

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ultrasonography during the second trimester has become an important screening tool for structural abnormalities. A major congenital malformation—as is observed in about 20% of fetuses with trisomy 21 and most fetuses with trisomy 13 or 18—is an indication for fetal karyotyping.1 The Society for Maternal-Fetal Medicine (SMFM) proposed guidelines on the evaluation and management of isolated ultrasound soft markers. They do not recommend invasive diagnostic testing for aneuploidy solely for the evaluation of isolated ultrasound soft markers following a negative serum result.2
Previous studies have revealed that the ultrasonographic detection of aneuploidy may be improved by soft markers, but ultrasonographic soft markers are considered to be normal variants rather than fetal abnormalities.34 They include choroid plexus cysts (CPC), echogenic bowel (EB), echogenic intracardiac focus (EIF), hypoplastic nasal bone (HNB), short femur (SF), single umbilical artery (SUA), and urinary tract dilatation (UTD). One or more markers are present in at least 10% of pregnancies.5 The American College of Obstetricians and Gynecologists (ACOG) and the SMFM currently recommend no further invasive diagnostic testing for pregnant people with negative cell-free DNA or serum screening results with isolated ultrasonographic soft markers.26 However, evidence regarding the clinical usefulness of CMA in cases with ultrasonographic soft markers is lacking, even though the risk of chromosomal aberrations may alter clinical decision-making regarding invasive tests.
Chromosomal microarray analysis (CMA) is increasingly being used due to its high detection rate of significant chromosomal abnormalities compared with traditional karyotyping. Karyotyping is limited to detecting numeric aneuploidy and large (≥ 5–10 Mb) chromosomal abnormalities, but CMA can detect microdeletions and micro-duplications with higher resolution.7 Pathogenic copy number variants (CNVs) have been identified in approximately 7.8% (range, 0–50%) of patients with unexplained developmental delay, intellectual disability, or autism spectrum disorder.89
Evidence has recently suggested that CMA can detect additional clinically significant abnormalities in about 6% of fetuses with ultrasonographic soft markers but a normal karyotype.10 Anecdotal reports have described cases with ultrasonographic soft markers in which CMA revealed pathogenic CNVs despite normal results on conventional karyotyping.8910
However, a systematic review focusing on chromosomal aberrations in fetuses with isolated ultrasonographic soft markers has not been published to date. Furthermore, the specific risk of chromosomal aberrations for each soft marker has not been reported. In this conetext, the objective of our study was to evaluate the clinical significance of CMA in pregnancies with isolated ultrasonographic soft markers.
METHODS
Search strategies, study selection and data extraction
An electronic search was conducted by an experienced librarian in the PubMed, EMBASE and Cochrane Library using the following search keywords and their synonyms: “ultrasonographic soft markers,” “chromosomal microarray analysis,” and “copy number variation”. The search was updated in July 2022. The selection criteria of studies are shown in Fig. 1. For each study, the following information was extracted: the first author’s name, pregnancy outcome, inclusion criteria of this article, fetal ultrasonographic findings, results of the CMA pattern of inheritance, and CNV descriptions. All abstracts or titles were screened by two reviewers (U Kim and YM Jung), and full papers potentially eligible for citation were obtained.
Fig. 1
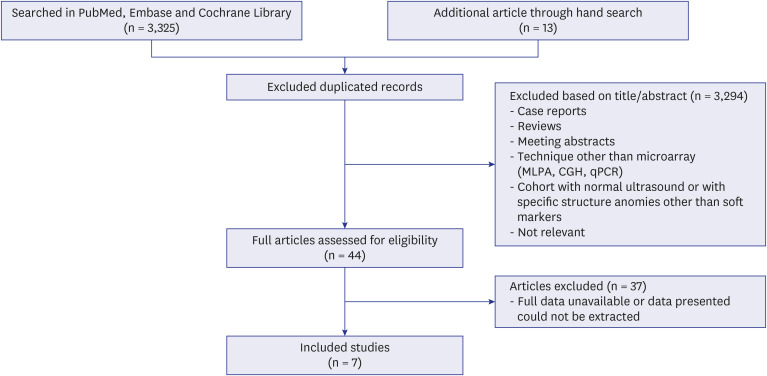
Flow-chart showing the study selection process.
MLPA = multiplex ligation-dependent probe amplification, CGH = comparative genomic hybridization, qPCR = quantitative polymerase chain reaction.
Studies that met the following criteria were included: 1) published in English; 2) women with singleton pregnancies; 3) fetuses that underwent detailed sonography for anomaly detection and had isolated ultrasonographic soft markers during the second trimester; 4) any invasive diagnostic test (amniocentesis or chorionic villi sampling) was performed for conventional karyotyping or CMA and conventional karyotyping showed fetal euploidy.
RESULTS
A total of 3,325 records were identified through the database search and 13 articles were added through hand searching using the keywords given mentioned above. After duplicate articles were removed, 3,237 articles were excluded after a review of their abstracts. Forty-four remaining articles were fully reviewed. Two studies lacking information about karyotyping and 8 studies with ultrasonographic findings other than soft markers were excluded. Twenty-seven studies not providing full information about the single-nucleotide polymorphism (SNP) arrays of the CMAs were also excluded (Fig. 1).
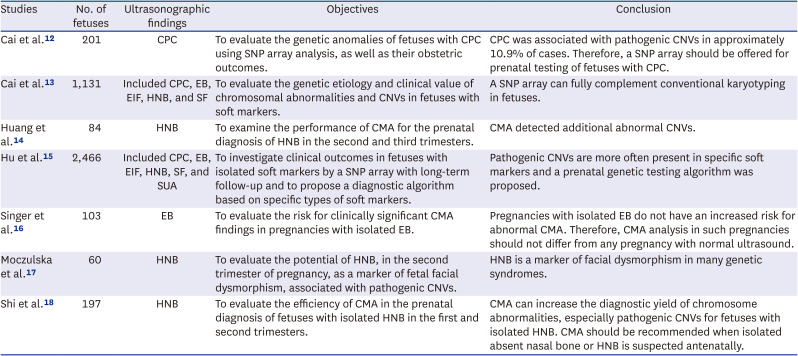
Seven eligible articles were included in the final review, including 2,048 cases with isolated ultrasonographic soft markers. Table 1 summarizes information on the 7 studies included in the current study.12131415161718 Cai et al.12 evaluated the genetic abnormalities of fetuses with CPC using SNP array results. They reported that isolated CPC with normal karyotype was associated with pathogenic CNVs in about 3.9% of cases. Other previous studies on fetuses with ultrasonographic soft markers and CMA are summarized in Table 1. Hu et al.15 examined 2,466 fetuses with six ultrasonographic soft markers, evaluated their clinical outcomes of them by SNP array, and proposed a clinical algorithm based on specific types of ultrasonographic soft markers. Pathogenic CNVs were often found in fetuses with specific ultrasonographic soft markers; therefore, they suggested offering their prenatal clinical algorithm to women whose fetuses have ultrasonographic soft markers. Information regarding other studies is also summarized in Table 1.
Table 1
Previous studies on fetuses with ultrasonographic soft markers and chromosomal microarray analyses
| Studies | No. of fetuses | Ultrasonographic findings | Objectives | Conclusion |
|---|---|---|---|---|
| Cai et al.12 | 201 | CPC | To evaluate the genetic anomalies of fetuses with CPC using SNP array analysis, as well as their obstetric outcomes. | CPC was associated with pathogenic CNVs in approximately 10.9% of cases. Therefore, a SNP array should be offered for prenatal testing of fetuses with CPC. |
| Cai et al.13 | 1,131 | Included CPC, EB, EIF, HNB, and SF | To evaluate the genetic etiology and clinical value of chromosomal abnormalities and CNVs in fetuses with soft markers. | A SNP array can fully complement conventional karyotyping in fetuses. |
| Huang et al.14 | 84 | HNB | To examine the performance of CMA for the prenatal diagnosis of HNB in the second and third trimesters. | CMA detected additional abnormal CNVs. |
| Hu et al.15 | 2,466 | Included CPC, EB, EIF, HNB, SF, and SUA | To investigate clinical outcomes in fetuses with isolated soft markers by a SNP array with long-term follow-up and to propose a diagnostic algorithm based on specific types of soft markers. | Pathogenic CNVs are more often present in specific soft markers and a prenatal genetic testing algorithm was proposed. |
| Singer et al.16 | 103 | EB | To evaluate the risk for clinically significant CMA findings in pregnancies with isolated EB. | Pregnancies with isolated EB do not have an increased risk for abnormal CMA. Therefore, CMA analysis in such pregnancies should not differ from any pregnancy with normal ultrasound. |
| Moczulska et al.17 | 60 | HNB | To evaluate the potential of HNB, in the second trimester of pregnancy, as a marker of fetal facial dysmorphism, associated with pathogenic CNVs. | HNB is a marker of facial dysmorphism in many genetic syndromes. |
| Shi et al.18 | 197 | HNB | To evaluate the efficiency of CMA in the prenatal diagnosis of fetuses with isolated HNB in the first and second trimesters. | CMA can increase the diagnostic yield of chromosome abnormalities, especially pathogenic CNVs for fetuses with isolated HNB. CMA should be recommended when isolated absent nasal bone or HNB is suspected antenatally. |
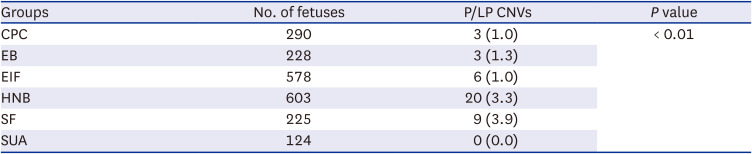
Among the 2,048 cases in the current study, 41 pathogenic/likely pathogenic CNVs (2.0%) were found in fetuses with isolated ultrasonographic soft markers during the second trimester and a normal karyotype. Table 2 shows the number of fetuses with isolated ultrasonographic soft markers and the prevalence of pathogenic or likely pathogenic CNVs according to each ultrasonographic soft marker. The frequency of pathogenic or likely pathogenic CNVs in fetuses with SF was the highest among all ultrasonographic soft markers, reaching 3.9%, followed by HNB (3.3%), EB (1.3%), CPC (1.0%), and EIF (1.0%). UTD was also included as a soft marker in the second trimester but we could not find any eligible studies dealing with UTD. A total of 124 fetuses had isolated SUA, there were no cases with pathologic CNV; thus, SUA showed the lowest frequency of CNVs among ultrasonographic soft markers.
Table 2
The findings of chromosomal microarray analysis with ultrasonographic soft markers
| Groups | No. of fetuses | P/LP CNVs | P value |
|---|---|---|---|
| CPC | 290 | 3 (1.0) | < 0.01 |
| EB | 228 | 3 (1.3) | |
| EIF | 578 | 6 (1.0) | |
| HNB | 603 | 20 (3.3) | |
| SF | 225 | 9 (3.9) | |
| SUA | 124 | 0 (0.0) |
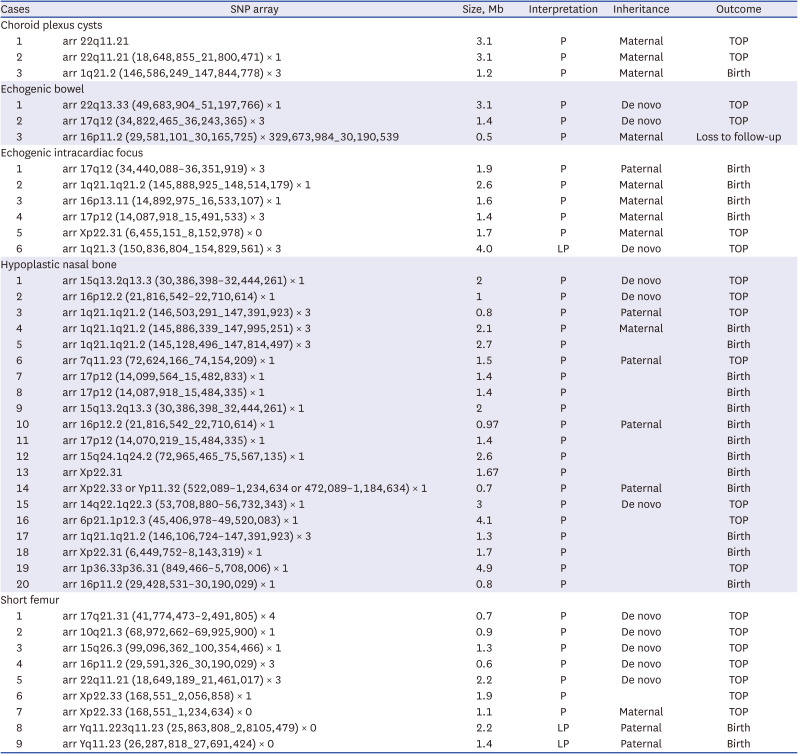
We reviewed the abnormal CMA findings in detail for each fetus with pathogenic or likely pathogenic CNVs. Three out of 290 fetuses with isolated CPC had abnormal (pathogenic or likely pathogenic) CMA findings, and the detailed CMA results were available in all three cases. Three pathogenic CNVs ranged from 1.2 to 3.1 Mb in size (Table 3). The abnormal CMA results of fetuses with other ultrasonographic soft markers are also summarized in Table 3. Three of 228 fetuses with isolated EB had pathogenic CMA findings (0.5–3.1 Mb in size). Of the 578 fetuses with isolated EIF, five had pathogenic and one had likely pathogenic CMA findings, ranging from 1.4 to 4.0 Mb in size. Of 603 fetuses with isolated HNB, 20 had abnormal CMA findings and their SNP (0.8–4.9 Mb in size).
Table 3
Summary of prenatal clinical assessments, pathogenic or likely pathogenic SNP results in each soft marker
DISCUSSION
This article focused on the prevalence of pathogenic or likely pathogenic CNVs in fetuses with ultrasonographic soft markers and a normal karyotype. The prevalence of chromosomal aberrations was 2.0%, with the highest rate of abnormal (pathogenic or likely pathogenic) CNVs in fetuses with isolated SF, followed by isolated HNB and EB.
The ACOG published guidelines regarding screening strategies for fetal chromosomal abnormalities and proposed clinical management strategies based on specific ultrasound findings.6 In clinical situations, if a soft marker is identified on fetal anatomic ultrasonography, aneuploidy screening should be offered to pregnant women who have not previously received screening. If screening has been performed, and the risk of aneuploidy is low, they suggest that no further risk assessment is needed.6
The SMFM also published guidelines on the evaluation and management of isolated soft ultrasound markers. They proposed that if an isolated ultrasonographic soft marker is confirmed on a detailed obstetrical ultrasound examination, the need for subsequent evaluation and counseling would depend on previous aneuploidy screening results, additional risk factors for aneuploidy (e.g., such as age or family history), and the concomitant presence of non-aneuploid conditions (e.g., viral infection). However, the SMFM guidelines do not recommend diagnostic testing for aneuploidy solely for the evaluation of isolated ultrasonographic soft markers following a negative serum result.2
In the current study, the prevalence of CNVs in fetuses with isolated ultrasonographic soft markers and a normal karyotype was about 0.7–6.0%. Some pathogenic CNVs have been reported in previous studies, and the specific phenotypes of those pathogenic CNVs have also been established. CNVs at 16p11.2 are frequently found in EB, EIF, and SF. In the current study, maternally inherited 16p11.2 microduplication was detected in three fetuses. This microduplication is associated with an increased risk for neurobehavioral disorders, such as intellectual disability, attention deficit hyperactivity disorder, autism and schizophrenia.192021 In addition, the prevalence of seizures and abnormal brain imaging is higher among probands with the 16p11.2 duplication than in the general population.17 A large meta-analysis by Chan et al.19 concluded that this variant is rare in the general population (0.025%), and the estimated penetrance of this CNV is 10–20% among probands with the 16p11.2 duplication.23
Another pathogenic CNV is 15q13. In our study, various pathogenic CNVs were identified in fetuses with isolated HNB, including 15q13 microdeletion, which mainly manifests as developmental delay, epilepsy, finger and toe anomalies, and minor facial abnormalities.24 In this study, however, only nasal bone hypoplasia was detected on ultrasonography in the fetus with 15q13 microdeletion.
A relationship between 16p12 and development abnormalities was also reported in previous studies. A susceptibility locus of neurocognitive impairment is known to exist in the region of 16p12 microdeletions, which have an estimated prevalence of less than 1% in normal populations.25 Patients with 16p12 microdeletions have various clinical manifestations, which mainly include developmental delay, mild intellectual disturbance, and epilepsy, despite HNB being the only ultrasonographic finding.26 Even when it comes to duplications in gene regions of similar domains overall, we were able to observe different patterns of inheritance depending on the type of soft markers.
To our knowledge, the current study is the first systematic review to meta-analyze the risk of CNVs in fetuses with isolated ultrasonographic soft markers. Our study reviewed a large dataset drawn from all previous papers, which enabled us to evaluate seven types of ultrasonographic soft markers, and investigated the frequency of chromosomal aberrations co-occurring with each ultrasonographic soft marker. Only fetuses with previously confirmed normal karyotyping were included in our study; therefore, we could focus on the clinical significance of CMA.
A limitation of our study Is that some ultrasonographic soft markers could not be found in our database search. For instance, we tried to evaluate the risk of CNVs in UTD, but no relevant studies were available in the literature. Invasive testing is not currently recommended in cases with isolated UTD, and the current study included fetuses that underwent invasive testing. Even though the actual indication for invasive testing was not available in the 7 studies, selection bias could be present in the current study, because it analyzed pregnant women who decided to undergo invasive testing despite the current guidelines.
The decision of whether to perform prenatal invasive testing is based on the risk of invasive testing and the likelihood of abnormal findings. Therefore, accurate information about the risk of chromosomal abnormalities should be available in the decision-making process. The current study provides evidence regarding the risk of chromosomal abnormalities in fetuses with normal karyotyping and isolated ultrasonographic soft markers.
In conclusion, current guidelines do not recommend diagnostic testing for aneuploidy solely for the evaluation of isolated ultrasonographic soft markers following a negative serum result. However, CMA could aid in the risk assessment and pregnancy counseling for mothers with fetuses that have isolated ultrasonographic soft markers along with normal karyotyping results.
 XML Download
XML Download