

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
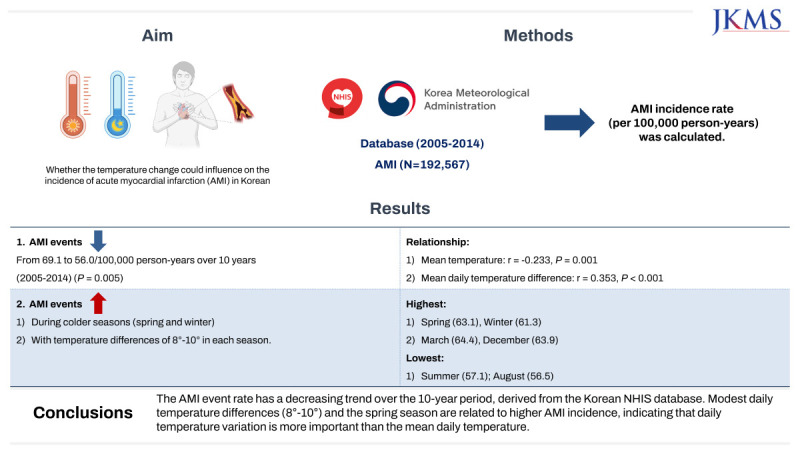
In the contemporary era, a growing body of epidemiological and clinical evidence has led to heightened concern regarding the potential short- and long-term deleterious effects of climate change on cardiovascular health.1 Acute myocardial infarction (AMI) is a major cause of disability and death worldwide, and can be triggered by meteorological and environmental factors, such as air temperature and microparticles.234 Weather conditions have been shown to influence daily mortality and disease burden, especially in relation to the cardiovascular system. Factors such as the extreme temperature, diurnal temperature range, temperature variation, and humidity have been considered as risk factors that may contribute to cardiovascular disease (CVD) mortality. In recent review of the literature showed that extreme (high or low) temperatures are associated with a higher risk of cardiovascular events.5
Assessing AMI events recorded in the National Registry of Myocardial Infarction, Spencer et al.,6 suggested a seasonal pattern exists in the occurrence of AMI, characterized by a high risk of AMI cases in winter and a lower risk in summer months. In the East Asian (Japanese) AIM Registry, Rumana et al.,7 reported that seasonal variations in case occurrence and AMI case fatalities peaked in winter and spring. However, additional findings from research on ambient temperature and cardiovascular events have been inconsistent.89101112 Here, we investigated the impact of temperature on the incidence of AMI in the Korean population using the National Health Insurance Service (NHIS) database and weather information from the Korea Meteorological Administration.
METHODS
Study setting and population
This observational and ecological study sought to investigate the impact of air temperature on the incidence of AMI over a 10-year period from January 2005 to December 2014. The study population included residents in the Republic of Korea, with a permanent resident population of around 50 million.
Data collection
Monthly AMI data were extracted from the Korean NHIS database according to the International Classification of Disease 10th edition (ICD-10) A total of 192,567 AMI cases were extracted without district-specific data available. In this study, new-onset acute myocardial infarction was defined as follows: First, patients must have no ICD-10 code for acute myocardial infarction or have not undergone percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) in 2004. Next, these patients are those who were hospitalized with an ICD-10 code or underwent PCI or CABG since 2005. Daily temperature (°C) data was systematically collected from the Korea Meteorological Administration Research database. Over a 10-year period, we assessed the data over 3 phases, including early (from 2005 to 2007), middle (from 2008 to 2010), and late (from 2011 to 2014) phase. Seasonal categories were as follows: spring (March, April, May), summer (June, July, August), fall (September, October, November), and winter (December, January, February).
Statistical analysis
We used an indirect standardization method for the age-gender standardized incidence of AMI. The age-sex standardized incidence method was as follows: After dividing by gender, age standardization was performed. Age standardization adjusted for differences between groups of various ages to make them comparable. For standardization purposes, a specific reference age is usually chosen and data from other age groups are adjusted to this reference. Descriptive statistical methods were used to describe the characteristics of the variables. Monthly incidence of AMI and mean temperature were examined graphically using time-series plots. Statistical analyses were performed using IBM SPSS version 22 (IBM Corp., Armonk, NY, USA). Pearson’s correlation coefficient was performed to assess the relationship between temperature and AMI. A two-tailed P value of < 0.05 was the criteria for statistical significance. Statistical graphing was performed using Excel software.
RESULTS
Study population, annual AMI rate distribution and temperature
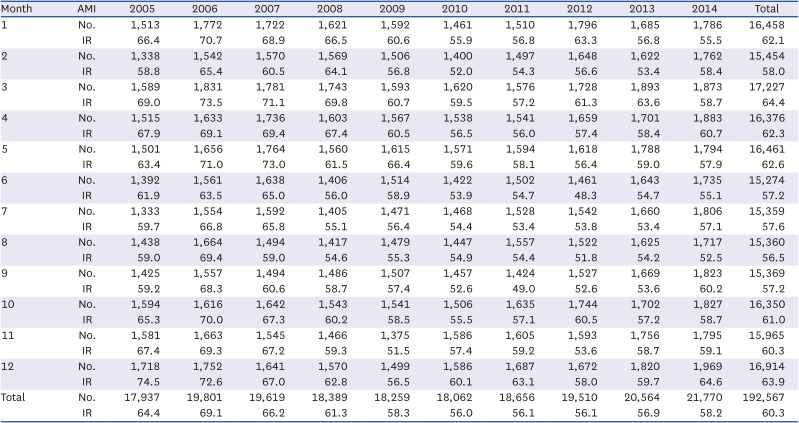
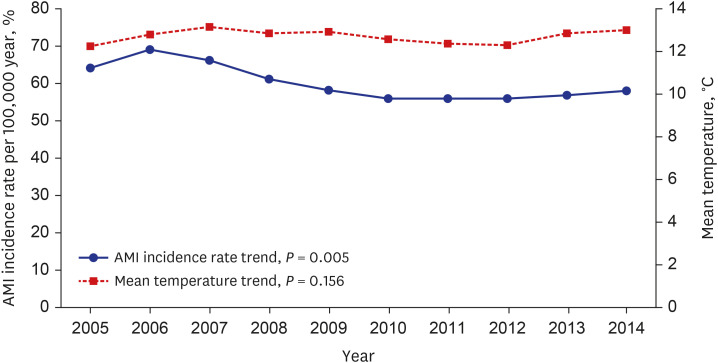
A total of 192,567 AMI cases (mean age: 64 years) were recorded in the Korean NHIS database. They were predominantly male (67.4, n =129,846, mean age: 61 ± 13 years), with males generally younger than female (difference in mean age of 11 years). Classifying according to age range, the majority of the population was middle-aged and older adults (40–59 years, > 60 years) for males, whereas older adults (> 60 years) were more likely to be female (Table 1). The distribution in monthly and annual incidence of AMI from 2005 to 2014 (Table 2) showed, that the mean AMI incidence rate per 100,000 year was 63.3. Over the 10-year period, there was a decreasing tendency (69.1 down to 56.1, P for trend 0.005) in prevalence of AMI from 2005 to 2014 (Fig. 1).
Table 1
The demographics in Korean patients with AMI
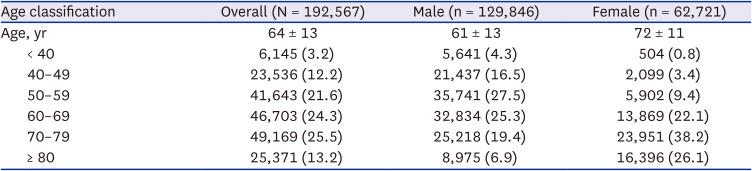
Table 2
The distribution in monthly incidence of AMI from 2005 to 2014 in Korean
Effects of mean temperature monthly AMI incidence
The distribution of monthly incidence of AMI according to temperature change is shown in the Supplementary Fig. 1. Overall, with the mean temperature decreasing from September, the incidence of AMI was getting increasing. In contrast, with the weather getting warmer in summer (June, July and August) the AMI incidence is decreasing. The highest monthly incidence of AMI was March, followed by December (Supplementary Fig. 1).
Effect of mean daily temperature change, seasonal variation and incidence of AMI
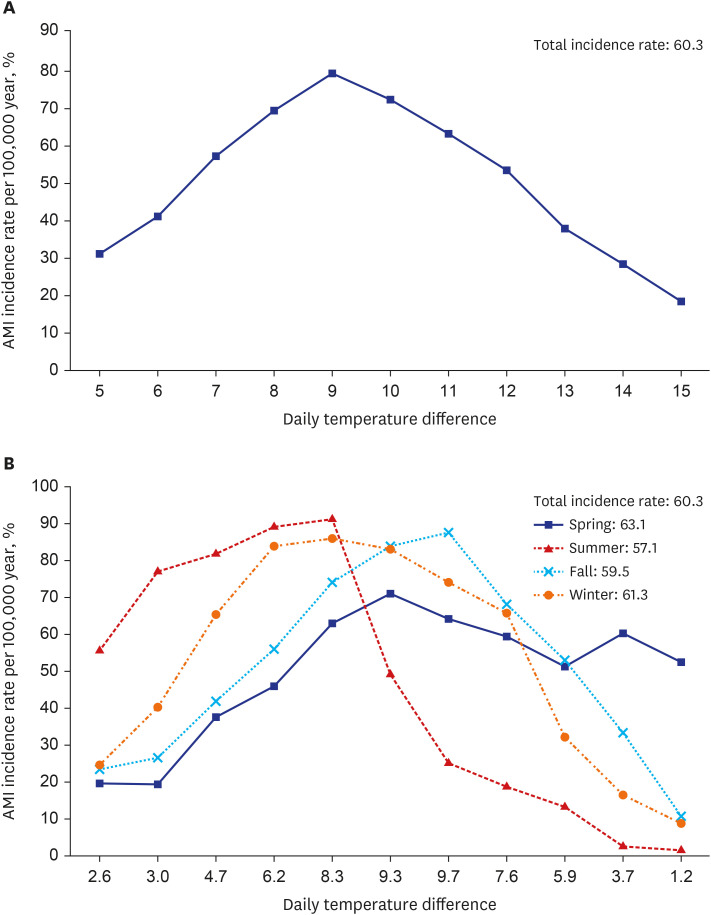
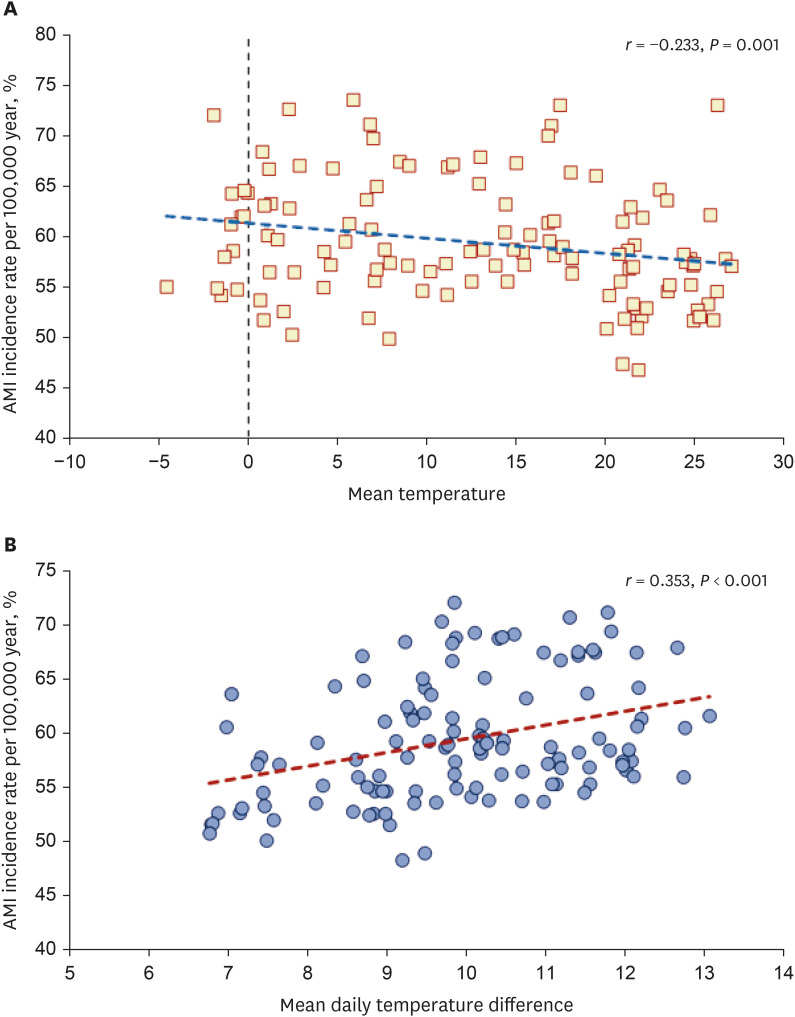
The distribution of AMI events according to daily temperature change is shown in Fig. 2. There was a moderate negative linear relationship between mean temperature and monthly AMI occurrence (r = −0.233, P = 0.001) (Fig. 3A). The highest incidence of AMI occurred at a temperature difference of 8–10° (Fig. 2A), with a moderate positive linear relationship (r = 0.353, P < 0.001) (Fig. 3B). In the distribution of seasonal AMI events, the incidence rate per 100,000 year was higher during the colder seasons (63.1 in spring, and 61.3 in winter), followed 59.5 in the fall and 57.1 in summer (Fig. 2B).
DISCUSSION
According to the NHIS-derived AMI Registry from 2005 to 2014 in the Republic of Korea, we report that temperature change (cold) has an adverse impact on the occurrence of AMI. Daily temperature differences share a liner correlation with increasing AMI events, with the same being evident for increasing daily temperature differences. The triggers for AMI have been examined in several studies, and among the factors associated with the onset of AMI, intense exercise or physical exertion, diet, coffee and alcohol consumption, smoking, sexual activity, cocaine or marijuana abuse, emotional stress and environmental conditions have been reported.13 Environmental conditions most often refer to temperature, air pollution and influenza epidemics.14 Here, we focused on temperature change and AMI events in the context of global warming, with an increase in mean temperatures of about 0.8°C occurring over the last 20 years in the Republic of Korea.
Cold weather can cause rises in catecholamine levels and subsequent vasoconstriction, increasing heart rate and blood pressure, which may precipitate myocardial ischemia and coronary plaque instability.2 We observed that the incidence of AMI was relatively lower in summer (June, July, and August), and the event rate increased as temperatures declined from September to April and when daily temperature differences were greater, such as during spring, with a slight decrease in incidence during the extreme cold season with smaller daily temperature differences (January and February). We also identified a moderate negative relationship between mean temperature and monthly occurrence of AMI. Consistent with previous findings, temperature decreases were associated with higher frequency of AMI occurrence.1516 This finding was consistent with warmer areas of tropical or subtropical regions such as Taiwan and Singapore.1718
In a previous study of the Korean AMI Registry from 1997–2006, Hong and Kang19 investigated the relationship between seasonal variation and AMI mortality in Korean patients using the Korean National Health Insurance Claims Database. The results showed a winter peak and summer nadir. In the general trend, there was a decrease in occurrence of annual AMI events from the early (0.066%) to middle (0.058%) phase, being lowest in the late (0.057%) phase, which may be hypothetically explained by global warming-related declines in acute cardiovascular events. During unseasonably cold days, the majority of the population a places a priority on keeping warm and reduces out-door physical activity. This may reduce the overall levels of physical exertion, causing a subsequent reduction in AMI occurrence, which may explain, in part, the findings for the coldest months (January and February). As well as global warming, less smoking, warmer housing conditions and less outside work with regard to the economic growth of Korea may have reduced AMI events during the winter season. Interestingly, modest temperature changes (8–10 degrees) correlate with the highest AMI incidence. This difference was a slightly lower than previously reported mean temperature differences of 10.3 to 12.7 degrees, which might be related to temperature zone differences.2 With such modest temperature differences, people participating in more outdoor activities or exercise might have an increased risk of AMI.2021 Therefore, not only cold temperature, but also transitions and variability of temperature may be more important to trigger AMI.222324
We note several limitations to our study. Firstly, important information for the analyzed population regarding AMI incidence including risk factors and medications was not included. Secondly, data was limited in relation to meteorological conditions such as air pressure,25 cloudy and rainy days with high humidity, and long sunshine duration,26 which have also been associated with cardiovascular events. In the fall and winter periods, a higher incidence of hospital admissions has been noted due to cardiopulmonary diseases related to atmospheric stagnation.27 Thirdly, cold weather also contributes to ambient air pollution. Chen et al.,28 reported that even short-term, transient (i.e., Several hours) exposure to air pollution can trigger the onset of AMI. Data for typical air pollutants including PM2.5, nitrogen dioxide, and sulfur dioxide were not extracted from the National Institute of Environmental Research database. Finally, there may be a potential bias from extracting our data or ICD-10 code from the NHIS database.
In conclusion, from the Korean NHIS database, the AMI event rate has a decreasing trend over the 10-year period. Modest daily temperature differences (8–10°) and the spring season correlate with higher AMI incidence, indicating daily temperature variation is more important than the mean daily temperature.
 XML Download
XML Download