

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Opioids are among the most common analgesics prescribed as they are potent pain relievers.1 However, their prescription has been associated with the risk of dependence and addiction,2 contributing to the current global opioid epidemic.3 A recent study reported that the risk of opioid abuse and dependence was the highest in six countries, namely Australia, Canada, France, Germany, United Kingdom, and United States,4 suggesting that the opioid epidemic is currently one of the most important public health issues.
Opioid administration can cause a range of side effects, including sedation, dizziness, nausea, vomiting, constipation, and respiratory depression.5 Moreover, opioid therapy is known to have an immunosuppressive effect,6 which may lead to various adverse health outcomes.7 Population-based cohort studies have consistently reported that opioid use is associated with increased mortality,8910 with similar results reported in South Korea.1112 However, these studies have primarily focused on the effect of long-term or chronic opioid use on long-term prognosis using relatively small sample sizes.89101112 While both short- and long-term opioid use can affect long-term mortality in the general adult population; the exact nature of this association remains controversial.
Therefore, this study aimed to investigate the association between both short- and long-term opioid use and long-term mortality using a national registration database in South Korea.
METHODS
Study design and ethical statement
This population-based cohort study followed the requirements of the Strengthening the Reporting of Observational Studies in Epidemiology.13
Data source
As South Korea’s sole public health insurance system, the NHIS record data on drug prescriptions, medical procedures, and disease diagnosis, all of which are classified using the International Classification of Diseases, 10th Revision (ICD-10) numbers. The NHIS is an obligatory government health-care system in Korea that covers citizens as well as foreigners who have been in the nation for more than six months. Furthermore, the NHIS supplies information on socioeconomic characteristics and fatalities for all individuals in the NHIS database.14
Study population
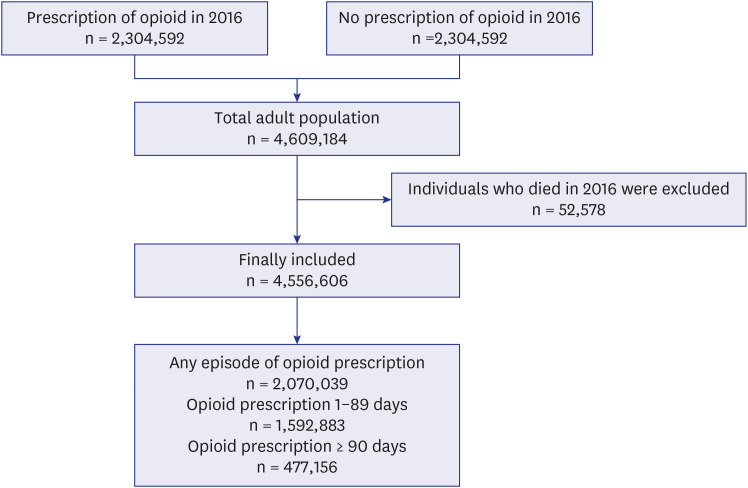
We initially requested the extraction of the data of all adult individuals (≥ 20 years old) who received any opioid prescription from medical institutions in 2016. Data were collected for only one day of opioid prescription for each individual. Thus, 2,304,592 adults receiving a prescription of opioids in 2016 were included. Thereafter, using a 1:1 stratified random sampling technique, considering the age and sex, we requested the extraction of data for 2,304,592 adult individuals in the non-user group who did not receive any opioid prescription between January 1, 2016 and December 31, 2016. Therefore, 4,609,184 adults were screened. After excluding 52,578 individuals who died in 2016, 4,556,606 were included in the analysis. Among them, 2,070,039 were prescribed opioids in 2016. Specifically, 1,592,883 individuals were prescribed opioids for 1–89 days while 477,156 individuals were prescribed opioids for ≥ 90 days. The participants were classified into three groups: non-user, opioid 1–89 days user, and opioid ≥ 90 days user groups according to the criteria of classification of short-term and long-term opioid prescription period.15 To evaluate chronic opioid prescriptions (lasting more than 3 months), data on opioid prescriptions from October 2015 to March 2017 was analysed. This approach was taken to minimize the misclassification of individuals who actually received long-term prescriptions as short-term users due to the relatively brief study period of one year. For instance, patients receiving opioid prescriptions from November 2016 to February 2017 might be inaccurately categorized as short-term users. The selection process for the study population is illustrated in Fig. 1.
Study endpoint
The primary endpoint in this study was 5-year all-cause mortality, which was evaluated from January 1, 2017 to December 31, 2021.
Collected covariates
All information regarding the covariates used in the analyses were collected in 2016. Demographic data included age and sex. Socioeconomic status-related information was assessed using household income levels and residences. Regarding household income, individuals who were too poor to pay insurance premiums were classified into the medical aid program group by the NHIS. All other patients were classified into four groups using quartile ratios (Q1 [lowest], Q2, Q3, and Q4 [highest]). Residences were classified into urban (Seoul or other metropolitan cities) and rural (all other areas). Information regarding underlying disabilities was collected as all disabilities must be registered in the NHIS database to be eligible for receiving various benefits from the social welfare systems in South Korea. All disabilities should be determined legally by a specialist doctor based on the criteria of difficulty in maintaining daily life activities due to disability. Underlying disability was categorized according to severity, distinguishing between mild-to-moderate and severe disability. To reflect the comorbid status of patients, 31 underlying diseases in the Elixhauser Comorbidity index were collected.16 Prescription data for other analgesics such as paracetamol, nonsteroidal anti-inflammatory drugs, gabapentin, and pregabalin were collected. Underlying musculoskeletal diseases such as osteoarthritis, low back pain, neck pain, gout, and other musculoskeletal diseases were collected as covariates because they necessitated opioid prescriptions. The ICD-10 codes of the underlying musculoskeletal diseases are displayed in Supplementary Data 1.
Statistical analysis
Percentages and interquartile ranges were used to represent categorical and continuous variables, respectively. Continuous variables were found to have a non-normal distribution, as indicated by the Kolmogorov-Smirnov test. The Mann-Whitney U Test and χ2 test were employed to test for the between-group comparisons of continuous and categorical variables, respectively.
We employed a multivariable Cox regression model to examine whether the opioid user group showed higher long-term mortality than the non-user group. All covariates were included in the adjusted model. Moreover, we fitted another multivariable Cox regression model for 5-year all-cause mortality after classifying the opioid user group into two subgroups–the 1–89 days opioid user and ≥ 90 days opioid user groups–to investigate whether the prescription period affects results. All results were presented as hazard ratios (HRs) with 95% confidence intervals (CIs), and log-log plots were used to confirm that the central assumptions of the Cox proportional hazard models were satisfied. There was no multicollinearity between the variables in the multivariate model, with variance inflation factors below 2.0. All statistical analyses were performed using IBM SPSS for Windows (version 25.0; IBM Corp., Armonk, NY, USA), and a P value < 0.05 was deemed statistically significant.
Ethics statement
Because this investigation used publicly available data, the Institutional Review Board (IRB) waived protocol deliberation (IRB number: X-2307-840-903). The National Health Insurance Service (NHIS) authorized the study protocol (NHIS approval number: NHIS-2023-1-115) and permitted data access. The IRB waived the necessity for informed consent because the study used retrospectively collected anonymised data.
RESULTS
Study population
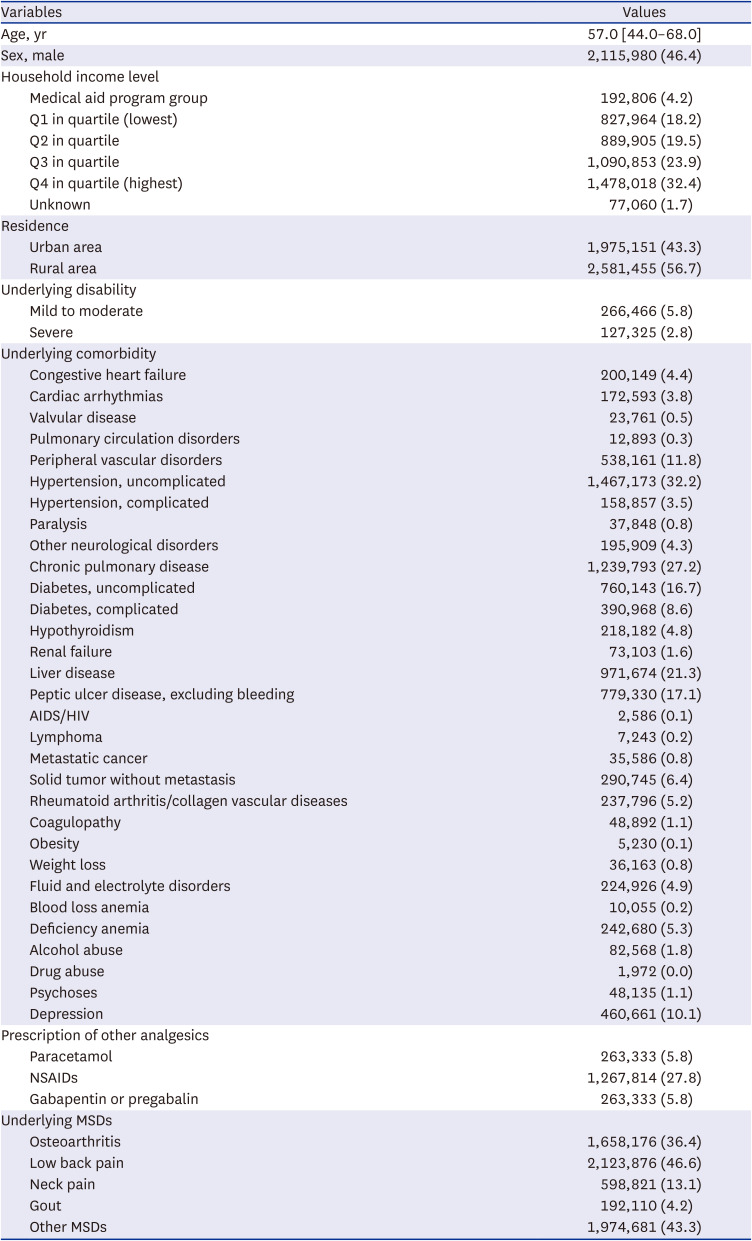
Fig. 1 shows a flowchart depicting the participant selection process in this study. The NHIS initially screened 2,304,592 adult individuals who were prescribed opioids in 2016 and extracted 2,304,592 controlled individuals as the non-user group. Thus, a total of 4,609,184 adult individuals were screened in 2016. After excluding 52,578 individuals who died in 2016, 4,556,606 adults were included in the study. Of these, 2,070,039 patients were prescribed opioids at least once. Specifically, 1,592,883 adult individuals were prescribed opioid for 1 day to 89 days, while 477,156 adults were prescribed opioids for 90 days or more. Table 1 shows the clinicopathological characteristics of the study population.
Table 1
Clinicopathological characteristics of the study population (N = 4,556,606)
Opioid use and mortality
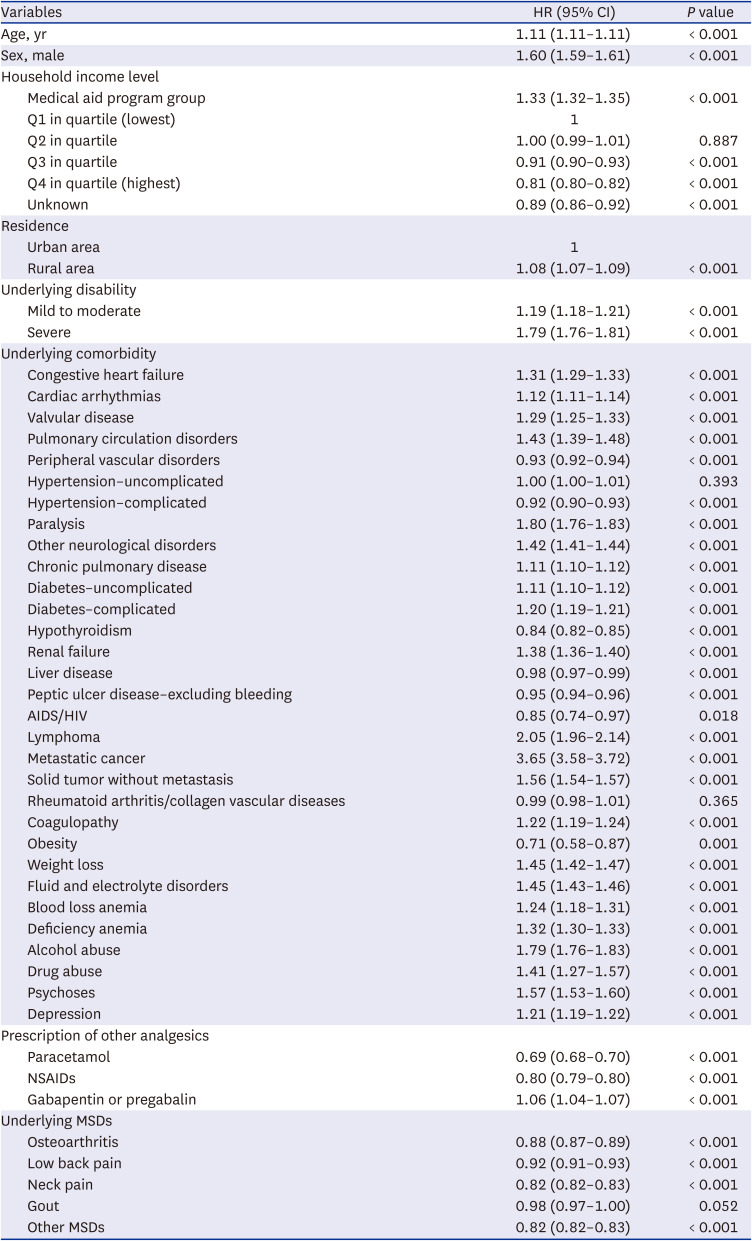
Table 2 shows the comparison of clinicopathological characteristics between opioid users and non-users. The 5-year all-cause mortality rate was higher in the non-user group (6.1%; 151,130/2,486,567) than in the opioid user group (5.6%; 115,216/2,070,039). However, as depicted in Table 3, after covariate adjustment, multivariable Cox regression model 1 showed that the opioid user group was associated with a 28% (HR, 1.28; 95% CI, 1.26–1.29; P < 0.001) higher risk of 5-year all-cause mortality than the non-user group. Moreover, the multivariable Cox regression model 2 showed that the opioid 1–89 days user group and opioid ≥ 90 days user group were associated with 15% (HR, 1.15; 95% CI, 1.14–1.17; P < 0.001) and 49% (HR, 1.49; 95% CI, 1.47–1.51; P < 0.001) higher risk of 5-year all-cause mortality, respectively, compared with the non-user group. All HRs with 95% CIs of the other covariates included in multivariable Model 1 are presented in Table 4. Old age (HR, 1.11; 95% CI, 1.11–1.11; P < 0.001), male sex (vs. female sex HR, 1.60; 95% CI, 1.59–1.61; P < 0.001), living in rural area (vs. urban area; HR, 1.08; 95% CI, 1.07–1.09; P < 0.001), mild to moderate disability (HR, 1.19; 95% CI, 1.18–1.21; P < 0.001), severe disability (HR, 1.79; 95% CI, 1.76–1.81; P < 0.001) and various underlying comorbidities were associated with an increased risk of 5-year all-cause mortality.
Table 2
Comparison of clinicopathological characteristics between opioid users and non-users
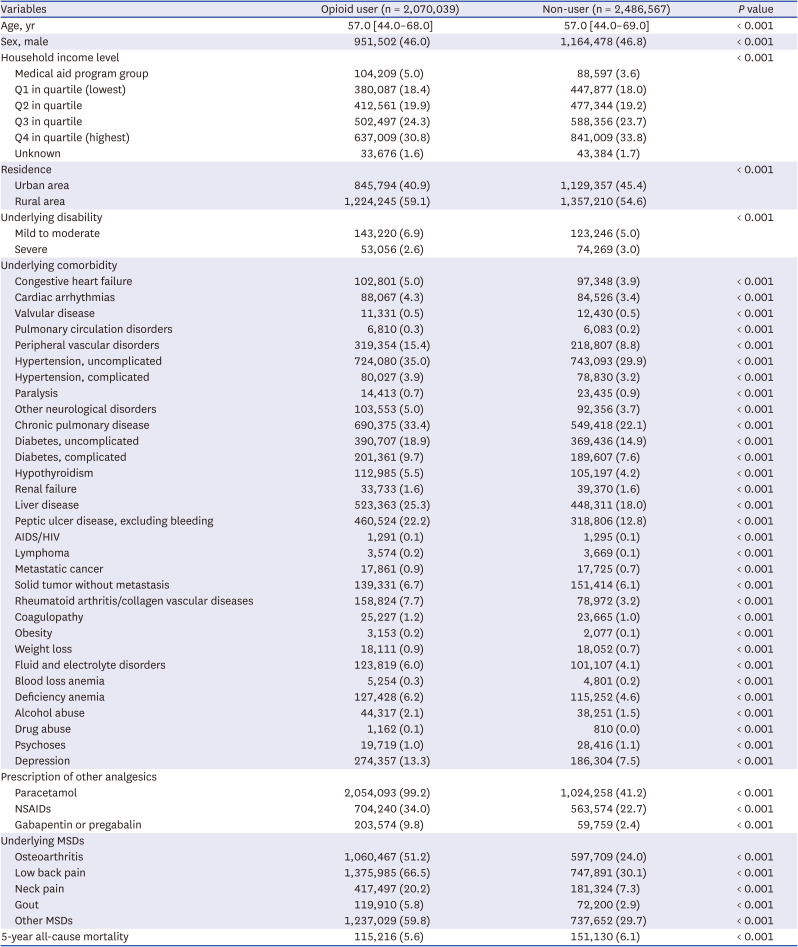
Table 3
Multivariable cox regression model for 5-year all-cause mortality (event N = 266,177, 5.8%)
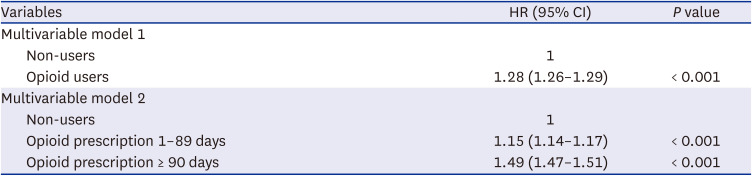
Table 4
All HRs with 95% CIs of the other covariates included in multivariable model 1
DISCUSSION
This population-based cohort study showed that opioid prescriptions are associated with increased long-term mortality within the adult population of South Korea. Moreover, this association was significantly evident in both short- and long-term opioid prescription periods. These findings suggest that both long-term and short-term opioid use could contribute to a worsened long-term prognosis among adults.
Long-term opioid therapy poses many risks and is a major public health concern, as it can lead to dependence, addiction, misuse, and overdose.17 In the United States, death due to opioid-related overdoses have tripled, increasing from 2006 to 2016, and health care costs, criminal justice expenses, and productivity losses associated with opioid misuse were estimated to total $78.5 billion.1819 Moreover, cohort studies in Korea have reported that the number of opioid users in the general population has increased and that opioid use is associated with increased mortality,111220 suggesting that long-term opioid use is becoming a major public health concern that cannot be ignored in Korea.
As a direct effect, long-term opioid therapy can cause various medical problems,21 which could be related to increased long-term mortality. The most common cause of mortality from an opioid overdose or misuse is opioid-induced respiratory depression.22 Opioid-induced respiratory depression could be linked to obstructive sleep apnoea because opioids impair upper airway function and disrupt respiratory control, resulting in central apnoea, upper airway obstruction, and hypoxemia during sleep.23 Long-term opioid therapy may induce immune system alterations, which can be elucidated by modifications in both the innate and adaptive immune systems.24 The immunosuppression associated with opioid prescription was linked to an increased risk of infection such as pneumonia25 and cancer through carcinogenesis due to long-term opioid therapy.26 Moreover, chronic opioid therapy was related to an elevated incidence rate ratio of 2.66 (95% CI, 2.30–3.08) for myocardial infarction compared with that in the general population.27 This is because chronic opioid use was associated with alterations in the serum concentrations of triglycerides and total high-density lipoprotein and low-density lipoprotein cholesterol,28 which could elevate risk of myocardial infarction.24
The exact physical condition that warranted opioid prescription could have also affected the results of this study. It was well reported that patients with chronic pain had higher prevalence of all comorbidities than those without chronic pain.29 In patients with knee osteoarthritis, comorbid hypertension, gastrointestinal disease, and depressed mood were independently associated with opioid use.30 In this study, as shown in Table 2, the opioid user group shows a higher proportion of 26 medical illnesses with regard to the Elixhauser Comorbidity index than the non-user group. Thus, the physical conditions related to opioid prescription may increase the 5-year all-cause mortality rate in the opioid user groups in this study.
Although the adverse effects of long-term opioid therapy are well established, the effect of short-term opioid therapy on long-term mortality remains to be identified. We included patients who were prescribed opioids for 1–89 days in 2016 and analysed their impact on 5-year all-cause mortality using large sample sizes. Short-term opioid users are at risk of progressing to long-term opioid use,15 which may worsen long-term survival outcomes. However, the corresponding clinical significance could be questionable in this study as the risk among short-term opioid users was low with an HR of 1.15 (95% CI, 1.14–1.17) based on a sample size of 4,556,606 individuals. Therefore, further studies to identify the impact of both short- and long-term opioid use on long-term mortality are warranted.
Additional important findings regarding 5-year all-cause mortality were depicted among the covariates in multivariable modelling, regardless of opioid use. Poor household income (medical aid program group) was a significant risk factor for increased 5-year all-cause mortality, whereas the high household income group (Q3 and Q4) was associated with decreased 5-year all-cause mortality. Income inequality was associated with mortality in the United States,31 which was also observed in South Korea in the present study. Living in rural areas was also associated with an increased 5-year all-cause mortality compared to those living in urban areas. Indeed, it has been reported that accessibility to healthcare services could significantly affect mortality,32 and those living in rural areas have limited access to healthcare service centres compared with those living in urban areas, which may have affected the results of this study. Moreover, we included underlying disabilities in addition to the 31 underlying diseases calculated using the Elixhauser comorbidity index. Therefore, our findings were derived from a robust analysis using several covariates.
This study had several limitations. First, opioid dosage was not considered in this study. Second, some important variables such as body mass index, smoking history, and alcohol consumption were not included as covariates because of the lack of information in the NHIS database. Third, because our study used South Korean data from a nationwide registration database, generalizability to other countries may be limited. Finally, residual or unmeasured confounders may have affected the results.
In conclusion, this population-based cohort study showed that opioid prescriptions are associated with increased long-term mortality in adults. Moreover, this association was significantly evident in both short- and long-term opioid users. Future studies to confirm the mechanism between opioid prescriptions and long-term mortality, considering the duration, dosage, and potency of opioid prescriptions, are warranted.
 XML Download
XML Download