

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
More than 760 million coronavirus disease 2019 (COVID-19) cases have been reported globally during the pandemic.1 COVID-19 has a diverse clinical course, ranging from asymptomatic to severe pneumonia. However, acute respiratory distress syndrome (ARDS) is the most life-threatening complication.2 It requires care in the intensive care unit (ICU), invasive mechanical ventilation, and extracorporeal membrane oxygenation (ECMO), and shortages of these critical care resources during the pandemic posed huge challenges.3 The World Health Organization declared the end of the COVID-19 pandemic after a staggering 7 million deaths.4 Nevertheless, COVID-19 may evolve into an epidemic seasonal disease such as influenza and cause repeated outbreaks.5 Furthermore, considering the H1N1 influenza and COVID-19 pandemics of 2009, the emergence of future pandemics caused by new viruses cannot be ruled out. Reviewing the management of patients with COVID-19 with respiratory failure will help prepare for future pandemics.
Venovenous (VV) ECMO, the last option for patients with severe ARDS, facilitates gas exchange in refractory hypoxemia or hypercapnic respiratory failure settings.6 VV ECMO is recommended when invasive mechanical ventilation fails in experienced centers.78 In two randomized controlled trials involving patients with ARDS, ECMO was implemented in specialized ECMO centers.910 However, in Korea, there are no nationally established ECMO centers. As reported in a previous multicenter study, only 2 of 16 hospitals were high-volume ECMO centers, and 8 centers experienced < 20 cases per year.11 In these hospitals, ECMO was performed for patients with severe respiratory failure during the COVID-19 pandemic. In Israel, which does not operate specialized ECMO centers, a study reported a mortality rate of 54% among COVID-19 patients who received ECMO.12 Therefore, we aimed to determine the mortality rates of patients with severe COVID-19 who received ECMO and analyze the associated factors using nationwide data.
METHODS
Study design and population
This was a secondary analysis of a nationwide, multicenter, retrospective, observational cohort study involving patients with COVID-19 from January 1, 2020 to August 31, 2021. We sourced the data from a registry created by 22 tertiary- or university-affiliated hospitals in the Republic of Korea, all of which participated in this study. In brief, the registry included patients aged ≥ 19 years who tested positive for COVID-19 in a polymerase chain reaction test and were admitted to the ICU. These patients received high-flow nasal cannula oxygen therapy, invasive mechanical ventilation, prone positioning, or ECMO. We analyzed patients who were supported by ECMO for acute respiratory failure due to COVID-19 from 19 hospitals. Patient registration protocols excluded patients under 18 years of age who were not hospitalized in the ICU, did not receive oxygen therapy, or received only low-flow oxygen therapy.
Data collection and definitions
The following data were collected by trained coordinators at each center: 1) demographic data, including age, sex, body mass index, comorbidities, clinical frailty scale, and sequential organ failure assessment (SOFA) score; 2) physiological and laboratory measurements at the time of ECMO insertion, including arterial blood gas analysis; 3) ICU admission treatment and information on the use of rescue therapies, including remdesivir, corticosteroids, tocilizumab, inhaled nitric oxide, vasopressors, and continuous renal replacement therapy (CRRT); and 4) clinical outcomes, such as in-hospital death, length of in-hospital and ICU stays, ECMO duration, ECMO-free days (EFDs) on day 28, ECMO weaning, and hospital-acquired pneumonia.
The index date was considered the date of ECMO initiation, and the primary outcome was the 90-day mortality after ECMO initiation. We defined a high-volume center as a hospital handling more than 30 ECMO cases per year.13 EFDs were defined as follows: EFDs = 0 if the subject dies within 28 days of ECMO; EFDs = 28 − x if successfully weaned from ECMO x days after initiation; and EFDs = 0 if the subject receives ECMO for > 28 days.14 The attending physicians at each center made decisions regarding the initiation and weaning of ECMO.
Statistical analysis
Categorical variables are presented as the number (percentage), whereas continuous variables are presented as the median (interquartile range; IQR). Categorical variables were compared by chi-square test or Fisher’s exact test, whereas continuous variables were compared by Student’s t-test or Mann–Whitney U test, when applicable. We conducted univariate and multivariate logistic regression analyses to identify risk factors for 90-day mortality. Variables with P < 0.1 in univariate analysis and clinically relevant variables were included in the multivariate logistic regression model. Multivariate regression analysis was adjusted for age, sex, presence of comorbidities, clinical frailty scale, SOFA score, tocilizumab use, receipt of CRRT, prone positioning before ECMO, and pre-ECMO lactate level. We reported the odds ratio (OR) for each variable with the 95% confidence interval (CI). In addition, we performed Kaplan–Meier (KM) curve analysis for the 90-day survival and compared the KM curves between groups by log-rank test. Statistical analyses were performed using the Statistical Package for the Social Sciences (version 26.0; IBM Corporation, Armonk, NY, USA), and statistical significance was set at P < 0.05.
Ethics statement
All procedures were performed in accordance with the Declaration of Helsinki. This study was reviewed and approved by the Institutional Review Board and Ethics Committee of Chung-Ang University Hospital (approval number 2112-025-19397) and the local committees of all other participating centers. The need for informed consent was waived owing to the retrospective nature of this study.
RESULTS
Baseline characteristics
During the study period, of 1,114 patients who received high-flow nasal cannula oxygen therapy, 620 patients required mechanical ventilation. Of these patients, 127 of them received ECMO and were included in the final analysis. Of 19 hospitals, 13 of them were high-volume centers. Initially, there were 106 patients with VV ECMO, 14 patients with venoarterial ECMO, and 7 patients with hybrid cannulation modes. Among them, 57 patients (44.9%) survived 90 days after ECMO initiation.
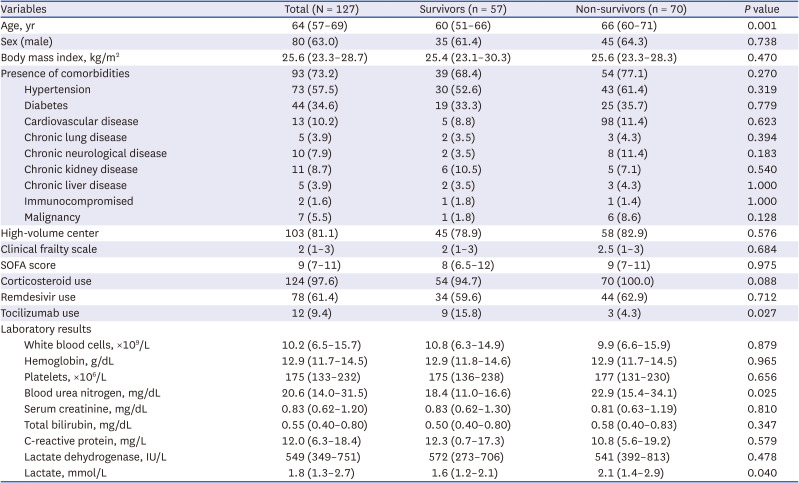
Table 1 shows the baseline characteristics of patients who received ECMO. There were no significant differences in comorbidities, clinical frailty scale, or SOFA score between survivors and non-survivors; however, survivors were younger than non-survivors (60 [51–66] vs. 66 [60–71] years, P = 0.001). Tocilizumab use was lower among non-survivors (15.8% vs. 4.3%, P = 0.027). Corticosteroid use was higher among non-survivors than among survivors; however, the result was not statistically significant (94.7% vs. 100%, P = 0.088). Based on laboratory findings at ECMO initiation, lactate level was higher among non-survivors than among survivors (1.6 mmol/L [1.2–2.1] vs. 2.1 mmol/L [1.4–2.9], P = 0.040).
Table 1
Baseline characteristics of patients who received ECMO
ICU management and clinical outcomes
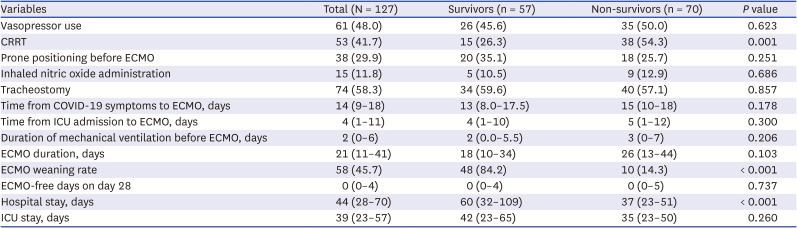
We observed no significant differences between the two groups in prone positioning before ECMO (35.1% vs. 25.7%, P = 0.251), inhaled nitric oxide administration (10.5% vs. 12.9%, P = 0.686), or tracheostomy (42.1% vs. 41.4%, P = 1.000) (Table 2). Additionally, there was no significant difference between the groups in the duration of mechanical ventilation before ECMO (2 days [0.0–5.5] vs. 3 days [0–7], P = 0.206) and ECMO duration (18 days [10–34] vs. 26 days [13–44], P = 0.103). However, the non-survivors were more likely to receive CRRT (26.3% vs. 54.3%, P < 0.001), and their weaning rate from ECMO was lower than that of survivors (84.2% vs. 14.3%, P < 0.001).
Table 2
ICU management and clinical outcomes
Factors associated with 90-day mortality
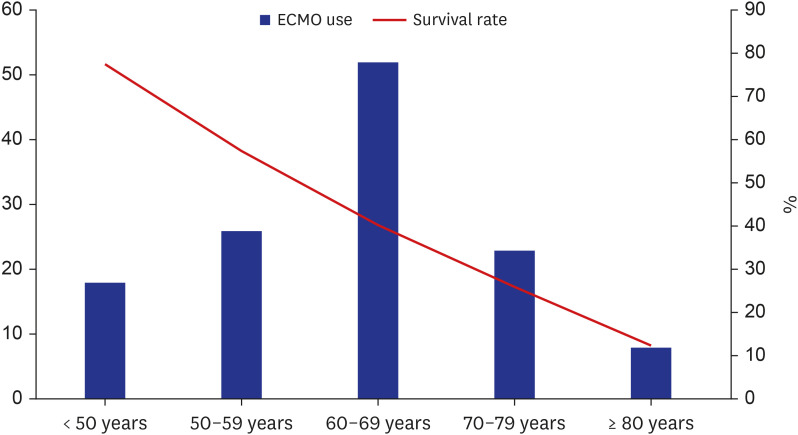
Fig. 1 shows the distribution of ECMO incidence and survival rate at 90 days according to the age group. The incidence of ECMO was increased with age but was decreased after 70 years of age. However, the survival rate was decreased linearly with age.
Fig. 1
ECMO use and survival rate at 90 days according to the age group.
ECMO = extracorporeal membrane oxygenation.
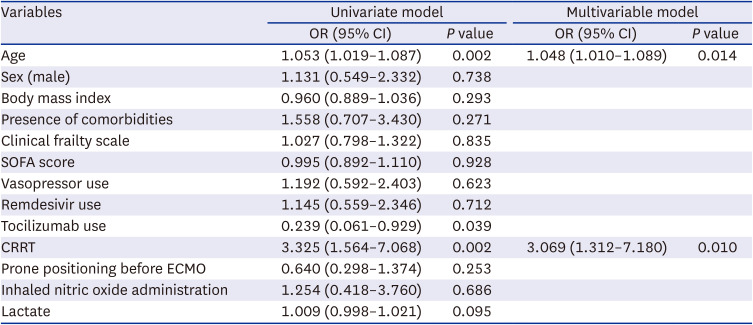
To evaluate the clinical factors associated with 90-day mortality, we performed univariate analysis using the clinical characteristics of patients who received ECMO (Table 3). Age (OR, 1.053; 95% CI, 1.019–1.087; P = 0.002), tocilizumab use (OR, 0.239; 95% CI, 0.061–0.929; P = 0.039), and receipt of CRRT (OR, 3.325; 95% CI, 1.564–7.068; P = 0.002) were associated with an increased mortality risk. In multivariate analysis, age (OR, 1.048; 95% CI, 1.010–1.089; P = 0.014), and receipt of CRRT (OR, 3.069; 95% CI, 1.312–7.180; P = 0.010) were also associated with an increased mortality risk.
Table 3
Univariate and multivariate logistic regression for 90-day mortality
Survival probability stratified according to the age group
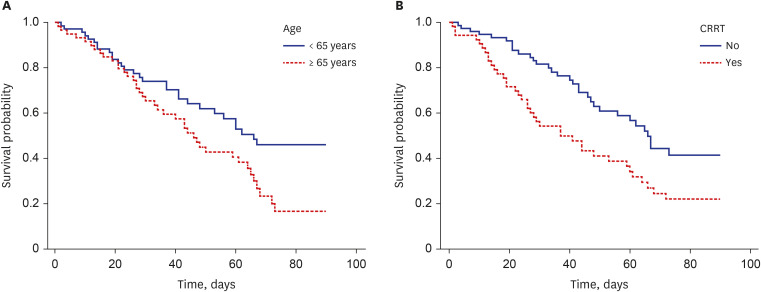
KM curves showed significant differences in survival between groups according to age (65 years) (log-rank P = 0.021) and receipt of CRRT (log-rank P = 0.004), which were associated with decreased survival rates (Fig. 2).
Fig. 2
Kaplan–Meier survival curves according to (A) age (65 years) (log-rank P = 0.021) and (B) receipt of CRRT (log-rank P = 0.004).
CRRT = continuous renal replacement therapy.
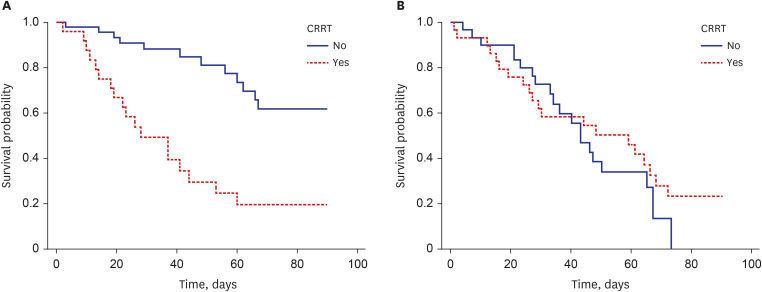
We performed subgroup analysis by classifying patients into two age groups (< 65 years and ≥ 65 years) (Fig. 3). Among patients aged < 65 years, receipt of CRRT was associated with increased mortality (P < 0.001); however, among patients aged ≥ 65 years, mortality was not affected by receipt of CRRT (P = 0.504).
DISCUSSION
In this multicenter cohort study, we found that patients with COVID-19 who received ECMO in Korea had a 55% mortality rate during the COVID-19 pandemic. Furthermore, age ≥ 65 years and receipt of CRRT were associated with an increased mortality risk. The survival rate was decreased linearly with age, particularly after 70 years of age. Receipt of CRRT was associated with increased mortality among patients aged < 65 years but not those aged ≥ 65 years.
Several meta-analyses on the mortality of patients with COVID-19 receiving ECMO have found a pooled mortality rate ranging from 37.1% to 48.8% in this population.15161718 These mortality rates are comparable to those of patients with influenza requiring ECMO.1920 This finding indicates that the ECMO mortality rate of COVID-19 is not higher than that of respiratory failure before the pandemic.21 However, the mortality rates of patients receiving ECMO can vary depending on the period or region during the pandemic. Ling et al.16 reported that mortality was increased in the late rather than early phase of the pandemic. Furthermore, although not reaching the threshold for statistical significance, mortality rates from studies in North America tended to be lower than those in the Asia-Pacific region (41.2% vs. 58.6%, P = 0.096).16
In a meta-analysis of venoarterial ECMO for patients with septic shock, the survival rate in Asia was reported to be lower than that in Europe and North America (19.5% vs. 57.8%, P < 0.001).22 Therefore, the prognosis of patients receiving ECMO may differ between regions. In a population-based cohort study in Korea, the 60-day mortality rate of the respiratory group that received ECMO was 61.3% before the COVID-19 pandemic.23 A multicenter cohort study of ECMO for acute respiratory failure also showed that the in-hospital mortality rate was 61.2% but was gradually decreased over time.11 Despite the shortage of resources during the pandemic, the mortality rate of patients receiving ECMO in Korea was decreased to 55%. Nevertheless, further improvements are required.
Age is one of the important risk factors consistently reported for patients with COVID-19 who received ECMO.1516171824252627 As shown in our study, the mortality rate of patients aged ≥ 65 years was considerably high regardless of receipt of CRRT. A meta-analysis by Tran et al.18 showed that older patients had a 2.3 times higher risk of mortality compared with that of younger patients. However, the cut-off age defined in the included studies ranged from 55 to 70 years.24272829 The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score has conventionally been used to predict survival after ECMO. In terms of age, the worst score has been given to patients aged ≥ 60 years.30 However, the predictive ability of the RESP score for patients with COVID-19 receiving ECMO remains poor.31
The demand for ECMO in the older population has increased as respiratory failure is a common occurrence in this population due to COVID-19. Furthermore, ECMO may be initiated in an isolated environment without sufficient deliberation on end-of-life care decision-making with patients and their surrogates. Interim guidelines for ECMO for patients with COVID-19 have suggested that an age of 65 years is a relative contraindication for patient selection.32 Supady et al.33 reported that age > 70 years was a major risk factor for mortality among patients receiving VV ECMO. ECMO initiation may be futile if the reference age for contraindication is unclear. Therefore, in the context of the pandemic, specific age-related recommendations for ECMO are required.
Up to 70% of patients with COVID-19 receiving ECMO support require CRRT.34 We found that CRRT was required by 42% of patients with COVID-19 receiving ECMO and was associated with a mortality rate as high as 72%. Consistent with our study, acute kidney injury and the need for CRRT have been previously reported as independent risk factors for patients with COVID-19 requiring ECMO support.1727 Possible mechanisms of renal injury include the direct cytotoxic effects of severe acute respiratory syndrome coronavirus-2 on the renal epithelium35 and endothelial dysfunction caused by a cytokine storm.36 Cytokine storms play a protective role in viral spread but can result in tissue damage, multiorgan failure, and even death.36
This study has some limitations. First, as this was a secondary analysis of a retrospective cohort study, there were some missing variables, including the RESP score, arterial blood gas analysis, and ventilatory parameters at ECMO initiation. Therefore, risk factors such as higher driving pressure were not reflected in the logistic regression model. Second, although the EOLIA trial has reported the indication criteria for ECMO,10 the initiation of ECMO was eventually determined by the ICU physicians at each hospital. Furthermore, patient mortality may differ depending on the experience of ECMO performed in each hospital. However, this study analyzed real-world data on the mortality of patients who received ECMO in a non-centralized setting during the COVID-19 pandemic. Therefore, the findings of our study may facilitate the allocation of ECMO resources in settings such as low-volume ECMO centers and non-nationally established ECMO centers in future pandemics.
During the COVID-19 pandemic, the mortality rate of patients with COVID-19 who received ECMO was high in Korea. We identified that older age (≥ 65 years) and receipt of CRRT were associated with an increased risk of mortality in this population. For efficient utilization of ICU resources, ECMO should be applied cautiously in patients with respiratory failure, accounting for their age and renal insufficiency.
 XML Download
XML Download