

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
A rapid aging population, characterized by a significant increase in the proportion of older adults in a country or population, is a global challenge faced by many countries, including Korea.1 Korea is on track to become a super-aged society by 2025, with the proportion of people aged 65 years reaching 20% of the total population.2 With the aging of society and the increase in life expectancy, the impact of these conditions on the health and well-being of older individuals has significant implications for both individuals and the healthcare system. Hypertension is a major cause of premature death and functional decline worldwide, being one of the most prevalent chronic diseases among older people. It is a well-known major risk factor for cardiovascular diseases such as heart disease, stroke, and kidney disease, affecting a substantial portion of the global population, particularly older adults.34 In 2020, 29.4% of the adult population suffered from hypertension, and 5.0 million (40% of total hypertension patients) aged 65 years or older had hypertension in Korea. Due to population aging, the number of people with hypertension aged 65 or older is increasing rapidly compared to those aged 20–64.5
Frailty could be defined as a reduction in functional capacity, an increased vulnerability to adverse health outcomes, and a diminished ability to cope with stressors.67 It is a multidimensional syndrome encompassing factors such as muscle weakness, fatigue, slowed movement, weight loss, and low physical activity.6 Frailty is associated with an elevated risk of falls, hospitalization, disability, and mortality.8 Previous studies have identified the potential benefits of intensive treatment for hypertension in reducing the incidence of cardiovascular events and mortality, even in the older population.910 However, the optimal target blood pressure (BP) for older hypertensive patients varies from under 130 to 140 mmHg according to guidelines.111213 The HOW to Optimize eLDerly systolic BP (HOWOLD-BP) trial, comparing the incidence of cardiovascular events in older Korean patients with hypertension based on two target systolic blood pressure (SBP) levels (≤ 130 and ≤ 140 mmHg) is currently ongoing.
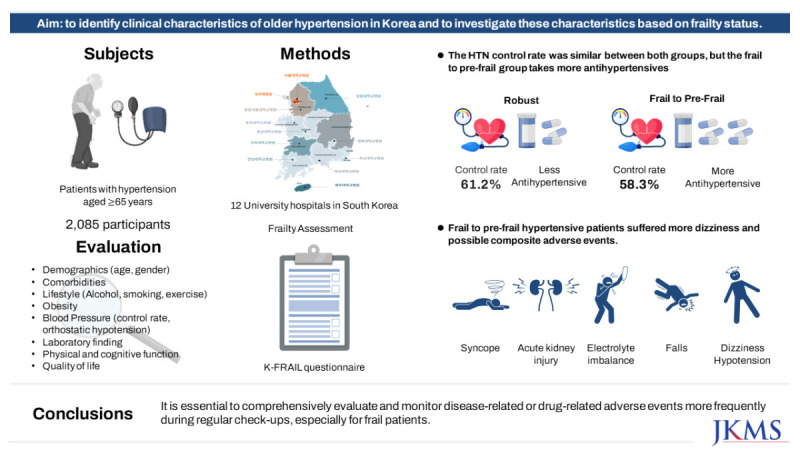
This study aimed to evaluate baseline characteristics of older hypertensive patients and patterns of antihypertensive medications in participants enrolled in the HOWOLD-BP study up to December 31, 2022. We will also identify clinical differences and antihypertensive medication use patterns according to frailty status.
METHODS
The HOWOLD-BP trial is designed as a prospective, multicenter, open-label randomized clinical trial planned to follow-up each participant for three years. The HOWOLD-BP trial aims to compare intensive SBP-lowering treatment (target SBP ≤ 130 mmHg) with standard treatment (target SBP ≤ 140 mmHg) to reduce cardiovascular events in older hypertensive Korean patients over 65 years. The subjects have been recruited from 11 university hospitals in Korea since January 15, 2019.
The inclusion criteria were 1) patients aged ≥ 65 years, 2) patients diagnosed with hypertension who were already taking antihypertensive medications or treatment-naïve patients with a clinic SBP of 140 to 180 mmHg, 3) patients with independent activity of daily living (ADL) and 4) patients who provided written informed consent. Participants were excluded if they met any of the following criteria: 1) a past medical history of secondary hypertension, 2) resistant hypertension, 3) orthostatic hypotension with symptoms during screening, 4) a recent experience of acute coronary syndrome, cardiac surgery, or urgent percutaneous coronary intervention within the recent 3 months, 5) heart failure with left ventricular ejection fraction < 40%, 6) hypertrophic obstructive cardiomyopathy, aortic stenosis, moderate to severe valve disease, or congenital heart disease, 7) diagnosis of acute cerebral infarction within the last 3 months, 8) uncontrolled diabetes mellitus at screening (HbA1c ≥ 10%), 9) end-stage renal disease (on hemodialysis or estimated glomerular filtration rate [eGFR] less than 15 mL/min/1.73 m2), 10) diagnosis of moderate to severe retinopathy (retinal hemorrhage, visual impairment, microaneurysm) within the last 6 months, 11) clinically significant liver disease or an aspartate transaminase/alanine transferase level greater than 3 times the upper normal range, 12) uncontrolled thyroid dysfunction, 13) enrollment in other clinical trials within the last 4 months or plans to participant other clinical trials during our study, and 14) other reasons that may limit participation or the progress of the study, as determined by the investigators.
We utilized data collected during the screening assessment to identify baseline clinical characteristics. Physical measurements included clinic BP, heart rate, weight, height, and orthostatic hypotension. Blood tests and urine analyses were also performed. Family history, medical history, sociodemographic history, smoking history, and alcohol-drinking history were assessed. ADLs were evaluated using the modified Barthel index (range, 0 to 100; lower numbers indicate worse activity and daily living function).14 Instrumental ADLs (IADLs) were measured using the Lawton and Brody index (range, 0–5 for males; 0–8 for females; lower numbers indicate worse IADL function).15 Frailty was assessed using the Korean version of the fatigue, resistance, ambulation, illnesses, and weight loss (K-FRAIL) questionnaire, with a score of 1–2, ≥ three defined as having pre-frail and frailty, respectively.16 Gait speed was measured based on the time it took to transverse a 4-m course, including 1 m for acceleration and deceleration. The handgrip strength was measured twice in both arms using a TKK-5401 GRIPD (Takei, Niigata, Japan), and maximum handgrip strength was used for analysis. Cognitive function was assessed using the Korean version of the Montreal Cognitive Assessment (MoCA-K; range, 0 to 30, with lower numbers indicating worse function).17 Health-related quality of life was evaluated using the Korean version of the EQ-5D.18 Detailed descriptions for assessment and primary and secondary outcomes were presented in the protocol paper.19 BP and heart rate were measured at the heart level in the seated position using a professional digital BP monitor (HEM7080-IC, Omron Healthcare, Lake Forest, IL, USA). BP was measured in a quiet room after 5 minutes of rest and was repeated three times after another 2 minutes of rest under the supervision of the research coordinator. The mean systolic and diastolic blood pressure (DBP) from the second and third measurements were used. Control of hypertension was defined as meeting both systolic BP of less than 140 mmHg and DBP of less than 90 mmHg. Orthostatic hypotension was defined as a decrease in systolic BP of at least 20 mmHg or a reduction in DBP of at least 10 mmHg within 3 minutes of standing.
Continuous variables were expressed as the mean ± standard deviation (SD), while percentages and numbers were used for categorical data. The baseline characteristics of the robust and pre-frail to frail groups were compared using the Student’s t-test for continuous data and Pearson’s χ2 test for categorical data. All statistical analyses used a significance level of 0.05 and were performed using the PASW Statistics software (SPSS version 25.0; IBM Corp., Armonk, NY, USA). The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statement
The study protocol has been approved by the ethics committee of each participating center, including the Seoul National University Bundang Hospital (approval No. B-1811-504-006). Informed consent was submitted by all subjects when they were enrolled. This study was registered with the Clinical Research Information Service (Internet) in 2019 (KCT0003787, available from: https://cris.nih.go.kr/).
RESULTS
Patients were enrolled in the HOWOLD-BP study from January 15, 2019, to December 31, 2022. A total of 2,093 patients were registered, but one patient dropped out before the eligibility assessment, two patients dropped out after randomization, and five patients dropped out due to screening failure. Finally, 2,085 patients were analyzed, including 1,044 patients in the intensive treatment group and 1,041 patients in the standard treatment group (Fig. 1). The mean age of participants was 73.2 years (SD, 5.60), and 48.0% (n = 1,001) were male. Over half were obese (53.6%, n = 1,118), and 20.75% were overweight. Mean BP was 136.5 (± 15.23)/74.7 (± 9.71) mmHg, and mean pulse pressure was 69.3 (± 12.87) per minute. About 60.4% (n = 1,260) of patients had well controlled BP. More than two-thirds (66.5%, n = 1,387) had dyslipidemia, and about one-third (28.9%, n = 603) had diabetes with comorbidity. Among the participants, 63.0% (n = 1,314), 49.8% (n = 1,039), and 19.7% (n = 410) had experience of admission, surgery, and coronary revascularization, respectively. Only a small proportion of patients were current smokers (6.5%, n = 136), consumed drinking alcohol more than twice per week (14.0%, n = 290). More than half of the participants exercised regularly (52.5%, n = 1,095), while 12.0% (n = 251) maintained an active lifestyle without exercise, and 21.9% (n = 456) did not exercise at all. About 4.9% (n = 103) reported at least one episode of syncope, acute kidney injury, electrolyte imbalance, falls, and hypotension. Dizziness was also self-reported among 1.6% (n = 33), and orthostatic hypotension was measured among 1.2% (n = 24). Most participants were independent in IADL (97.0%, n = 2,023). Regarding physical performance, 27.7% (n = 577) of patients had a slow gait speed (≤ 0.8 m/sec), and 29.2% (n = 609) had low grip strength (men: ≤ 28 kg; women: ≤ 18 kg). Participants had a mean MoCA-K score was 24.4 (± 4.59), and 25.0% (n = 521) participants were categorized for cognitive impairment (MoCa-K score < 23) (Table 1).
Fig. 1
Flow chart of inclusion of study participants.
n = number of patients, HOWOLD-BP = HOW to Optimize eLDerly systolic BP.
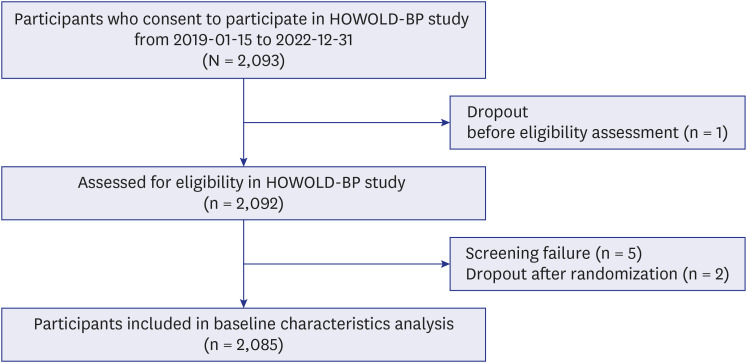
Table 1
Baseline characteristics of 2,085 participants recruited from the HOWOLD-BP study
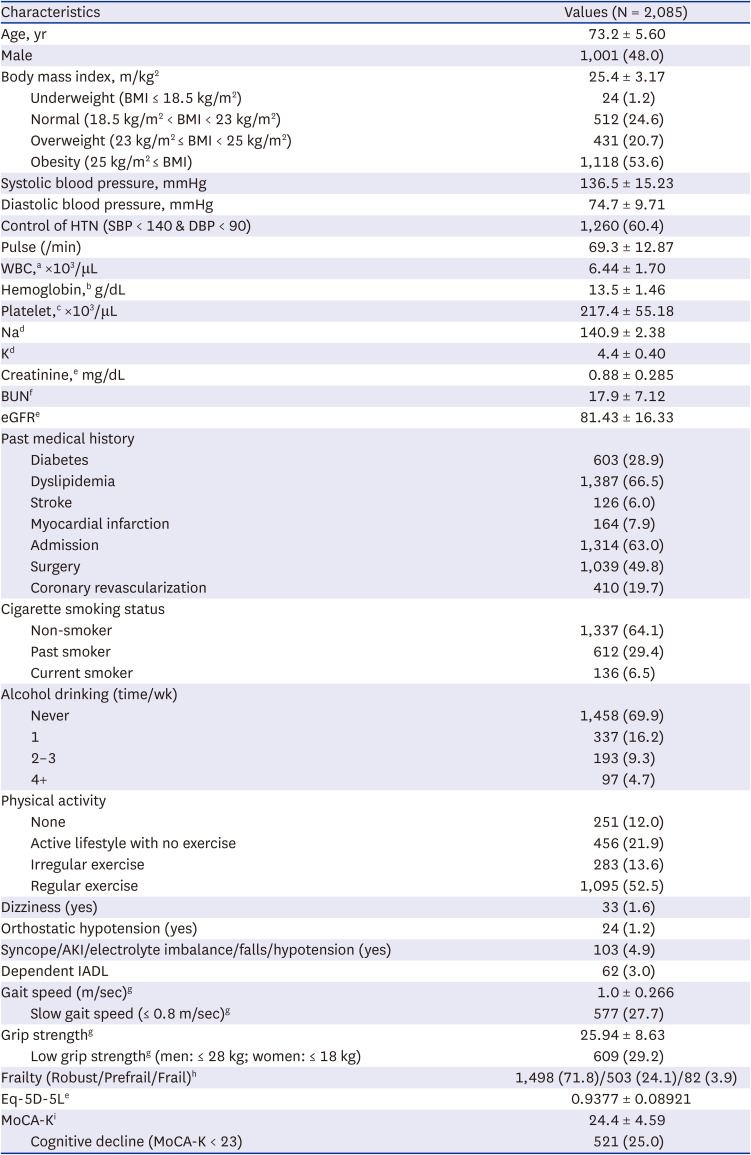
Values are presented as number (%) or mean ± standard deviation.
HOWOLD-BP = HOW to Optimize eLDerly systolic BP, BMI = body mass index, HTN = hypertension, SBP = systolic blood pressure, DBP = diastolic blood pressure, WBC = white blood cell, BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate, AKI = acute kidney injury, IADL = instrumental activities of daily living.
a11 patients were missing, b9 patients were missing, c12 patients were missing, d22 patients were missing, e3 patients were missing, f4 patients were missing, g7 patients were missing, h2 patients were missing, i10 patients were missing.
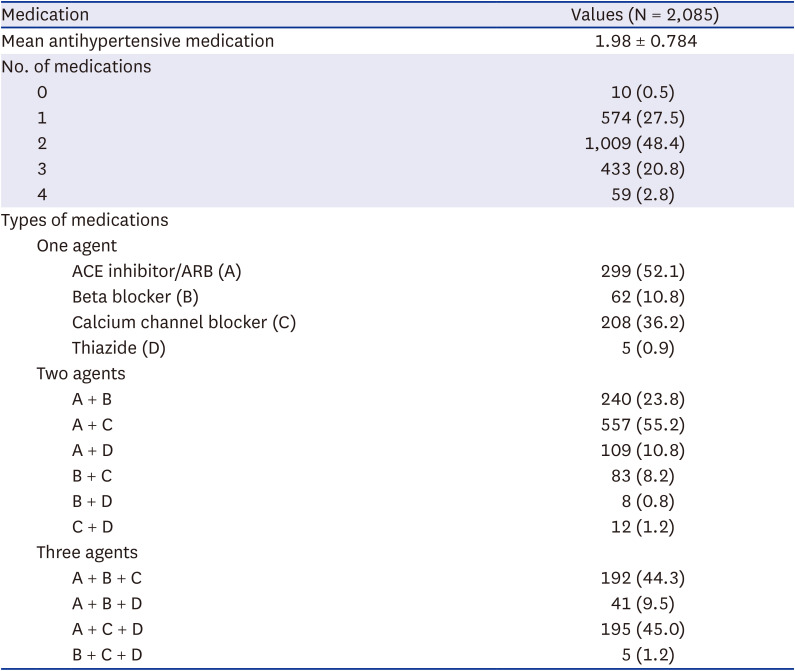
The majority of older Korean hypertensive patients received two antihypertensive drugs (48.4%, n = 1,009), while 27.5% (n = 574) and 20.8% (n = 433) received 1 and 3 antihypertensive medications, respectively. Among hypertensive patients taking only one drug, 52.1% (n = 299), 36.2% (n = 208), 10.8% (n = 62) and 0.9% (n = 5) were prescribed an angiotensin receptor blocker (ARB)/angiotensin-converting-enzyme inhibitor (A), calcium channel blocker (CCB) (C), beta-blocker (B) and thiazide-like diuretics (D), respectively. The most frequently prescribed two-drug combination was A + C (55.2%, n = 557), followed by A + B (23.8%, n = 240) and A + D (10.8%, n = 109). Among patients taking three medications, A + C + D combination (45.0%, n = 195) and A + B + C (44.3%, n = 192) were the most frequent combinations (Table 2).
Table 2
The medication history of 2,085 participants recruited from the HOWOLD-BP study
The control rate of hypertension was similar in robust (61.2%, n = 917) vs. prefrail to frail (58.3%, n = 341) patients (P = 0.220). Frail hypertensive patients tended to be older, have lower hemoglobin, lower serum sodium, higher serum potassium, lower eGFR, and a lower percentage of males. In terms of comorbidity, frail patients are more likely to have diabetes, a history of stroke, and admission. Regarding lifestyle, frail patients were less likely to have a history of past or current smoking and less likely to exercise regularly. Interestingly, robust patients were less likely to report dizziness, but the actual rate of orthostatic hypotension was similar to frail to pre-frail patients. The composite incidence of syncope, acute kidney injury, electrolyte imbalance, falls, and hypotension was higher than the pre-frail to frail group than the robust group (5.7% vs. 3.65%, P < 0.001). Pre-frail to frail patients tended to have dependent IADL, slower gait speed, lower grip strength, lower quality of life score, and cognitive function (Table 3).
Table 3
Baseline characteristics according to frailty status from the HOWOLD-BP study
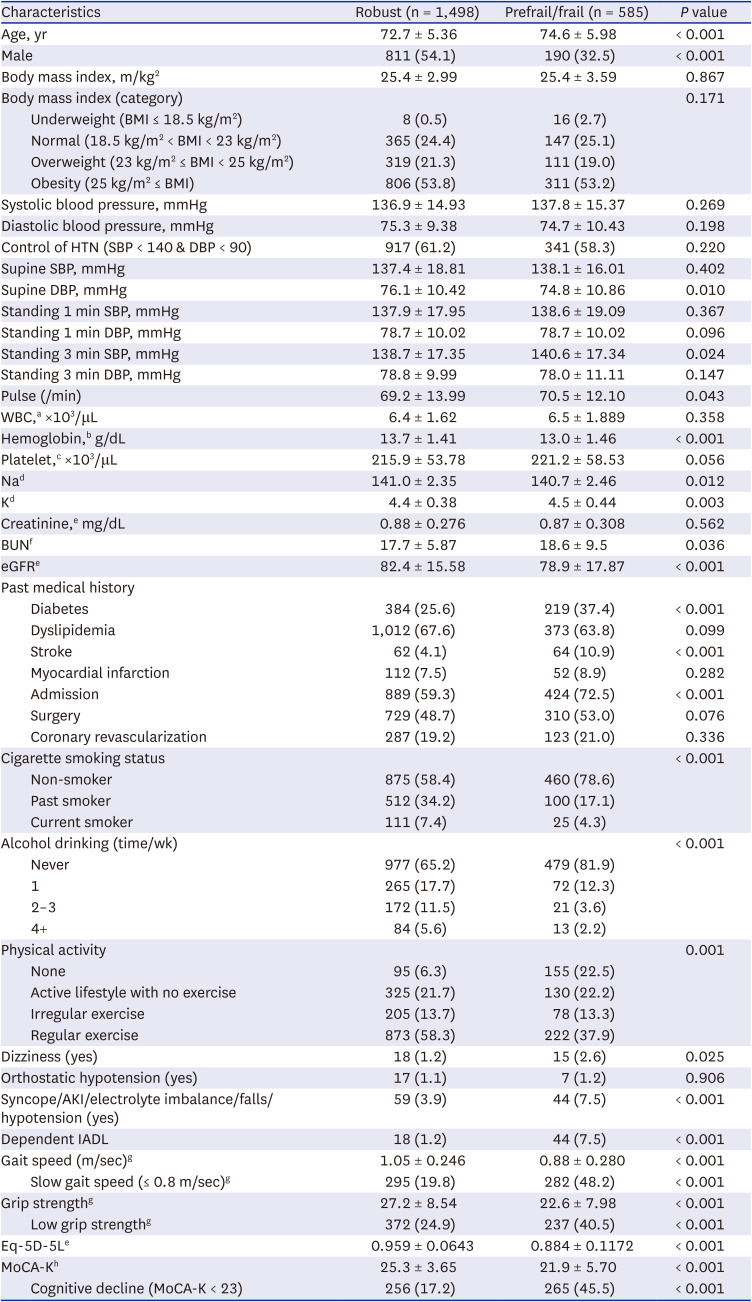
Values are presented as number (%) or mean ± standard deviation.
HOWOLD-BP = HOW to Optimize eLDerly systolic BP, BMI = body mass index, HTN = hypertension, SBP = systolic blood pressure, DBP = diastolic blood pressure, WBC = white blood cell, BUN = blood urea nitrogen, eGFR = estimated glomerular filtration rate, AKI = acute kidney injury, IADL = instrumental activities of daily living.
a11 patients were missing, b9 patients were missing, c12 patients were missing, d22 patients were missing, e3 patients were missing, f4 patients were missing, g7 patients were missing, h10 patients were missing.
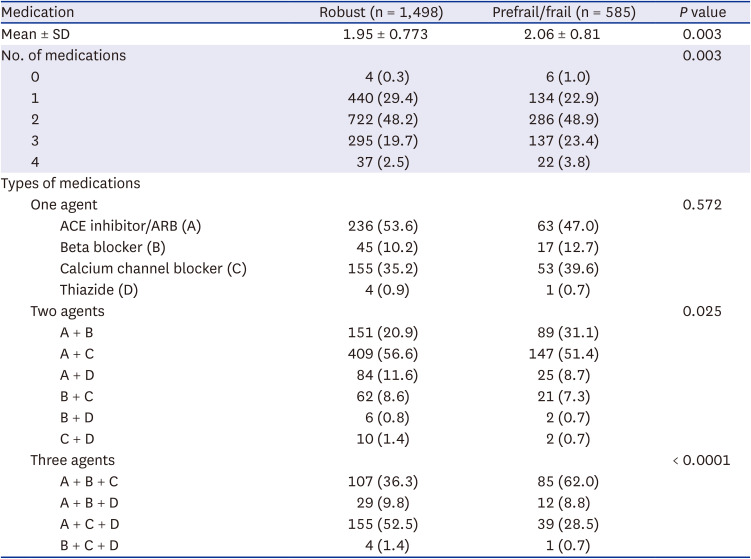
Frail to pre-frail older hypertensive patients used more antihypertensive medications than robust older hypertensive patients (1.95 vs. 2.06, P = 0.003). Most pre-frail to frail patients used two medications (48.9%) or three medications (23.4%) to control hypertension, whereas robust patients used two medications (48.2%) or one medication (29.4%). For three-drug combinations, frail to pre-frail patients preferred beta blockers, while robust patients preferred diuretics after ACE inhibitor/ARB and CCB combination (Table 4).
Table 4
The hypertension medication history according to frailty status from the HOWOLD-BP study
DISCUSSION
The results of the HOWOLD-BP study offer a comprehensive insight into the clinical characteristics of older hypertensive patients in Korea, focusing on demographic, laboratory, clinical, lifestyle, frailty, functional (physical, cognitive) aspects, as well as adverse events related to antihypertensive medication. In this study, 60.4% (n = 1,260) of participants had controlled blood pressure, which means systolic BP of less than 140 mmHg and diastolic BP of less than 90 mmHg. Although the participants of this study did not represent the general older population because they were recruited at national university hospitals and visited for hypertension, the control rate of this study was relatively higher than the general adult population according to the 2023 fact sheet released by the Korean Society of Hypertension, which reported a 47.4% control rate among hypertensive patients in Korea.5 However, older hypertensive patients often contend with other chronic diseases, including dyslipidemia (66.5%), diabetes (28.9%), a history of coronary revascularization (19.7%), myocardial infarction (7.9%), and stroke (6.0%).
Prevalence of obesity (body mass index ≥ 25 kg/m2) in the HOWOLD-BP study was 53.6%, which aligns closely with the results of the study conducted in China (54.2% among 65–74 and 47.4% among patients aged ≥ 75 years).20 Unhealthy lifestyles choices, such as smoking and heavy drinking, were relatively rare (current smoker: 6.5%, alcohol consumption more than twice per week: 14.0%). Nevertheless, only about half of the patients engaged in regular physical activity (52.5%). Given that lifestyle modifications, particularly weight loss for obese patients, are well-tolerated and effective in reducing cardiovascular risk, it is crucial to emphasize lifestyle changes, including weight management and exercise, for older patients with hypertension in Korea.2122
The study reveals a significant association between frailty status and factors, such as older age, female gender, higher pulse pressure, lower hemoglobin, and a higher prevalence of comorbidities like diabetes and stroke, and a history of hospitalization. Predictively, older pre-frail to frail hypertensive patients displayed a higher likelihood of dependence on IADL, weaker grip strength, slower walking speed, lower quality of life, and diminished cognitive function compared to the robust population. The composite event (syncope, acute kidney injury, electrolyte imbalance, falls, hypotension), which is considered a possible adverse event during hypertension treatment in frail elderly, indeed occurred more in the pre-frail to frail group (7.5%) compared to the robust group (3.9%, P < 0.001). Therefore, it is essential to comprehensively evaluate older hypertensive patients and to monitor disease-related or drug-related adverse events more frequently during regular check-ups for pre-frail to frail older patients with hypertension. The result of the gender difference in frailty status among older hypertensive patients is consistent with previous research on the general population that females had higher frailty status than males at all ages, and male mortality rates exceeded female mortality rates.23 The findings from this study have contributed to a better understanding of the implication of frailty on hypertension management in older adults.
While the study offers several valuable insights, it has some inevitable limitations. First, the study’s cross-sectional nature limits the ability to infer causality between frailty and clinical characteristics. For example, pre-frail to frail older patients engaged in regular physical exercise less frequently, but there were fewer cases of being a current smoker or drinking more than twice a week. It is difficult to determine whether the lifestyle pattern is a cause or a result of frailty. Second, beta-blockers were chosen as the preferred third medication over diuretics for the pre-frail to frail patients, but it is unclear whether this is due to the comorbidity pattern or whether frailty status influences the choice of medication and the number of medications. Even though heart failure with decreased ejection fraction was excluded, the prevalence of atrial fibrillation was more frequent in the prefrail to frail group than in the robust group (8.2% [n = 68] vs. 4.6% [n = 47], P = 0.001, missing 9.5% [n = 215]) according to the initially collected electrocardiogram. Future research should employ longitudinal designs to explore the causal relationships and the long-term impacts of different treatment approaches to explore causal relationships and the long-term impacts of different treatment approaches on frail, older hypertensive patients. Additionally, further studies should investigate the underlying mechanisms linking frailty, hypertension, and adverse health outcomes, which could inform the development of targeted interventions to effectively manage hypertension in older adults with varying frailty statuses.
In conclusion, the HOWOLD-BP study verifies the characteristics of older hypertensive patients in Korea and identifies the intricate relationship between frailty and clinical characteristics among older hypertensive patients. These findings underscore the importance of considering frailty status in managing hypertension in older adults, advocating for personalized treatment approaches and lifestyle modifications. When determining the optimal BP target (< 130 mmHg vs. < 140 mmHg of SBP), which is the research goal of the HOWOLD-BP study, considering frailty is essential. Future research aimed at unraveling the complexities of hypertension management in the aging population will be needed, ultimately contributing to improved management and monitoring strategies, clinical outcomes, and quality of life for older hypertensive patients.
 XML Download
XML Download