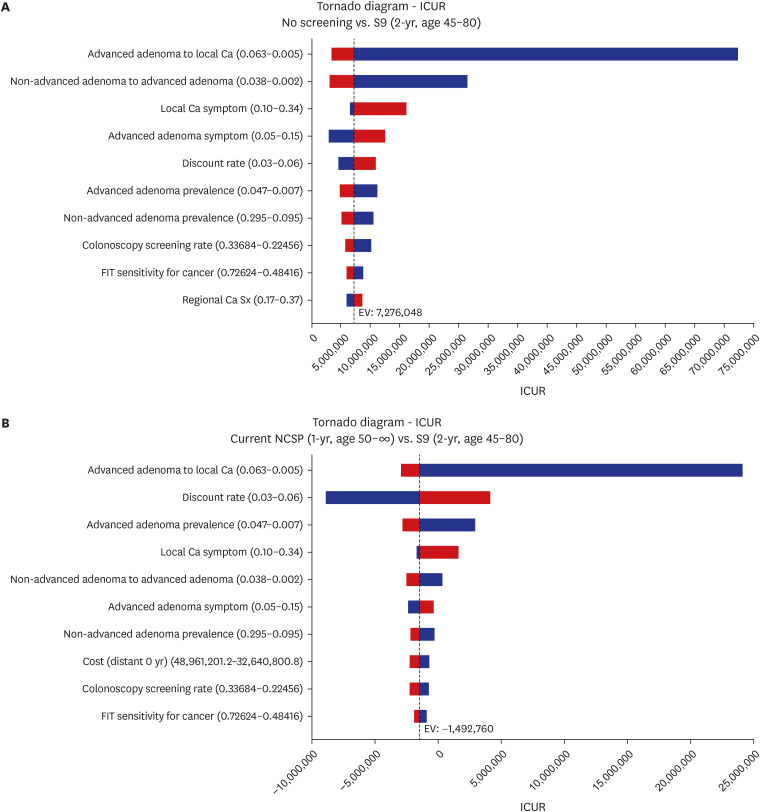
A one-way sensitivity analysis was performed and visualized using a tornado diagram to determine which variables had the greatest impact on the cost-effectiveness analysis results (Fig. 2). The discount rate ranged from 3–6%, and other variables had ranges based on standard deviations, maximum and minimum values, etc.
Fig. 2
(A) Tornado diagram of one-way sensitivity analysis (no screening vs. S9). The most sensitive variables are transition probability from advanced adenoma to local Ca and from non-advanced adenoma to advanced adenoma, and ICUR increases as both variables decrease. (B) Tornado diagram of one-way sensitivity analysis (current NCSP vs. S9). The most sensitive variables are transition probability from advanced adenoma to local Ca and discount rate. When discount rate increases, ICUR between the two strategies also increases.
ICUR = incremental cost-utility ratio, Ca = cancer, NCSP = National Cancer Screening Program.
A probabilistic sensitivity analysis was also conducted to verify the uncertainty of the model. A probabilistic sensitivity analysis was used to predict the results by assigning a distribution to each variable and randomly extracting values from each distribution for tens of thousands of simulations. In this study, we repeated the Monte Carlo simulation 100,000 times. Supplementary Table 1 shows the distributions of each variable used in the probabilistic sensitivity analysis. A 95% CI or standard deviation from the reference studies was applied for the range of distribution; however, if there was no existing evidence, we input the value that was assumed based on expert opinion.
RESULTS
Model validation
To verify the validity of the Markov model, the assumed values obtained from the model were compared with statistical indicators. Mortality rate, CRC mortality rate, and cancer detection rate were used as the indicators. In the case of mortality, the model showed an age distribution very similar to the KOrean Statistical Information Service (KOSIS) value. The lowest was 0.131% (KOSIS 0.138%) in the individuals aged 40–49 years, followed by 0.289% in those aged 50–59 (KOSIS 0.298%), 0.611% in those aged 60–69 (KOSIS 0.646%), 1.874% in those aged 70–79 (KOSIS 1.874%), and 8.579% in those aged 80 or older (KOSIS 7.847%). In the case of cancer mortality rate, in the model, 30.6 (3.4–68.1) per 100,000 died from CRC (KOSIS 30.4 [2.5–174] per 100,000), and the cancer detection rate was 0.808 (0.66–1.25) per 1,000, which was similar to the value calculated from conjunction between NHIS Cancer Screening Database and the KCCR Cancer Registration Database (0.904 [CI, 0.50–1.94] per 1,000).
ICUR
When the 12 strategies were displayed on the cost-utility graph at once, the undominated strategies were Strategy 9 (S9; 2-year cycle for 45–80 years old), Strategy 7 (S7; 2-year cycle for 40–80 years old), Strategy 1 (S1; 1-year cycle for 40–80 years old), and Strategy 2 (S2; 1-year cycle for ages of 40 years old to “no limit”). Table 1 shows the ICUR values obtained in these strategies with “no screening” as a common control group. The ICUR values for S9, S7, S1, and S2 were KRW 7,281,646, 7,646,732, 7,938,005, and 8,061,365/QALY, respectively, all of which were within the ICUR threshold (KRW 50 million).
Table 1
ICURs of undominated strategies

Tornado diagram
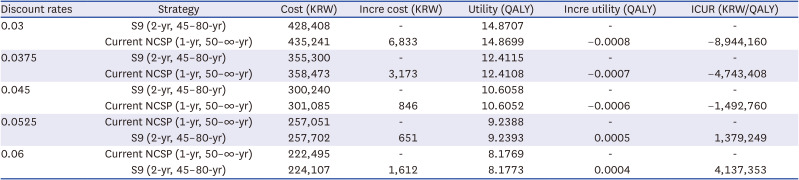
A one-way sensitivity analysis was implemented, comparing the most cost-effective strategy (S9; 2-year cycle for ages 45–80 years) with no screening and the current NCSP strategy (1-year cycle for ages 50 years to no limit), respectively. In the former, transition rates from advanced adenoma to local cancer and from non-advanced adenoma to advanced adenoma were variables that affected the results the most (Fig. 2A). When comparing S9 with the current NCSP, the transition rate from advanced adenoma to local cancer and discount rate were the most sensitive variables (Fig. 2B). Specifically, when the discount rate was < 4.5%, the current NCSP strategy (1-year, 50-no limit years old) was estimated to cost higher and the utility was lower, so S9 was the overwhelmingly dominant strategy (ICUR negative value), but as the discount rate exceeded 4.5%, the cost of the S9 strategy became more expensive than the current strategy. As discount rate increased, the ICUR value was converted to a positive number, and continued to increase (ICUR KRW 1,379,249/QALY at a discount rate of 5.25%; KRW 4,137,353/QALY at a discount rate of 6%) (Table 2).
Table 2
One-way sensitivity result depending on discount rates (current NCSP vs. S9)
Overall, except for the discount rate, indicators that could not be artificially adjusted, such as transition probabilities, were sensitive variables, meanwhile screening costs did not significantly affect the results.
Probabilistic sensitivity analysis
We verified that the uncertainty of the cost-effectiveness in the four strategies was significantly low, indicating that the probability that each of the four strategies were cost-effective was very high compared to that of “no screening.”
Scenario analysis
Sensitivity and specificity of qualitative & quantitative methods of FIT
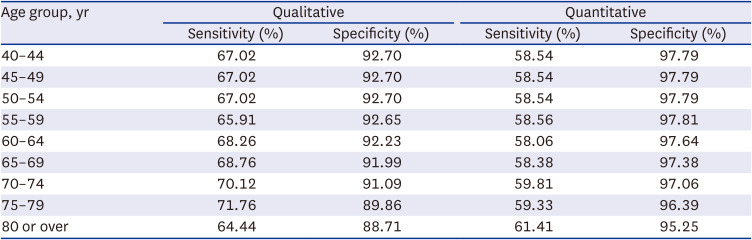
Table 3 shows the age-specific sensitivity and specificity of each qualitative and quantitative FIT method utilized in the scenario analysis. They were derived from the conjunction between the NHIS Cancer Screening Database and the KCCR Cancer Registration Database. The specificity of the qualitative method was approximately 5–7% lower, confirming that its false positive rate was higher than that of the quantitative analysis. In other words, the qualitative method identified more healthy individuals as positive, leading to unnecessary additional tests and treatments.
Table 3
Age-specific sensitivity and specificity of qualitative and quantitative fecal immunochemical test in 2018
Cost-utility analysis results
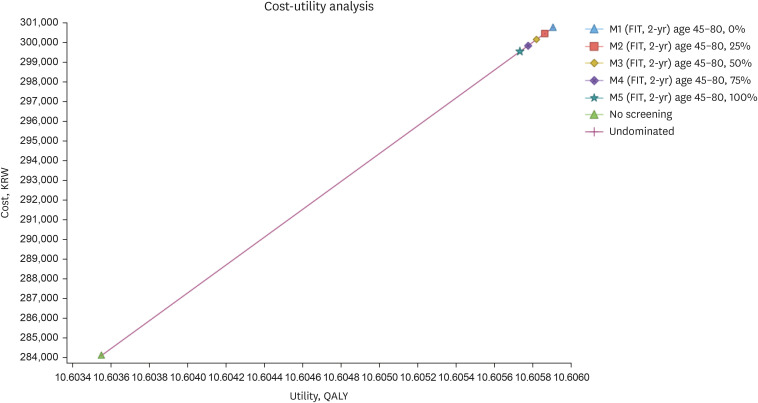
Fig. 3 shows the results of the cost-utility analysis for five scenarios (M1–M5) with different relative screening ratio between quantitative and qualitative methods for the S9 strategy. The strategy using a quantitative method as 100% (M5) costed the least (KRW 299,532), but the cost-effectiveness among five strategies did not differ significantly (ICUR KRW 7,066,382/QALY for M1; KRW 7,065,900/QALY for M2; KRW 7,066,026/QALY for M3; KRW 7,066,797/QALY for M4; 7,068,254/QALY for M5).
Fig. 3
Cost-utility graph according to relative screening rates of quantitative FIT. This is an ICUR graph between scenarios with various relative screening ratios of quantitative and qualitative method of FIT. M1 is the model when the relative screening rate of the quantitative method is 0% (qualitative 100%). According to the cost-utility analysis, ICURs among all five strategies and no screening are very similar, meaning there is no significant difference in terms of cost-effectiveness.
FIT = fecal immunochemical test, ICUR = incremental cost-utility ratio, QALY = quality-adjusted life years.
DISCUSSION
In this study, we analyzed which age and cycle combination screening strategy was the most economic for CRC screening. Many studies have shown that screening decreases mortality and reduces the prevalence of CRC; however, the relative utility, cost, and cost-effectiveness of various strategies have not been sufficiently verified. This should be analyzed by country because the situation in each country varies widely.
In domestic studies, cost-effectiveness analyses were performed by comparing FIT with colonoscopy.2223 FIT is recommended in the 2015 Korean guideline for CRC screening10 based on the “high” evidence level suggesting that FIT reduces CRC mortality and increases early detection rate. Nonetheless, studies on FIT are required to determine the optimal strategy, specifically cost-effectiveness in different screening ages and cycle terms.
In Korea, the NCSP for CRC is provided to adults aged > 50 years, but the 2015 recommendation suggested to lower the initiating age for screening to 45 years and set the upper limit to 80 years. Although this was determined based on various overseas clinical practice guidelines, randomized comparative clinical trial studies, and domestic age-specific CRC incidence,410 the economic aspects were not considered. Since the NCSP is a project provided for the whole nation, it needs to derive a highly acceptable strategy for both providers and recipients; therefore, cost-effectiveness evidence should be evaluated. The results of this study are nationally meaningful and may provide supportive scientific evidence for establishing NCSPs in other Asian countries.
Consequently, lowering the initiation age to 45 years and limiting the termination age to 80 years were superior in terms of cost-effectiveness. Moreover, strategies that set the starting age at 40 years were also cost-effective, whereas none with the initiation age of 50 years were selected. Setting 50 years as the initiating age reduced the total cost, but the overall utility was inferior compared to strategies with starting ages of 40 or 45 years. Likewise, according to additional analysis including strategies that further varied the termination age (70, 75, 80 years old, and no limit), no strategy with an initiating age of 50 years was selected as cost-effective. Meanwhile, setting the termination age at 70 or 75 years were found to be more cost-effective, but the termination age of 80 years was also cost-effective (KRW 7,931,055/QALY) within ICUR threshold. This is shown in Supplementary Table 2. The Korean guideline of CRC screening states that it is appropriate to undergo screening from the age of 45–80 years, and it can be concluded that the cost-effectiveness results of this study are supporting this claim.
Regarding the screening interval, 1 and 2 years were acceptable in the recommendations based on the Minnesota study242526 and the oversea clinical practice guidelines. Moreover, in the cost-utility analysis, both screening intervals could be considered in the NCSP since the ICURs were both within the threshold, although 1 year was slightly more cost-effective than 2 years.
According to one-way sensitivity analysis, FIT screening cost did not have a significant effect because the price was too small (KRW 17,866). In Korea, the unit price of FIT is only 1/20 of that of colonoscopy (FIT KRW 12,410, colonoscopy KRW 115,810), and the FIT screening cost used in this study was relatively low compared to German and US economic evaluation studies, which had values of 15.9 Euro and 17.70 dollars, respectively (KRW 23,076 and KRW 23,688, respectively).1627
According to the scenario analysis, there was no significant difference in cost-effectiveness between quantitative and qualitative. High false positive rates of the qualitative method have been reported in many studies; for example, Park et al.28 reported that the rate of positive diagnoses among all examinees was higher with the qualitative method (8.11% vs. 2.51%), whereas the actual cancer detection rate was higher with the quantitative method (5.2% vs. 14.4%). In a Chinese study, the quantitative method had significantly higher positive predictive values for large adenomas (≥ 1 cm) and CRC than the qualitative method (P = 0.013, 0.034), rendering it more dominant in CRC screening.29 We expected that qualitative method may result in higher healthcare expenditure due to unnecessary additional screening and treatment done for actually healthy recipients; however, the difference in the cost estimated through the Markov simulation was minor.
As a strategy for CRC national cancer screening, we showed that it was most economical to conduct the FIT every 2 years for individuals aged 45–80 years. This study is significant because it provides cost-effectiveness evidence for the screening strategy presented in the 2015 NCSP recommendations. However, to produce the expected effect from the best strategy based on clinical and economic evidence, the public should be encouraged to comply with screening according to the recommended cycle. Currently, an annual screening rate for FIT in the NCSP is approximately 30–40%. Making consistent efforts to increase the screening rate is the most important precondition for implementing a more effective NCSP strategy.
The strengths of this study are as follows: first, we utilized a Markov simulation model to track long-term cost-effectiveness until death. To predict the cost-effectiveness of chronic diseases that require long-term follow-up, such as cancer, a Markov simulation is suitable because it can predict the complex progression of chronic diseases in a simple and effective manner.30 Second, age- or stage-specific data were used when inputting mortality, sensitivity, specificity of screening, and medical costs into the model. Finally, while there are no previous domestic or foreign studies on the economic evaluation of quantitative and qualitative methods, this study also confirms the cost-effectiveness according to the relative screening ratios of quantitative and qualitative methods.
This study has some limitations. First, a sex comparison analysis was not performed in each screening strategy. This was because the study focused on determining the most cost-effective age for screening initiation. However, in the follow-up study, the analysis should be supplemented to consider men and women separately because sex may affect the cost-effectiveness result. Second, there were limitations in data collection. For example, the baseline period of the study was 2021, but not all variables were available for 2021 data; therefore, some outdated sources were used. Furthermore, in case of utility, the data sources used were different between general population and CRC patients, the possibility of variation due to the use of multiple data remained a limitation. We made an effort to resolve uncertainty problem due to limited sources, by applying distributions for each variable in the basic analysis and performing additional sensitivity analysis. Finally, simulations employed the probability of the entire group without considering individual-level socioeconomic status, family history, and social support as variables. In a follow-up study, a more sophisticated cost-effectiveness analysis should be conducted through microsimulations using individual patient data.
In conclusion, for national CRC screening, lowering the initiating age of FIT screening to 45 years, limiting the upper age to 80 years, and implementing it every 2 years is the most cost-effective strategy. Moreover, the cost-effective strategies with low uncertainty levels included 1- and 2-year cycle for individuals aged 40–80 years old and 1-year cycle for those aged between 40 years until death. Meanwhile, there was no difference in cost-effectiveness between quantitative and qualitative methods. This study confirmed that screening strategies more effective in the clinical world are also superior in terms of cost-effectiveness. Therefore, the results of this study can be used to support the economic basis for revising the NCSP as a guideline published in 2015.
 XML Download
XML Download