

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The incidence of death certificate (DC) errors has been widely reported in previous studies.12345678910111213141516171819 It is not difficult to estimate the cause of death (COD) if a patient dies from a cause related to their previous medical history. However, in the case of death in an emergency department (ED), it is often difficult to estimate the COD if the patient’s medical history is not sufficiently known or if the COD is unrelated to their medical history. Therefore, the likelihood of DC errors may be higher.5615161720
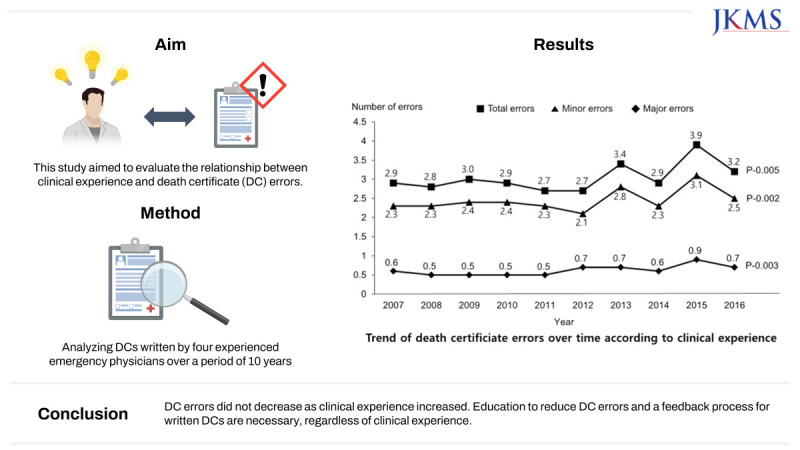
Although it is generally known that more DC errors are made by less-experienced medical doctors than experienced ones,21 no studies exist on whether the clinical experience of clinicians is related to reductions in DC errors over time. Therefore, this study aimed to evaluate whether more clinical experience leads to fewer DC errors by analyzing DC errors made by experienced emergency physicians (EPs) with over 10 years of experience working in an ED.
METHODS
Study design
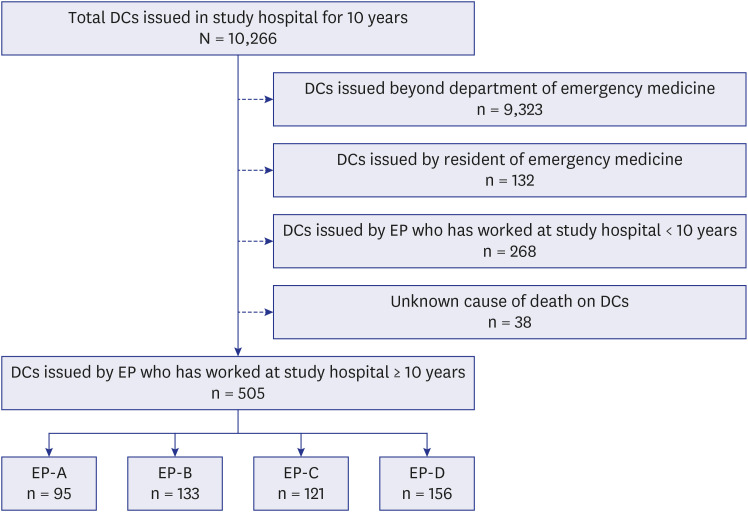
This was a pilot study in one training hospital to discover changes in DC errors over time according to the clinical experience of a select number of clinicians. DCs issued in the ED of a university hospital located in the southeast coastal area of the Republic of Korea for 10 years from 2007 to 2016 were retrospectively analyzed. DCs written by EPs who worked in the ED of the same hospital for 10 years were included to identify changes in DC errors by individual clinicians. Four EPs were included in the analysis (EP-A, EP-B, EP-C, and EP-D). DC and postmortem examination certificates can be issued at the ED in the Republic of Korea. However, postmortem examination certificates have a high possibility of unknown CODs. Therefore, only DCs were included in this study. Any DCs issued by EPs who worked for only some of the study period and by departments other than emergency medicine were excluded from the analysis. DCs for any cases where the COD was unknown were excluded from the analysis (Fig. 1).
Study setting and population
An experienced EP was defined as a medical doctor qualified as a board-certified EP after completing a six-year medical school course, a one-year internship, and a four-year residency, which is the standard for emergency medicine training in the Republic of Korea. In 2017, the study hospital introduced a method that applied the Korean Standard Classification of Diseases (KCD), corresponding to the International Classification of Diseases, 10th edition (ICD-10) codes, to CODs for DCs, and quality control for DC errors began with one EP completing DC writing training. Therefore, the study period was limited to 2016. An EP’s clinical experience in the ED was defined as the number of years of work experience in the ED after obtaining a board-certified EP qualification, which ranged from two to 10 years in 2007. The time elapsed for the study subjects after obtaining a medical doctor’s license was seven to 20 years in 2007.
Study outcomes
The primary outcome was a change in errors in DCs that were written over the decade from 2007 to 2016.
Data sources and measurement
DC errors were divided into major and minor errors based on previous literature.123456891011121314151617182223 Major errors were defined as errors that could affect COD determination, and other errors were defined as minor errors. The detailed classification and examples of errors are shown in Tables 1 and 2.
Table 1
Definitions of major death certificate errors
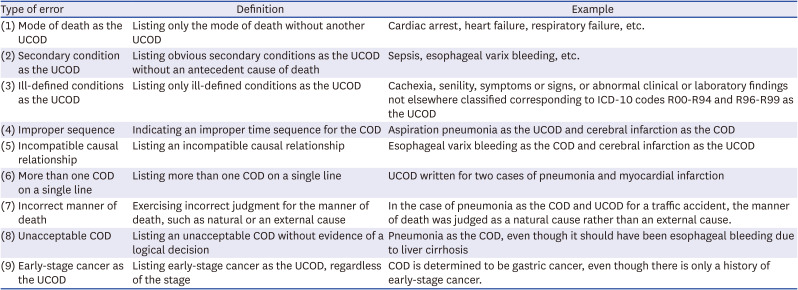
Table 2
Definitions of minor death certificate errors

The evaluation of DC errors was conducted by four EPs working at the ED of the study hospital by referring to electronic medical records and DCs. The primary evaluators (the four EPs) included three fourth-year and one third-year emergency medicine resident. Three of the EPs with previous experience in research related to DC errors conducted the first evaluation by dividing the study periods between them, and one EP conducted the first evaluation of all DCs during the entire study period. A second evaluation was conducted for cases where there was a difference in the judgment of errors between the evaluators in each first evaluation. In the second evaluation, which included the participation of an additional EP with previous experience in conducting studies related to DC errors, the final errors were judged after discussion among the five EPs.610161722 All evaluators who participated in the judgment of errors received guidelines for DC writing training and made judgments with sufficient knowledge.24252627
The patient’s gender, age, number of CODs listed on the DC, the manner of death, and detailed COD classification on the DC were also collected. The manner of death was divided into natural causes and external causes. The detailed COD classification included certain infectious and parasitic diseases, malignant neoplasms, endocrine-nutritive and metabolic diseases, circulatory diseases, neurological diseases, digestive diseases, respiratory diseases, genitourinary diseases, external causes, and others according to COD statistics classified by the Korea National Statistical Office.28 The existence of one or more major or minor errors in the DC was identified, and each major and minor error item was investigated. The three most common major errors in the DCs were investigated by dividing the study period into two halves: the first five years and the second five years.
RESULTS
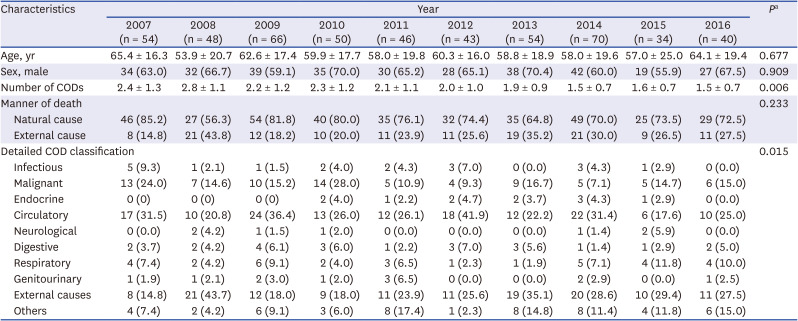
A total of 505 DCs were analyzed, with an average of 34 to 70 per study year. The number of DCs analyzed by the issuer was 95 for EP-A, 133 for EP-B, 121 for EP-C, and 156 for EP-D (Fig. 1). No significant difference was observed over time for the age and gender of the deceased on the DC, and the number of CODs written in the DC was 2.4 in 2007, 2.8 in 2008, 1.6 in 2015, and 1.5 in 2016, showing a tendency to write fewer CODs over the years (P = 0.006). There was no tendency to change the manner of death over time (Table 3).
Table 3
General characteristics of death certificates issued by four EPs over a 10-year period
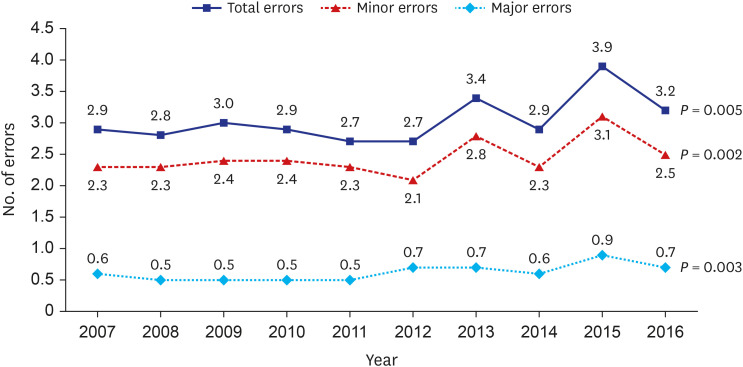
The total number of DC errors was averaged, including all major errors and minor errors in each DC. The total number of DC errors tended to increase from 2.9 in 2007 and 2.8 in 2008 to 3.9 in 2015 to 3.2 in 2016 (P = 0.005). The sum of the major errors tended to increase from 0.6 in 2007 and 0.5 in 2008 to 0.9 in 2015 and 0.7 in 2016 (P = 0.003). The sum of the minor errors increased from 2.3 in both 2007 and 2008 to 3.1 in 2015 and 2.5 in 2016 (P = 0.002) (Fig. 2).
Fig. 2
Trend of errors on death certificates issued by four emergency physicians over a 10-year period.
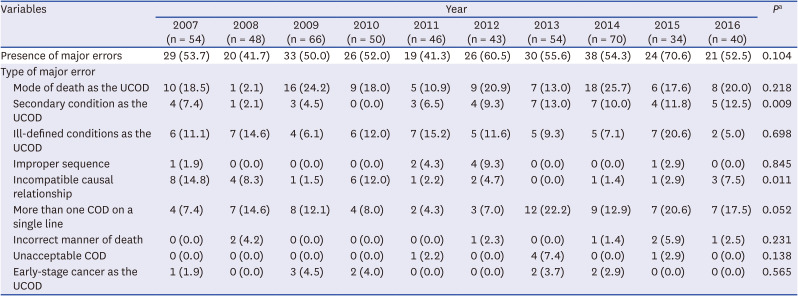
The presentation of major DC errors did not show a tendency to change over time, but in the major errors detailed analysis, secondary conditions as the underlying COD (UCOD) tended to increase, and incompatible causal relationships between CODs tended to decrease. The mode of death as the UCOD and more than one COD on a single line were common major DC errors. However, those major errors did not show a tendency to change overtime (Table 4).
Table 4
Major errors in death certificates issued by four emergency physicians over a 10-year period
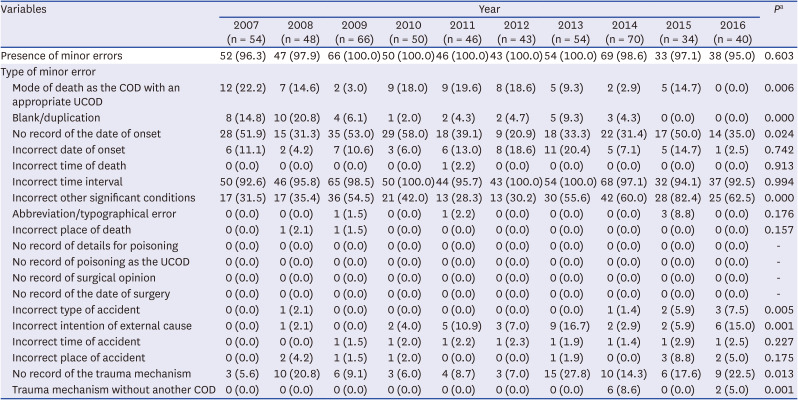
The presentation of minor DC errors did not show a tendency to change over time. In the detailed analysis of minor DC errors, the number of incorrect other significant conditions, incorrect type of accident, incorrect intention of the external cause, no record of the trauma mechanism, and record of the trauma mechanism without another COD tended to increase. However, among the minor errors, the mode of death as the COD with an appropriate UCOD, blank/duplication, and no record for the date of onset tended to decrease. An incorrect time interval was the most common minor DC error, but this minor error did not show a tendency to change over time (Table 5).
Table 5
Minor errors in death certificates issued by four emergency physicians over a 10-year period
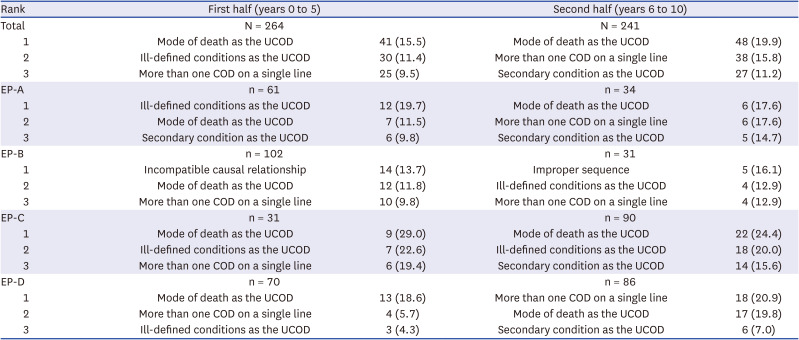
The three most common major errors on DCs during the first half of the study period were in the order of the mode of death as the UCOD, ill-defined condition as the UCOD, and more than one cause of death on a single line. For the second half of the study period, the order was the mode of death as the UCOD, more than one cause of death on a single line, and a secondary condition as the UCOD. The mode of death as the UCOD was the most common major error by EP-C in both the first and second half of the study period. The most common major error in the first half of the study by EP-A was an ill-defined condition as the UCOD, incompatible causal relationship by EP-B, and mode of death as the UCOD by EP-D. For the second half of the study, the major errors were the mode of death as the UCOD by EP-A, improper sequence by EP-B, and more than one COD on a single line by EP-D (Table 6).
Table 6
The three most common major errors on death certificates during the first and second half of the study period
DISCUSSION
National COD statistics are generated based on the COD on DCs, and major policies related to healthcare are determined based on the results.81118 Therefore, an accurate COD is an important piece of medical information that is related to major health issues on a domestic and global basis. The COD on the DC is also important for deaths requiring investigation or insurance claims, civil and criminal disputes. Any errors in the main information, which can greatly affect the COD decision in a DC, can lead to incorrect COD statistics. In this study, which examined DCs written by EPs over a 10-year period, major errors that could affect COD decisions did not decrease. Numerous studies have shown that many errors occur in DCs.123456789101112131415161718 Therefore, various efforts are required to reduce these errors, such as the application of ICD-10 codes for COD on DCs,17 and the most necessary is education for DC writers.12121418222930 Regarding cardiopulmonary resuscitation training, knowledge or skills are improved through education, and repeated education is required in addition to the initial training to acquire a high level of ability. In a similar manner, DC errors can be reduced through DC writing education. The study results indirectly showed that even the DCs of experienced clinicians contain many errors if the clinicians do not receive continuous education.
All four EPs included in the study were educated at three different medical colleges and trained in their residency at three different training hospitals. They did not receive any formal training in writing DCs when they were medical students. They all learned orally about DC writing from a senior doctor during their residency and relied on simple guidelines. In addition, regular feedback was not provided regarding errors in their DC writing. However, their total number of DC errors was similar, although the characteristics of the frequent DC errors varied. This situation may be similar for most clinicians who do not have sufficient training experience in writing DCs.
Many errors may occur when writing DCs, and the characteristics of the errors vary according to the experience of the issuer.56 In this study, the characteristics of the major errors of four DC issuers were examined. The mode of death as the UCOD was the most common among the major errors made by EP-A, EP-C, and EP-D, and more than one COD on a single line was the most common error made by EP-B. Among the major errors, the second most frequent occurrence was ill-defined conditions as the UCOD by EP-A and EP-C, mode of death as the UCOD by EP-B, and more than one COD on a single line by EP-D. The most frequent major errors were the mode of death as the UCOD, secondary conditions as the UCOD, and an unacceptable COD in a previous study.17 Another study reported that secondary conditions as the UCOD, mode of death as the UCOD, and incompatible causal relationships, in that order, were the most frequent major errors.6 Thus, neither the overall nor individual error characteristics exactly matched, and the types of errors that occurred frequently differed according to individual characteristics. Therefore, feedback or education regarding errors is required to limit the differences and improve errors according to individual characteristics.
Since this study evaluated DCs issued by EPs who worked continuously for 10 years at one study hospital, there were a limited number of EPs and DCs for analysis. In addition, during the study period, some EPs were dispatched to other institutions or worked as a dedicated EPs specializing in ED pediatrics or severe trauma. Therefore, the number of DC issuances did not remain constant from year to year. Furthermore, due to the nature of the training university hospital, there is a possibility that a resident who worked with a study subject EP may have written a DC under the guidance of the EP but differed from their opinion, so it was not included in the study. Another limitation is that the results of this study cannot be generalized because there is no previous study related to this, so an appropriate sample size could not be presented. Although the medical school and training hospital of the four EPs in this study were not all the same, and the characteristics of the frequent DC errors were different, it is meaningful that the total number of DC errors was similar between them. However, the results must be verified through further studies. It is also possible that errors existed in the DC error evaluation itself. When multiple CODs are involved, it is sometimes difficult to accurately determine only one COD. In this case, if several experts reach an agreement, the value of the decision must be respected. Therefore, in this study, three evaluators and one overall evaluator performed the first evaluation of the errors, and evaluation errors were minimized by conducting a second evaluation for cases where there was a difference in the first evaluation.
In conclusion, as a result of analyzing DCs issued by experienced EPs over a 10-year period, the study found that DC errors did not decrease as clinical experience increased. Education to reduce DC errors and a feedback process for DC writing is necessary, regardless of the writer’s amount of clinical experience. DC writing education should be included in the regular curriculum at medical schools, and regular education for DC writing is necessary after graduation. It is also worth considering a system in which the agency with the authority to issue DCs independently verifies DC errors and provides feedback to the DC issuer. Additionally, if the COD changes based on autopsy results conducted after the issuance of the DC, a system in which the DC issuer is notified may be considered. In the future, a multicenter study, in addition to a study to verify whether actual errors are reduced through education, is required.
 XML Download
XML Download