

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertrophic cardiomyopathy (HCM) is an inheritable, relatively common cardiomyopathy that affects 1:200–1:500 of the general population.12 Adverse events are common during the natural course of HCM, with up to 30% of patients experiencing heart failure (HF), atrial fibrillation (AF), stroke, or sudden cardiac death (SCD).2345 Aside from SCD, which can be prevented by implantable cardioverter-defibrillator therapy, the life expectancy and quality of life of patients with HCM are largely determined by the occurrence of cardiovascular complications such as HF, AF, and stroke.2 Thus, continuous efforts have been made to identify the prognosticators predicting these events.
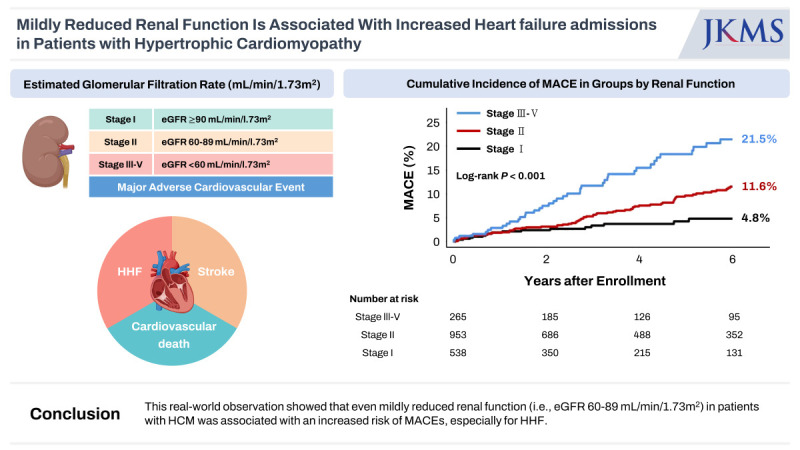
Impaired renal function, defined by an estimated glomerular filtration rate [eGFR] < 60 mL/min/1.73 m2, is one of the well-known prognostic factors for cardiovascular outcomes.67 The adverse effects of mildly reduced renal function (i.e., eGFR 60–89 mL/min/1.73 m2) on cardiovascular outcomes in comparison to normal renal function (i.e., eGFR ≥ 90 mL/min/1.73 m2) have also been reported in a few studies.8910 In the general population, it is suggested that reduced renal function affects the sympathetic nervous system and the renin-angiotensin-aldosterone system, finally contributing to left ventricular (LV) diastolic dysfunction.1112 Given the basic pathophysiology of HCM, i.e., a disease characterized by LV diastolic dysfunction, it is plausible that reduced renal function elevates cardiovascular risk. However, data on the association between renal dysfunction and cardiovascular outcomes in patients with HCM, particularly in relation to mildly reduced renal function, are limited. We thus aimed to evaluate the long-term risk of cardiovascular events among groups determined by renal function in a sizable multicenter HCM cohort, stratifying patients into three distinct groups based on their eGFR values (see Methods section for details).
METHODS
Study design and participants
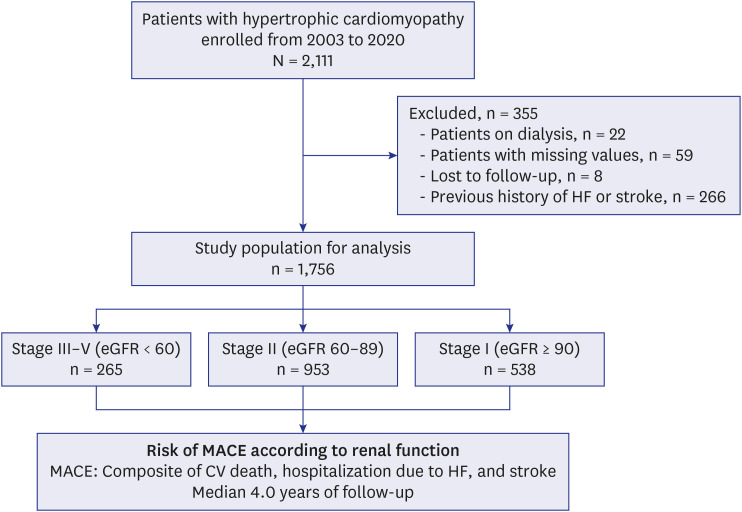
The study population included patients with HCM who underwent initial echocardiography at two tertiary referral hospitals in Korea (Seoul National University Hospital and Seoul National University Bundang Hospital) between 2003 and 2020. HCM was defined as increased LV wall thickness (end-diastolic LV wall thickness ≥ 15 mm or ≥ 13 mm in patients with a family history of HCM) that could not be explained by other causes, such as hypertension and aortic stenosis.313 Subjects were excluded if: 1) they were on dialysis; 2) serum creatinine level was unavailable; 3) they were lost to follow-up; or 4) they had a previous history of HF or stroke (Fig. 1).
Fig. 1
Study flow of patients. Patients diagnosed with hypertrophic cardiomyopathy and without a previous history of HF or stroke were enrolled. MACE, a composite of CV death, hospitalization for HF, and stroke, during median 4.0 years of follow-up was analyzed according to the groups stratified by renal function (stage III–V, eGFR < 60 mL/min/1.73 m2; stage II, eGFR 60–89 mL/min/1.73 m2; and stage I, eGFR ≥ 90 mL/min/1.73 m2).
eGFR = estimated glomerular filtration rate, HF = heart failure, CV = cardiovascular, MACE = major adverse cardiovascular event.
Renal function evaluation and categorization
The eGFR at enrollment was used to evaluate the renal function of study participants. The eGFR of each patient was calculated using the simplified four-component Modification of Diet in Renal Disease equation that included age, race, gender, and serum level of creatinine; i.e., eGFR = 186 × (Serum Creatinine Level [in mg/dL]) − 1.154 × (Age [in Years]) − 0.203.14 The result was multiplied by a correction factor of 0.742 for the women. Patients were then divided by their renal function as follows: stage I (normal renal function with eGFR ≥ 90 mL/min/1.73 m2), stage II (mildly reduced renal function with eGFR 60–89 mL/min/1.73 m2), and stage III–V (overt renal dysfunction with eGFR < 60 mL/min/1.73 m2) groups, according to the Kidney Disease: Improving Global Outcomes (KDIGO) 2012 guidelines.15
Echocardiographic examination
Commercially available echocardiography machines (GE Medical Systems, Philips Healthcare, and Siemens Medical Solutions) were used. LV dimensions, end-diastolic wall thickness, LV ejection fraction (LVEF), and left atrial dimensions were obtained in accordance with the current guidelines.16 The LV outflow tract (LVOT) pressure gradient was estimated at rest and with the Valsalva maneuver, and the maximum value was recorded. Patients with a maximal LVOT gradient of ≥ 50 mmHg were classified as having significant dynamic LVOT obstruction (LVOTO). The ratio of early diastolic mitral inflow velocity (E) to early septal mitral annular velocity (e′) was used for LV filling pressure assessment. Apical HCM was defined as LV hypertrophy affecting only the apical segments.
Study outcomes and follow-up
The primary outcome was major adverse cardiovascular events (MACEs) defined as a composite of cardiovascular death, hospitalization for HF (HHF), and stroke. The secondary outcomes were the individual components of the primary outcome. The occurrence and causes of death were confirmed using the National Death Registration Records of Korea. Cardiovascular death was defined as death due to HF, myocardial infarction, cardiac arrest, ischemic stroke, or hemorrhagic stroke.17 HHF was defined as at least one episode of hospital admission for HF that was clinically diagnosed based on worsening symptoms and signs of congestion with volume overload, such as dyspnea and peripheral edema, or the use of diuretics due to volume overload.18 Stroke was defined as a sudden neurological deficit originating from brain vascular lesions, including thromboembolism, hemorrhage, or a ruptured aneurysm that persisted for more than 24 hours.19 Dedicated research personnel collected the clinical outcomes by reviewing electronic medical records and conducting telephone interviews. The date of the initial echocardiography was designated as the index date. The study participants were followed up from the index date until the event, end of follow-up, or death, whichever occurred first. Follow-up was censored at the 6-year time point for primary and secondary outcomes.
Statistical analysis
Categorical variables are presented as numbers and frequencies (percentages) and were compared using the χ2 test. Continuous variables are expressed as mean ± standard deviation and were compared using the Student’s t-test. Cumulative event rates were estimated using Kaplan-Meier censoring estimates, and the log-rank test was used to compare clinical outcomes among groups according to renal function. A multivariable Cox regression model was used to adjust for the confounding factors. Covariates included in the multivariable model were selected if they were significantly different between the two groups or assumed to have predictive values, which are listed as follows: age ≥ 60 years, sex, body mass index (BMI) ≥ 25 kg/m2, hypertension, diabetes mellitus, history of myocardial infarction, LVEF, significant dynamic LVOTO, systolic blood pressure, use of beta-blockers, and apical form of HCM (Supplementary Table 1). In addition, the primary outcome was compared among the subgroups of interest according to renal function, and the interactions between each subgroup were assessed using a multivariable Cox regression model. All probability values were two-sided, and statistical significance was set at P < 0.05. The statistical software package Stata (version 17.0; Stata Corp., College Station, TX, USA) was used for statistical analyses.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of each hospital (IRB No. H-2204-051-1314, Seoul National University Hospital) and was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for written informed consent was waived because of the retrospective nature of this study. Data supporting the findings of this study can be obtained from the corresponding author upon request.
RESULTS
Characteristics of study population
Table 1 shows the baseline characteristics of the study population according to the groups stratified by renal function. Of the 1,756 patients with HCM, 538 (30.6%) had stage I renal function, 953 (54.3%) had stage II renal function, and 265 (15.1%) had stage III–V renal function. The mean eGFRs were 102.3 ± 12.3 mL/min/1.73 m2, 75.8 ± 8.4 mL/min/1.73 m2, and 49.7 ± 8.8 mL/min/1.73 m2 in the stage I, II, and III–V groups, respectively. The stage III–V and II groups were at a more advanced age than the stage I group, whereas the sex distribution and BMI levels were similar among the three groups. The proportions of patients with hypertension, diabetes mellitus, and a history of AF were significantly higher in the stage III–V and II groups than in the stage I group. Although the difference among the three groups was not statistically significant for LVEF, patients with worse renal function (stage III–V and II groups) had greater LV chamber size, E/e′ ratio, and left atrial diameter, with lower E and septal e′ velocities. The proportion of patients with significant dynamic LVOTO was significantly lower in the stage III–V group. The number of patients taking beta-blockers was lower in the stage III–V and II groups than in the stage I group.
Table 1
Baseline characteristics of subjected patients by stages of renal function
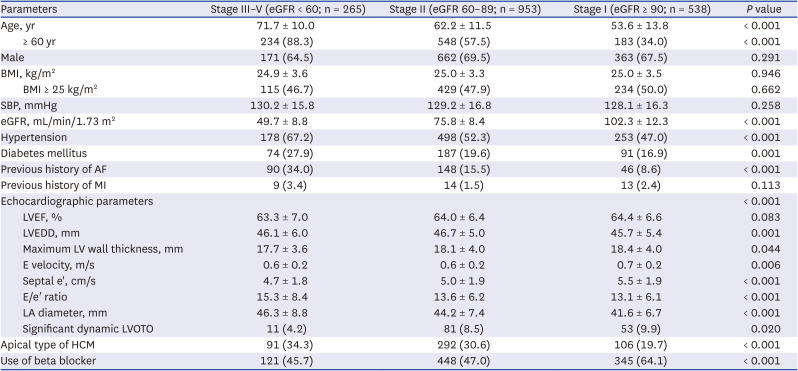
Values are presented as number (%) or mean ± standard deviation.
eGFR = estimated glomerular filtration rate, BMI = body mass index, SBP = systolic blood pressure, AF = atrial fibrillation, MI = myocardial infarction, LVEF = left ventricular ejection fraction, LVEDD = left ventricular end-diastolic dimension, LV = left ventricular, E velocity = early diastolic transmitral inflow velocity, Septal e′ = early diastolic mitral annular velocity, LA = left atrial, LVOTO = left ventricular outflow tract obstruction, HCM = hypertrophic cardiomyopathy.
Clinical outcomes according to renal function
During a median follow-up of 4.0 years (Q1–Q3 1.6–6.0 years), 127 events (cumulative incidence of 11.5%) of MACE (cardiovascular death, n = 37 [3.5%]; HHF, n = 67 [6.0%]; or stroke, n = 41 [4.1%]) occurred, with significant differences among the groups stratified by renal function (P < 0.001) (Fig. 2).
Fig. 2
Cumulative incidence of MACE in groups by renal function. When MACE was defined as a composite of all-cause death, hospitalization for heart failure, and stroke, the cumulative incidence of MACE was significantly higher even in patients with stage II renal function, as compared to those with stage I renal function.
eGFR = estimated glomerular filtration rate, MACE = major adverse cardiovascular event.
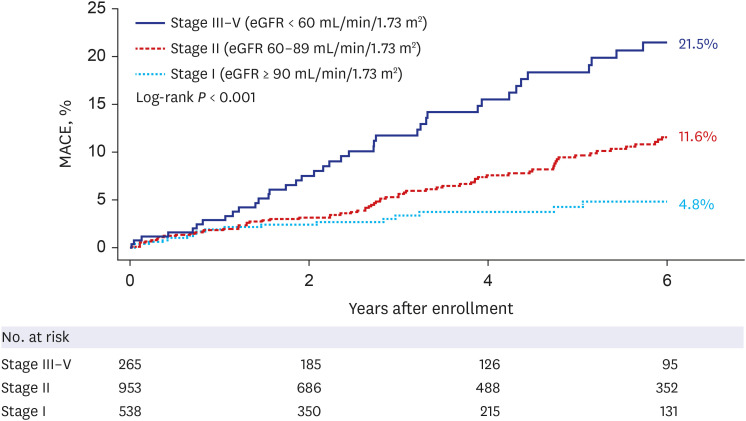
Fig. 3 depicts a comparison of the cumulative incidences and adjusted risks of MACE and each individual outcome among the three groups. In patients with HCM with stage III–V renal function, the incidence of MACE was significantly higher compared with that in patients with stage I renal function (multivariable-adjusted hazard ratio [aHR], 2.71; 95% confidence interval [CI], 1.39–5.27; P = 0.003). For individual outcome, the stage III–V renal function group had higher risks of cardiovascular death (aHR, 3.08; 95% CI, 0.92–10.30; P = 0.068) and HHF (aHR, 2.79; 95% CI, 1.16–6.71; P = 0.022) than the stage I renal function group, but statistical significance was achieved only for the HHF. The stage III–V renal function was not associated with an increased risk of stroke compared with stage I renal function (aHR, 1.05; 95% CI, 0.31–3.61; P = 0.938).
Fig. 3
Risks of MACE and its individual components in each category of renal function. The number of events, cumulative incidence, and multivariable-adjusted HR with 95% CI of MACE (a composite of all-cause death, hospitalization due to HF, and stroke) and its individual outcomes are illustrated in each category of renal function with stage I as a reference.
MACE = major adverse cardiovascular event, HF = heart failure, HR = hazard ratio, CI = confidence interval.
aAdjusted for age ≥ 60 years, sex, body mass index ≥ 25 kg/m2, hypertension, diabetes mellitus, previous history of myocardial infarction, left ventricular ejection fraction, significant dynamic left ventricular outflow tract obstruction, systolic blood pressure, use of beta blocker, and apical type of hypertrophic cardiomyopathy.
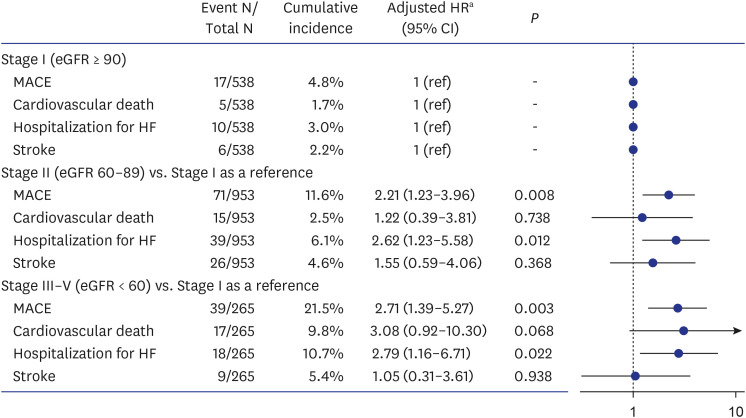
In the stage II renal function group, the adjusted risk of MACE was significantly higher than in the stage I renal function group (aHR, 2.21; 95% CI, 1.23–3.96; P = 0.008), which was mainly driven by a significantly elevated risk of HHF in the stage II group (vs. stage I: aHR, 2.62; 95% CI, 1.23–5.58; P = 0.012). The incidences of cardiovascular death (aHR, 1.22; 95% CI, 0.39–3.81; P = 0.738) and stroke (aHR, 1.55; 95% CI, 0.59–4.06; P = 0.368) were not statistically different between the stage II and I groups. The results were consistent in various multivariable models including AF (Supplementary Table 2) or parameters of LV diastolic dysfunction (Supplementary Table 3).
Subgroup analysis
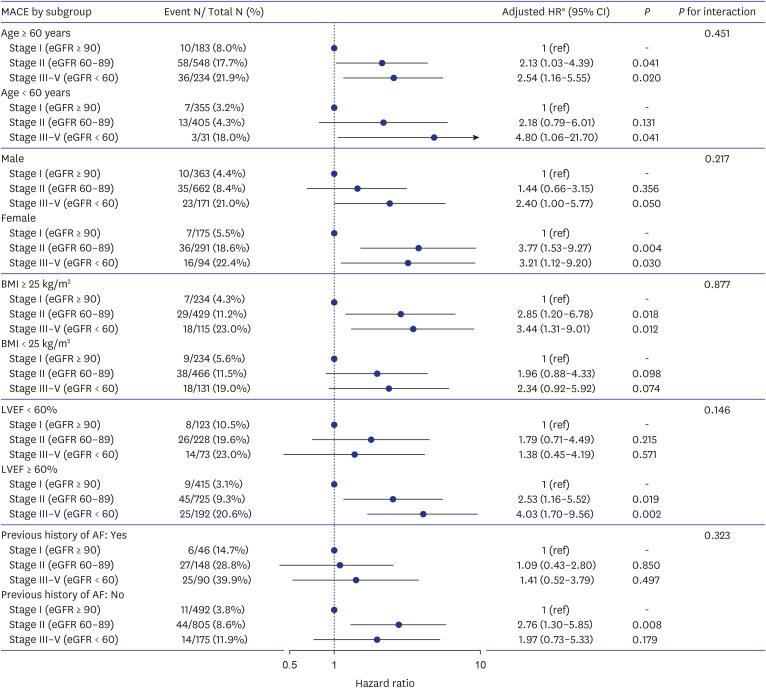
Fig. 4 summarizes the results of the subgroup analysis. No statistically significant interaction was observed in the risk of MACE in terms of the different subgroups (P for interaction in all subgroups > 0.05). However, an increased risk of MACE in patients with impaired renal function tended to be more prominent in women, BMI ≥ 25 kg/m2, LVEF ≥ 60%, or without a history of AF.
Fig. 4
Subgroup analysis by age, sex, BMI, LVEF, and previous history of AF.
MACE = major adverse cardiovascular event, HR = hazard ratio, CI = confidence interval, eGFR = estimated glomerular filtration rate, BMI = body mass index, AF = atrial fibrillation, LVEF = left ventricular ejection fraction, ref = reference.
aAdjusted for age ≥ 60 years, sex, body mass index ≥ 25 kg/m2, hypertension, diabetes mellitus, previous history of myocardial infarction, left ventricular ejection fraction, significant dynamic left ventricular outflow tract obstruction, systolic blood pressure, use of beta blocker, and apical type of hypertrophic cardiomyopathy, except for each corresponding variable for subgroup.
DISCUSSION
In this large, two-center HCM cohort, more than half (54.3%) of the patients had stage II renal function (i.e., mild renal dysfunction) and 15.1% had stage III–V renal function. Given the elevated risk of end-stage renal disease in patients with HCM,7 clinicians need to closely monitor and regularly follow up patients with HCM and mild renal dysfunction for kidney and cardiovascular outcomes.
This study can be summarized as follows. First, patients with HCM with stage II and III–V renal function had a significantly increased risk of MACEs compared with those with stage I renal function. Second, the increased risks of MACEs in the stage II and III–V renal function groups were mainly driven by a significantly higher risk of HHF. Third, the risk of cardiovascular death increased only in the stage III–V renal function group with borderline statistical significance, whereas stage II renal function was not associated with the elevated risk of cardiovascular death. Fourth, stroke risk was not associated with the degree of renal function. Lastly, a subgroup analysis showed that women with HCM, those with obesity or normal LVEF (defined as ≥ 60%) or those without a history of AF tended to be at increased risk of MACE in the presence of renal dysfunction, even in the stage II renal function.20
Chronic kidney disease is a well-known risk factor for cardiovascular events in the general population.6 However, the association between renal dysfunction and cardiovascular outcomes in patients with HCM remains underexplored. While the prevalence of stage III–V renal function in the general population is at 0.35%, it is significantly higher in HCM patients, ranging from 16–38%.2122 Similar to the general population, HCM patients with stage III–V renal function demonstrate an elevated risk of cardiovascular events. For instance, in a cohort of 581 Chinese patients with HCM, 90 individuals (16.0%) with an eGFR < 60 mL/min/1.73 m2 exhibited a higher incidence of mortality and hospitalization due to HF compared to those with an eGFR ≥ 60 mL/min/1.73 m2.21 Additionally, a Japanese study including 450 HCM patients found that the subset with stage III–V renal function (n = 171) had an elevated risk of SCD.22 Our study aligns with these findings, demonstrating that HCM patients with stage III–V renal function had a significantly higher risk of MACEs, primarily driven by an increased risk of cardiovascular death and HHF.
A previous study has shown that patients with HCM have a much higher risk of mortality due to cardiovascular causes than those without HCM.23 We also noted a borderline threefold increase in the risk of cardiovascular death in the stage III–V renal function group compared with the stage I group. The risk of cardiovascular mortality was similarly increased in 90 Chinese patients with HCM with stage III–V renal function (aHR, 2.98; 95% CI, 1.36–6.50).21 Taken together, a higher mortality risk in patients with HCM and overt renal dysfunction can be largely explained by cardiovascular causes.
HF is a major cardiovascular complication of HCM and significantly affects quality of life and prognosis.24 Alteration in renal function is recognized to be directly associated with short- and long-term deterioration in cardiac function and incident HF.25 Decreased renal function activates the sympathetic nervous system and the renin-angiotensin-aldosterone system, and subsequent electrolyte imbalances may also promote an inflammatory response and change the myocardial structure, resulting in a proarrhythmic condition.11 Renal dysfunction is also linked to LV diastolic dysfunction in a spectrum of cardiovascular conditions.12 In the current study, an approximately threefold increase in the cumulative incidence of HHF was noted in patients with stage III–V renal function compared with the stage I renal function group. Thus, it is plausible that HCM itself and reduced renal function have a synergistic effect on incident HF in patients with HCM.
It is well established that an eGFR < 60 mL/min/1.73 m2 is a significant prognostic factor for cardiovascular disease in the general population as well as patients with HCM. However, the impact of mildly reduced renal function on cardiovascular risk remains controversial. This is crucial given that nearly 40% to 60% of the general population have mildly reduced renal function.1026 Various studies have investigated the prognostic significance of this condition in diverse groups. The subgroup analysis of the VALIANT trial identified mildly reduced renal function, defined as an eGFR of 60.0–74.9 mL/min/1.73 m2, as a major risk factor for cardiovascular events after myocardial infarction.9 Similarly, the Framingham Offspring Study also reported elevated risks of cardiovascular diseases in individuals with eGFR ranges of 60–69 and 70–79 mL/min/1.73 m2, compared to those with eGFR ≥ 90 mL/min/1.73 m2.10 However, a recent study found that this association was not observed in patients with coronary artery disease who underwent multivessel coronary revascularization.27 Notably, the relationship between mildly reduced renal function and cardiovascular risk remains unknown in HCM patients, who have 40–60% prevalence of stage II renal function.2122
To the best of our knowledge, the present study is the first to show that patients with HCM and mildly reduced renal function have an elevated cardiovascular risk compared with those with normal renal function. Particularly, in our study, HHF was a major driver of adverse cardiovascular events in association with mildly reduced renal function. Several pathophysiological mechanisms could explain this finding. Mildly reduced renal function may be an indirect early indicator of occult vascular disease or elevated levels of inflammatory mediators.2829 When compared with those with normal eGFR over 90 mL/min/1.73 m2, those with eGFR 60–89 mL/min/1.73 m2 had an increased risk of subclinical cardiovascular diseases and had higher levels of surrogate markers, such as growth/differentiation factor-15 and brain natriuretic peptide, indicating myocardial injury.10 Additionally, the burden of coronary artery calcification progresses even in a mildly reduced eGFR range, which was a major predictor of incident HF.3031
At present, early diagnosis and rapid management of cardiovascular comorbidities, such as HF, are becoming more important issues in determining the long-term prognosis of patients with HCM.32 Hence, our findings highlight the clinical relevance of identifying HCM patients at risk, simply by monitoring eGFR with regular blood test; that is, if eGFR declines below 60 mL/min/1.73 m2, additional attention should be paid to the presence or absence of HF symptoms and/or subclinical coronary disease for the establishment of early interventions. Physicians should also be aware that patients with HCM and mildly reduced renal function, a group accounting for more than 50% of the total HCM population, are more than twice as likely to progress to HF as those with normal renal function. Furthermore, whenever possible, patients with HCM and mildly reduced renal function should undergo screening for cardiometabolic risk factors and receive prompt management for obesity, hypertension, diabetes mellitus, and dyslipidemia.
Notably, sodium-glucose transporter protein 2 (SGLT2) inhibitors are reported to prevent the progression of chronic kidney disease and reduce MACEs in patients with HF, irrespective LVEF.3334 Given the results of this study, further research exploring whether SGLT2 inhibitors could provide benefits in HCM patients with mildly reduced renal function may be of merit.
We observed that women with HCM and obesity, normal LVEF, or the absence of AF were subgroups in which the association between mildly reduced renal function and the risk of MACEs was more pronounced. Some points need to be mentioned based on these findings. First, given the absolute cutoff value of LV wall thickness required to diagnose HCM without considering body surface area, HCM can be presumed to be already in an advanced stage when diagnosed in women.35 Therefore, despite the lower cardiovascular risk profile in women in the general population,36 women with HCM are more likely to manifest with advanced HF symptoms leading to hospitalization and thus have worse prognosis.1735 Also, the increased susceptibility to HF admission in women with HCM, particularly those with mildly reduced renal function, may have been influenced by biological differences such as sex hormone levels including estrogen.37 Second, the risk of cardiovascular events in patients with HCM and reduced renal function seem to be partly modified by obesity. Individuals with obesity were reported to have a significantly higher incidence of clinical HCM; thus, obesity can be regarded as a modifiable risk factor for HCM.38 Moreover, obesity contributes to an increased risk of unfavorable outcomes in individuals with HCM, particularly rehospitalization for HF.39 Obesity is also independently associated with increased LV mass and unfavorable LV remodeling, suggesting that obesity may determine the progression of HF symptoms.40 Indeed, BMI is one of the most relevant factors in explaining HF-related symptoms in a cohort of patients with chronic kidney disease.41 Finally, decreased LVEF and the presence of AF are established predictors of cardiovascular mortality and HHF in patients with HCM.2042 Therefore, in the presence of decreased LVEF or AF, renal dysfunction is anticipated to increase the risk of MACEs by acting as an accomplice. However, we observed no increase in the risk of MACEs in patients with decreased LVEF or AF, while patients with preserved LVEF or without AF had a significantly higher relative risk of MACEs. We speculate that HCM patients with decreased LVEF or AF may have received closer monitoring and thus appropriate HF-related medications, thereby attenuating the adverse impact of renal dysfunction on the risk of MACEs. Conversely, patients with preserved LVEF or without a previous history of AF may have received less attention to renal dysfunction. However, patients with HCM with LVEF ≥ 60% and mild renal dysfunction had a similar incidence rate of MACEs as those with LVEF < 60% but normal renal function (9.3% vs. 10.5%; Fig. 4). Furthermore, the incidence of MACEs in patients without a previous history of AF, but with mild renal dysfunction was 8.6% (44/805; Fig. 4), a value that cannot be overlooked in our daily clinical practice. Taken together, even mild renal dysfunction can play a significant role in cardiovascular risk and should not be ignored in patients with HCM.
Several limitations need to be acknowledged. First, establishing causality was challenging due to the retrospective nature of the study. Second, data on albuminuria and use of diuretics were unavailable. Third, despite multivariable adjustments, controlling for strong risk factors such as age might not be sufficient. Fourth, renal function was assessed only at enrollment, limiting the consideration of longitudinal changes during follow-up. Finally, serum creatinine levels and eGFR were used as surrogate markers of renal function, although direct GFR measurement with radioactive isotopes or inulin could be more precise.
In conclusion, even mild renal dysfunction is significantly associated with a higher risk of cardiovascular outcomes, particularly HHF.
 XML Download
XML Download