

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
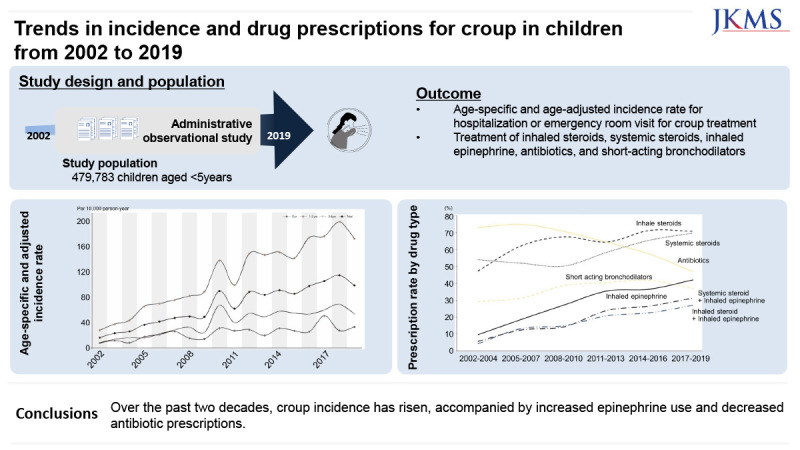
Croup is the most common cause of acute upper airway obstruction in young children, typically occurring between 7 and 36 months of age. It is characterized by symptoms such as inspiratory stridor, a barking cough, and hoarseness.12 Although mild in most cases, croup places a significant burden on the health care system, with an annual peak incidence of nearly 5% during the second year of life.345 Advanced diagnostic tests have identified the main causative viruses of croup as parainfluenza, and rhinovirus, followed by enterovirus, respiratory syncytial virus (RSV), influenza, and human bocavirus.2 The epidemic period of croup varies according to region and climate. In the Northern Hemisphere, such as in the United States and Canada, croup hospitalizations rapidly increase in autumn and early winter in odd-numbered years.4678 In a prospective study in Finland, croup hospitalizations were mainly prevalent in late spring or autumn, and in studies in Korea, there was no significant seasonal variation.910
The management of croup primarily focuses on keeping the upper airway open, as its constriction can result in respiratory challenges.1 Treatment strategies have evolved in recent decades.2 Consequently, the use of corticosteroids has become a fundamental element in addressing croup.11 Notably, recognition of the importance of inhaled epinephrine therapy for moderate to severe croup cases has been growing.12
Despite croup being a significant and burdensome respiratory disease in young children, it has not been comprehensively examined using nationally representative data over an extended period in recent years. Monitoring the national trends in the prevalence and treatment of croup can provide important insights into childhood health management. Therefore, we used a national sample cohort to characterize cases of croup requiring hospitalization or emergency room (ER) visits, analyze trends over time, and describe management.
METHODS
Study design, population, and data source
The National Health Insurance Service-National Sample Cohort (NHIS-NSC) included approximately one million subjects. They were randomly selected, constituting 2% of the Korean population who had been eligible for their health insurance qualifications for at least 1 year as of 2006, based on factors such as sex, age, region, and insurance premium.13 All of the residents in South Korea were compulsorily subscribed to the universal national health insurance provided by the Korean NHIS.1415 This national sample cohort study included socio-demographic profiles (age, sex, residence area, insurance premium decile, and types of health insurance), medical care service utilization (diagnostic codes, hospitalizations/out-clinics/procedures or prescriptions, medical costs, and medical institutions), and mortality data. All children aged 0–4 years were included in the analysis. We tracked them using the NHIS-NSC database from January 1, 2002, to December 31, 2019.
Definition of hospitalization or ER visit for croup treatment
The primary event of interest was hospitalization or an ER visit for croup treatment. All records of hospitalizations or ER visits with a principal diagnosis of croup (International Classification of Diseases, 10th Revision [ICD-10], code J05.0) were identified. The total number of children under the age of 5 years who had been hospitalized or visited the ER with a principal diagnosis of croup was 4,608, and the total number of hospitalizations or visits to the ER with a principal diagnosis of croup was 5,569 during the study period (2002–2019).
Prescription for croup
Medications prescribed during hospitalization or ER visits with the principal diagnosis of croup were individually identified. Based on the guidelines for the treatment of croup, systemic steroids, inhaled steroids, and epinephrine were included. Furthermore, we evaluated the use of short-acting β-2 agonists and systemic antibiotics.
Systemic steroid administration was defined as oral, intramuscular, or intravenous administration. All types of antibiotics were administered orally, intramuscularly, or intravascularly. The combination of medications prescribed for one hospitalization or ER visit for croup treatment was identified, and the number of events using only the corresponding combination of the five drugs was analyzed. Monotherapy refers to the use of a single type of drug, whereas polytherapy refers to the use of a combination of two, three, or four of the specified 5 drugs.
Procedures for croup treatment
We identified the utilization of chest radiography, supplementary oxygen therapy, and nebulizer treatment for croup through treatment codes.
Covariates
The residential areas were divided based on geographic proximity: 1) Seoul, Incheon, and Gyeonggi-do; 2) Gyeongsang-do; 3) Jeolla-do and Jeju; and 4) Chungcheong-do and Gangwon-do. Economic status was determined based on the insurance co-payment amounts, with “low” defined as less than the lowest 30%, “middle” as ≥ 30% and < 80%, and “high” as ≥ 80%. The seasons are divided into spring from March to May, summer from June to August, fall from September to November, and winter from December to February. Medical institutions are segmented into three levels based on institutional size and variety of available departments: 1) tertiary hospitals; 2) secondary or general hospitals; and 3) primary hospitals or clinics.
The assessed comorbidities included a history of asthma exacerbation, atopic dermatitis, or hospitalization for pneumonia treatment. Asthma exacerbation was defined as hospitalization with a principal diagnosis of asthma (ICD-10 code J45.X or J46.X). Atopic dermatitis was defined as having at least one outpatient visit with a principal diagnosis of atopic dermatitis (ICD-10 code L20.X) and receiving two or more prescriptions of topical corticosteroids. The hospitalization history for the treatment of pneumonia was based on the principal diagnosis of pneumonia (ICD-10 codes J12.X to J18.X).
Statistical methods
The study identified the number of children who experienced hospitalization or ER visits for croup treatment and tracked these events from 2002–2019. To analyze trends according to specific age ranges, we categorized the subjects into three age groups: 0, 1–2, and 3–4 years. The age-specific incidence rate per 10,000 persons-years was calculated at each year during the study period, and the age-adjusted standardization with the direct method was used to compare the incidence rates of hospitalization or ER visits for croup treatment.16 The age-adjusted standardized incidence rates per 10,000 persons-year of hospitalization or ER visit for croup treatment from 2003 to 2019 were calculated as the sum of the expected events of interest based on the population distribution in 2002. In addition, to confirm the seasonal variability, the incidence rates per 10,000 person-months of hospitalization or ER visits for croup treatment and the size of the population in each year were defined as the midterm population of the size of the population on July 1. Statistical tests for linear trends across prevalence cycles stratified by sex, residence area, economic status, comorbidity, types of medical institutions, and procedure were performed using orthogonal polynomial contrasts, and probability values of < 0.05 were considered statistically significant. We calculated estimated prevalence ratios and their 95% confidence intervals (CIs) for the use of inhaled epinephrine, inhaled steroids, the use of three or more types of medication, and hospital stays exceeding the median number of days. These calculations were performed using binomial logistic regression. The analysis was adjusted for sex, age, residence area, economic status, comorbidities (asthma exacerbation, atopic dermatitis, or hospitalization for pneumonia treatment), and types of visiting hospitals. We showed the distribution of the number of prescription drugs and the prescription rate by drug type. Significance was set at P < 0.05. All the statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
This research was conducted with ethical clearance under the current National Health Insurance Act. This retrospective study was performed in accordance with the relevant guidelines and regulations. The study protocol was reviewed and approved by the Institutional Review Board of the Korea National Institute for Bioethics Policy (P01-201603-21-005).
Patient consents were not required as this study was based on de-identified and publicly available data. The need for informed consent was waived the Institutional Review Board of the Korea National Institute for Bioethics Policy.
RESULTS
Age-adjusted standardized incidence rate
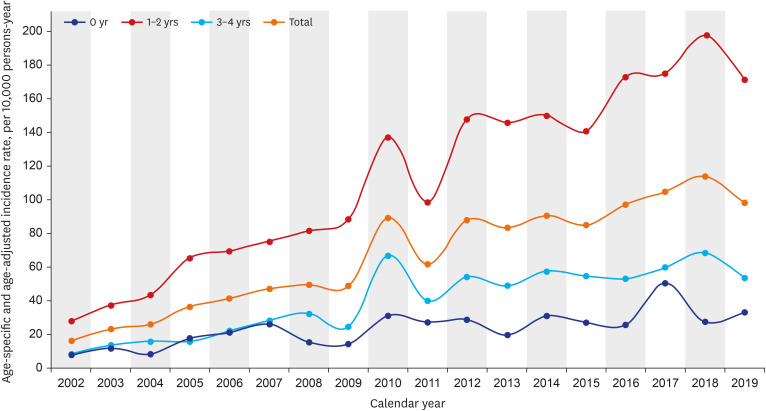
The age-adjusted standardized incidence rate and age-specific incidence rate of hospitalizations or ER visits for croup treatment in children aged < 5 years from 2002 to 2019 are shown in Fig. 1. The age-adjusted incidence rate was applied to consider the different population distributions from 2002 to 2019, which tended to increase during the study period. The age-adjusted incidence per 10,000 person-year was 16.1, 22.90, 25.84, 36.29, 41.29, 47.07, 49.44, 48.81, 89.50, 61.75, 88.18, 83.46, 90.70, 85.12, 97.40, 105.12, 114.22, 98.29 each year from 2002 to 2019, respectively. The age-specific incidence rates were highest in children aged ≥ 1 year and < 2 years among all periods and lowest in children aged under 1 year except 2005.
Hospitalization or ER visits for croup treatment
Table 1 shows the trends in hospitalizations or ER visits for croup treatment in children under 5 years of age from 2002 to 2019 with 3-year increments. The prevalence of children who were hospitalized or who visited the ER for croup treatment showed an increasing trend over the study period, with a prevalence of 0.36% from 2002 to 2004 and 1.48% from 2017 to 2019 (P value for trend < 0.001). The utilization of medical institutions for hospitalization or ER visits related to croup treatment showed a notable trend: a decrease in secondary and tertiary hospitals, coupled with an increase in primary hospitals or clinics (All P values for trend were < 0.001).
Table 1
Prevalence of hospitalizations or ER visits for croup treatment in children under 5 years of age by demographic and clinical characteristics, 2002 to 2019
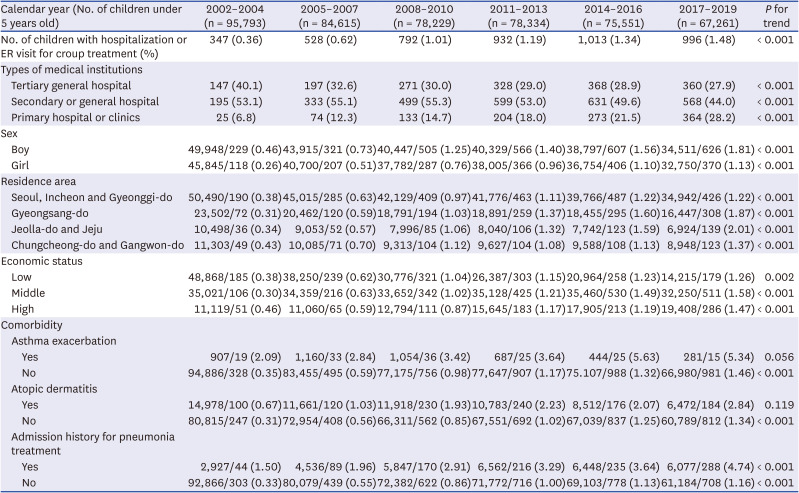
During the entire study period, the prevalence of hospitalization or ER visits for croup treatment was higher in boys than in girls. Regardless of sex, residential area, and economic status, the prevalence of hospitalization or ER visits for croup treatment tended to increase during the study period (P values for trend were < 0.001). Moreover, children who had comorbidities such as asthma exacerbation, atopic dermatitis, or a history of admission for pneumonia treatment showed a higher prevalence than those who did not. Furthermore, the prevalence of croup increased statistically significantly from 2002 to 2019 in children without comorbidities, while it remained relatively stable in those with comorbidities.
Seasonal variability of hospitalization or ER visits for croup treatment
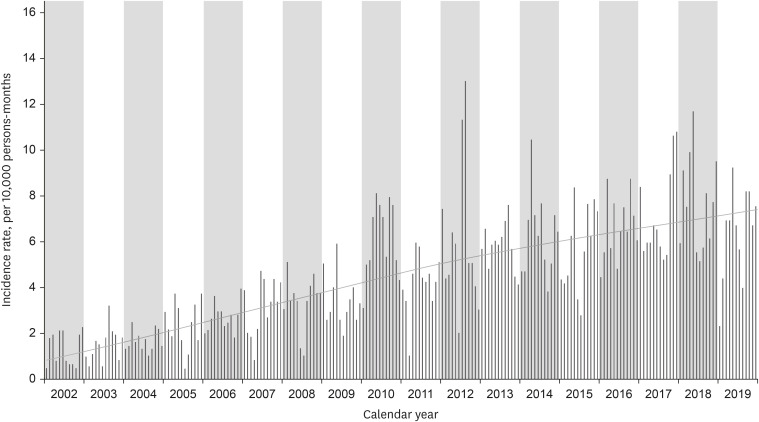
Fig. 2 shows the monthly incidence of hospitalization or ER visits for croup treatment in children under 5 years of age from 2002 to 2019. Although seasonal fluctuations were observed, the incidence rate gradually increased from 2002 to 2019. During the study period, the season with the highest incidence of croup each year in this study was spring, followed by winter. In August 2012, the incidence rate of hospitalizations or ER visits for croup treatment in children under 5 years of age was 12.93 per 10,000, which was the highest.
Prescription drugs at hospitalization or ER visits for croup treatment
Fig. 3 and Supplementary Table 1 show drug prescriptions during hospitalization or ER visits for croup treatment. From 2002 to 2004, polytherapy was administered to approximately two-thirds of patients requiring hospitalization or ER visits for croup treatment. Over time, the proportion of patients treated with polytherapy increased.
Fig. 3
Medication prescriptions per hospitalization or emergency room visit for croup treatment, 2002 to 2019. (A) Distribution by number of prescription drugs. (B) Prescription rate by drug type.
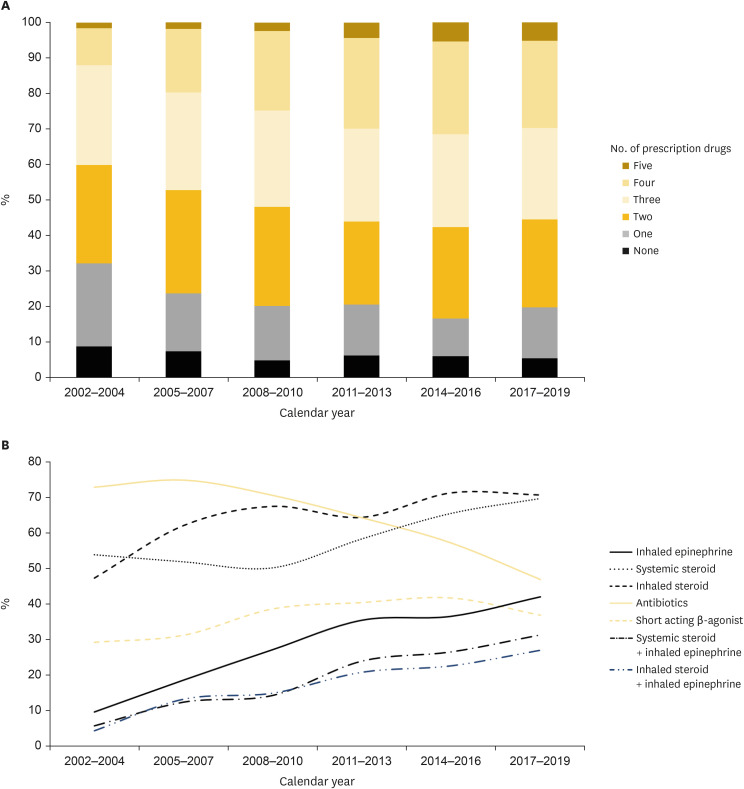
In addition, during the study period, there was a decline in the prescription of antibiotics from 73% to 47%, whereas there was an increase in the prescription of inhaled steroids (from 47% to 71%), systemic steroids (from 54% to 70%), and inhaled epinephrine (from 10% to 42%). Furthermore, from 2002 to 2019, a significant upward trend was observed in prescriptions for polytherapy, which included systemic steroids and inhaled epinephrine (increasing from 6% to 31%), as well as inhaled steroids and inhaled epinephrine (increasing from 4% to 27%).
Procedures at hospitalization or ER visits for croup treatment
The procedures performed during hospitalization or ER visits for croup treatment also changed during the study period (Table 2). Supplemental oxygen supply was decreased (21.3% to 3.4%, P for trend = 0.03), and nebulizer treatment was increased (59.7% to 69.3%, P for trend < 0.001). In addition, chest radiography was still performed in more than half of the events but showed a decreasing trend over the study period (87.2% to 76.1%, P for trend < 0.001). Cases exhibiting high severity symptoms, such as requiring intubation (mechanical ventilation), intensive care unit (ICU) admission, or the use of High-Flow Nasal Cannula (HFNC), were relatively few. Only two cases of intubation occurred (one between 2014–2016 and another between 2017–2019), and a total of nine cases were admitted to the ICU (two between 2002–2004, four between 2005–2007, one between 2008–2010, one between 2014–2016, and one between 2017–2019). Additionally, six cases required the use of HFNC (one between 2014–2016 and five between 2017–2019). As a result, a total of 15 cases with high severity symptoms were identified during the study period, which is approximately 0.27% of all croup cases in this study. Therefore, the rarity of high-severity cases among all croup cases examined.
Table 2
Treatments or procedures during hospitalization or emergency room visit for croup treatment, 2002 to 2019

Factors affecting drug prescriptions and length of hospital stay at hospitalization or ER visits for croup treatment
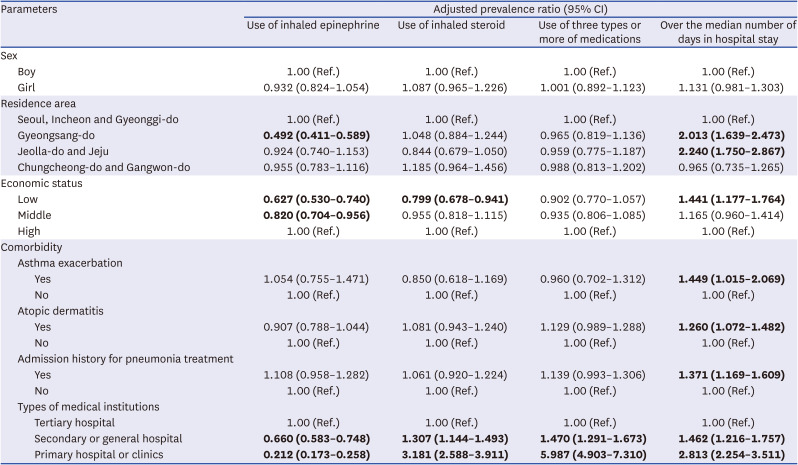
All prescriptions or procedures during hospitalization or ER visits for croup treatment from 2002 to 2019 were compared according to sex, residential area, economic status, presence of comorbidities, and types of medical institutions (Table 3). There were no sex-based differences in the use of epinephrine (adjusted prevalence ratio [95% CI], 0.93 [0.82–1.05]), inhaled corticosteroids (1.09 [0.97–1.23]), the use of three or more types of medications (1.00 [0.89–1.12]), or the length of hospital stays exceeding the median duration (1.13 [0.98–1.30]). Low economic status was associated with reduced use of epinephrine and inhaled corticosteroid (0.63 [0.53–0.74] and 0.80 [0.68–0.94]), as well as longer hospitalization stays (1.44 [1.18–1.76]) when compared to high economic status. Children with comorbidities (asthma exacerbation, atopic dermatitis, or admission history for pneumonia treatment) were more likely to require longer hospital stays exceeding the median duration than those without comorbidities. Compared to the tertiary general hospital, secondary or primary hospital prescribed lower amounts of inhaled epinephrine (0.66 [0.58–0.75] and 0.21 [0.17–0.26]), higher amounts of inhaled steroid (1.31 [1.14–1.49] and 3.18 [2.59–3.91]) and multiple drugs of three or more types (1.47 [1.29–1.67] and 5.99 [4.90–7.31]), and tended to have longer hospital stays exceeding the median duration (1.46 [1.22–1.76] and 2.81 [2.25–3.51]).
Table 3
Multivariable-adjusted prevalence ratios of hospitalizations or emergency room visits for croup treatment in children under 5 years of age, 2002 to 2019
DISCUSSION
In the present study, we characterized the demographic and clinical factors in a nationwide sample cohort of children under 5 years old who were hospitalized or visited the ER for croup treatment in Korea from 2002 to 2019. Our results showed that the incidence of hospitalization or ER visits for croup treatment showed an upward trend. Specifically, hospitalizations and ER visits for croup treatment were highest in children aged 1–2 years and were approximately 1.5 times more prevalent in boys than in girls. Although there were fluctuations during the study period, the number of patients requiring hospitalization or ER visits continued to increase. Prescriptions of antibiotics decreased for croup during hospitalization or in the ER but those of inhaled epinephrine, inhaled steroids, and systemic steroids increased. In addition, only about 0.27% of croup cases exhibited high severity symptoms such as requiring intubation or ICU admission, indicating that such severe cases were very rare. The increase in croup cases was prominent in primary care facilities and was accompanied by an increase in treatment options and the duration of hospitalization within these settings. Therefore, the rise in croup incidence over the past 20 years is considered to be related more to the increased healthcare utilization than to an increase in disease severity.
To date, studies reporting trends in croup hospitalization or ER visits over a long period from the 2000s to the 2010s are lacking. A notable decline was observed in hospitalizations for croup treatment among children under five years old in Ontario, Canada, from 1988 to 2002, largely attributed to the introduction of systemic steroids during the 1990s.6 In another epidemiological study conducted in Alberta, Canada, from 1999 to 2005, ER visit rates did not decrease over the study period.17 A study in the US showed that the incidence of ER visits for croup treatment from 2007 to 2014 did not change significantly.18 In this study, the incidence gradually increased in the 2000s, but there was a sharp increase in 2010 and 2012. This is consistent with studies reporting the detection rate of respiratory viruses in Korea.1920 The increased occurrence of croup appears to be attributable to the increase in respiratory viral infections. However, a previous study reporting the prevalence of respiratory virus infection from 2006 to 2016 in Korea showed that the positive rates of respiratory virus tests were highest in 2010, 2012, and 2016 (50.7–58.7%) compared to those in 2007 (24.5%).19 In addition, from 2008 to 2011, the prevalence of parainfluenza virus, the most common cause of croup, increased in the summer of 2010 and the late spring of 2011.21 Thus, these are consistent with our results of increased hospitalization or ER visits owing to croup treatment in early 2010. Our findings suggest that these broader epidemiological trends in respiratory virus prevalence may be influencing the patterns of croup incidence observed in our study.
The season with the highest incidence of croup was spring, followed by winter in this study. In Korea, bocavirus, parainfluenza virus, and influenza B were mainly identified in spring, and influenza A and RSV were mainly identified in winter between 2006 and 2016.22 In addition, in previous studies of respiratory virus prevalence in the mid-2000s, the prevalences of bocavirus and RSV as well as parainfluenza were highest in winter, which is consistent with the results of our monthly incidence.2324 However, in our study, we were unable to conduct an analysis on the causative viruses of croup. Therefore, caution must be exercised in the interpretation of our findings in this context.
In the late 1970s, studies began to surface, examining the effectiveness of corticosteroids as a treatment for croup.25 By 1983, favorable outcomes for the use of dexamethasone were reported in patients with moderate to severe croup.26 Throughout the 1990s, a series of studies focused on the effectiveness of steroids in addressing croup-related issues.112728 Nebulized steroids, particularly budesonide, gained popularity, and from 1995 onwards, research confirmed the efficacy of polytherapy involving oral dexamethasone and nebulized steroids.29 Moreover, the 1970s research hinted at the short-term benefits of racemic epinephrine in alleviating inspiratory blockages in croup, although evidence for long-term effects was lacking.3031 Even subsequent to this, several studies affirmed the impact of nebulized epinephrine on mitigating upper respiratory tract edema due to vasoconstriction, spanning from the late 1990s to the early 2000s.32333435 A Cochrane review in 2013 established that simple nebulized epinephrine without positive pressure breathing improved the symptoms of croup and shortened the hospitalization period.12 In addition, the use of epinephrine for the treatment of croup began to be described in Nelson’s textbook around the 2010s. In line with these evolving trends in croup treatment, this study investigated the alterations in drug prescription patterns from 2002 to 2019. Over the study period, antibiotic prescriptions dwindled by approximately 40%, whereas prescriptions for nebulized inhaled corticosteroids and epinephrine surged by 1.5 times and 4 times, respectively. Notably, epinephrine use increased rapidly between 2002 and 2011.
Interestingly, croup treatment patterns in hospitalization or ER visits varied significantly based on factors such as the patient’s economic status, geographical region, and the type of medical institution. Tertiary hospitals were observed to prescribe more epinephrine and fewer inhaled corticosteroids compared to primary or secondary hospitals. Additionally, the likelihood of patients receiving three or more medications and staying hospitalized for the median duration of croup treatment was higher in primary or secondary institutions than in tertiary ones. Notably, in Gyeongsang-do, the usage of inhalation epinephrine was lower than in other regions. We assumed that this trend, according to the Korea Children’s Hospital Association, may be attributed to the higher number of children’s hospitals associated with secondary hospitals in Gyeongsang-do, which is more than double that in other regional groups. Such variations could be explained by differing levels of interest in and access to the latest medical knowledge among providers at each institution size. Moreover, we observed that patients with lower economic status were less likely to receive epinephrine inhalation therapy. This trend is likely influenced by the choice of hospital based on economic status, considering that epinephrine is a less expensive drug. A parallel study in the United States, involving inpatient croup cases at 26 children’s hospitals, also noted differences in steroid use between hospitals. However, this study did not consider the type of hospital or the potential regional variations in steroid use by providers.36
One of the notable strengths of this study is its use of a comprehensive nationwide sample cohort encompassing a substantial number of children and spanning an extended study duration. There has been a dearth of research examining changes in croup incidence and treatment over the past two decades using data on a national scale. Nonetheless, it is important to acknowledge that this study followed a retrospective administrative cohort design, which inherently limits the ability to establish definitive causal relationships. In addition, we relied on the definitions of croup and comorbidities based on the ICD-10 codes for health claims. The medical records of the participants could not be accessed in this database; therefore, it was not possible to verify the accuracy of the diagnoses. There might be a disagreement between diagnoses using ICD-10 codes and diagnoses based on symptoms and examination results. Additionally, our outcome of interest was defined only as hospitalizations or ER visits with a principal diagnosis of croup, not the overall incidence of croup. Furthermore, we were not aware of the viruses that caused the croup. This limitation highlights the need for further research to directly identify and analyze the viruses responsible for croup, which would provide a more comprehensive understanding of the disease’s etiology and optimal management strategies. Last, with the outbreak of severe acute respiratory syndrome coronavirus 2, studies about the association with coronavirus disease variants such as omicron and croup are coming out in Korea,37 but due to database access policy, trends after 2019 could not be confirmed. We hope that further research on this will continue.
This administrative cohort study utilizing a broad national sample showed a rising pattern in both hospitalizations and ER visits aimed at addressing croup among children under the age of 5 years, spanning from 2002 to 2019. Furthermore, the study revealed shifting trends in croup treatment throughout the study period, wherein prescriptions for systemic corticosteroids, inhaled steroids, and epinephrine notably increased as the preferred therapeutic options.
 XML Download
XML Download