

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF), the primary cause of embolic stroke, presents a significant healthcare challenge.12 Early detection of AF is crucial for preventing severe complications such as heart failure and stroke, as well as averting cardiac structural abnormalities. Moreover, early identification of AF encourages lifestyle changes that can reduce healthcare costs and associated problems.34 However, detecting AF before clinical symptoms appear is complex due to many individuals exhibiting paroxysmal and asymptomatic characteristics.45 Furthermore, the limited effectiveness of a 12-lead electrocardiogram (ECG) in identifying transient arrhythmias and the impracticality of prolonged monitoring complicate the identification of undetected or potential AF.156
The application of artificial intelligence through deep learning algorithms can classify 12-lead ECGs by arrhythmia types and even detect undiagnosed AF.78910 This research hypothesizes the presence of subtle features of AF indicators in 12-lead ECGs during normal sinus rhythm (NSR).
Recent advances have led to the development of more practical and convenient ECG recording devices.111213 Technological progress now allows cardiac rhythm monitoring using single-lead ECG equipment, which is effective for AF diagnosis and screening.121415 It has been established that using a single-lead ECG, acquired by a mobile device, is a good alternative to Holter monitoring for diagnosing AF.161718 Unlike 12-lead ECGs, single-lead ECG recordings are more user-friendly for capturing cardiac rhythm and offer advantages in continuous, long-term ECG acquisition compared to Holter monitoring. Although deep learning algorithms could detect AF in NSR using 12-lead ECG, these ECGs are less convenient than single-lead mobile ECG devices and offer limited continuous monitoring capabilities, thus restricting ongoing AF monitoring and individual data collection. Holter monitors can be beneficial in certain cases, but they are cumbersome to wear and can disrupt daily life.19
With the advent of single-lead mobile ECG devices, both the quality and quantity of data have significantly improved. Recent studies have explored the classification of AF using deep learning techniques with single-lead ECGs.2021 However, the identification of AF remains a challenge with single-lead mobile ECG devices, primarily due to the subtle and often undetectable features of AF. Furthermore, the focus on screening rather than determining the prevalence of AF presents additional complexities.4522 Therefore, there has been limited understanding in identifying AF using single-lead mobile ECG devices.
METHODS
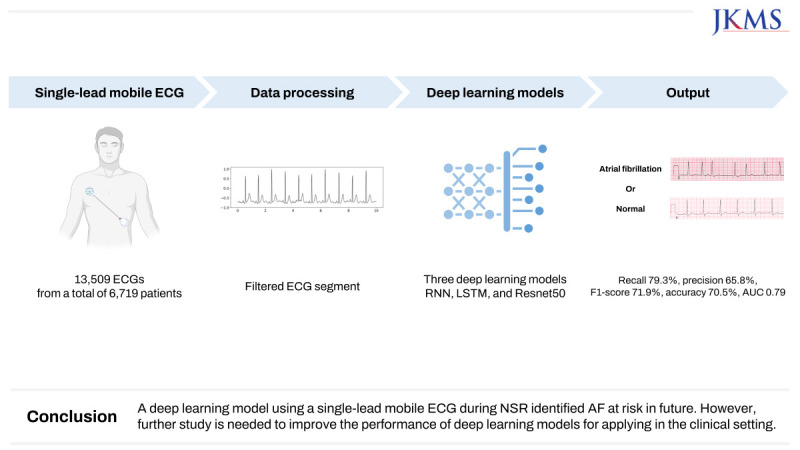
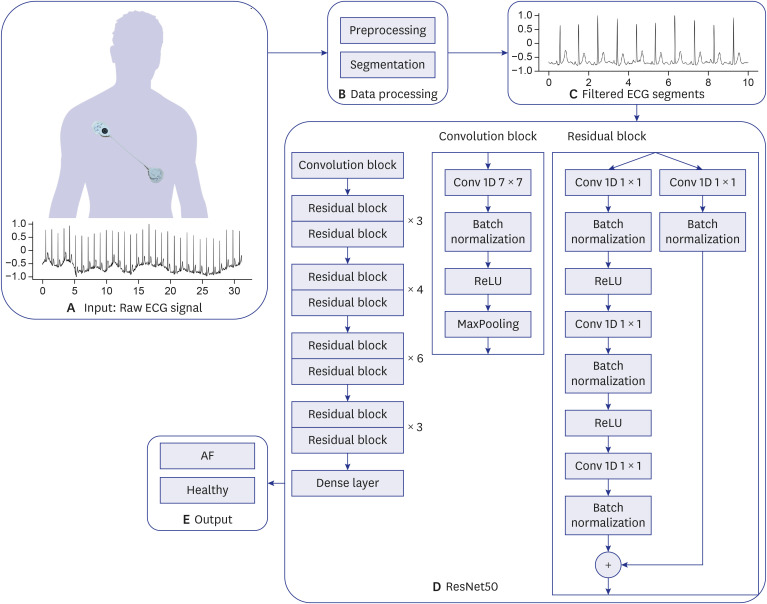
Our methodology comprises five essential components: mobile ECG datasets, preprocessing procedures, segmentation, deep learning models, and outputs (Fig. 1). We ensured the reliability of our analysis by having all mobile ECGs meticulously diagnosed and labeled by clinical experts.
Fig. 1
Proposed method for AF prediction using single-lead mobile ECG in normal sinus rhythm.
(A) Input stage with raw ECG signal. (B) Stage of data processing. (C) Segments of filtered ECG. (D) Application of ResNet50. (E) Final output stage.
ECG = electrocardiogram, AF = atrial fibrillation, ResNet = residual neural network, Conv = convolutional layer, ReLU = rectified linear unit.
Data collection
We collected mobile ECGs prospectively and consecutively from the patients who consented to the data collection and those who visited or were admitted at the Departments of Cardiology and Neurology, Chonnam National University Hospital. From July 2021 to December 2022, we acquired 13,059 mobile ECGs from 6,720 patients using the mobiCARE-MC100 device (Seers Technology, Seongnam, Korea). These ECGs had a sampling rate of 256 Hz and comprised single-lead recordings of approximately 60 seconds each.
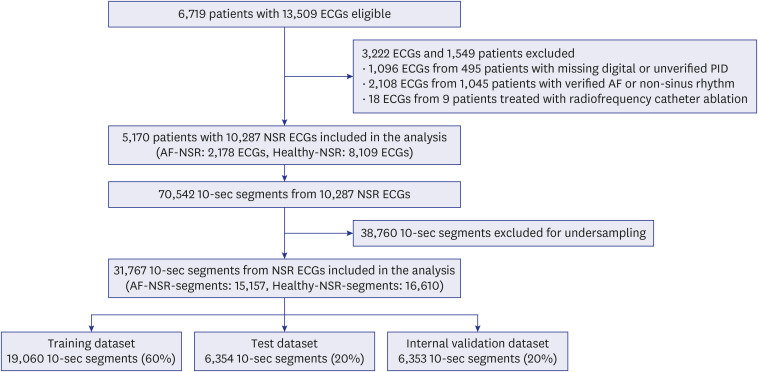
To ensure data suitability for analysis, we applied specific exclusion criteria: ECGs with AF or non-sinus rhythms, those lacking a confirmed patient identification number (PID), or containing incomplete digital information. Additionally, ECGs from patients who underwent radiofrequency catheter ablation (RFCA) for AF were excluded changes in ECG waveforms.23242526 As a result, 3,222 ECGs from 1,549 patients were excluded: 1,096 ECGs from 495 patients due to missing digital information or unverified PID, 2,108 ECGs from 1,045 patients with confirmed AF or non-sinus rhythm, and 18 ECGs from 9 patients with a history of AF RFCA (Fig. 2). We utilized 10,287 NSR ECGs from 5,170 patients for analysis. Within this subset, 2,178 NSR ECGs from 1,089 patients with an AF history were labeled “AF” and 8,109 ECG recordings from 4,081 patients were labeled “Healthy.” AF history was determined by at least one documented 12-lead ECG with AF. Notably, a history of AF without a documented 12-lead ECG was not considered as AF history. The external validation dataset comprised 160 72-hour-Holter ECGs from 160 distinct patients, using the same device.
Data preprocessing
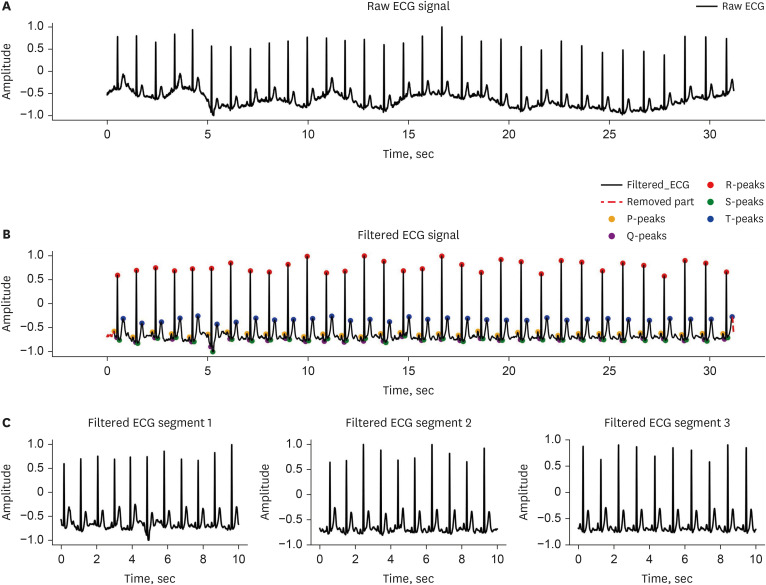
To eliminate noise, the PQRST peaks of each ECG were labeled, and segments not containing these waveforms were removed. The initial segment preceding the first P-Peak and the trailing segment following the last T-Peak were also removed. Subsequently, the ECG baseline was adjusted, and a 0.5 Hz high-pass Butterworth filter applied to further denoise the ECG waveform. ECGs were then segmented into 10-second increments to standardize ECG length across individuals (Fig. 3).
Fig. 3
Process of data preprocessing for atrial fibrillation detection in mobile ECG under normal sinus rhythm.
(A) Raw ECG signal. (B) Filtered ECG signal. (C) Filtered ECG segments.
ECG = electrocardiogram.
To counteract data imbalance and enhance the generalizability of our models while reducing bias, a random under-sampling technique2728 was employed. This involved the random exclusion of 38,760 10-second segments labeled as Healthy. The dataset was divided into training, internal validation, and testing sets, adhering to a distribution ratio of 6:2:2, respectively.
Deep learning model
Residual neural networks (ResNet) were utilized as deep learning models for identifying potential AF in NSR mobile ECGs.
ResNet, a type of convolutional neural network, demonstrates high accuracy even with deeper layers, effectively addressing the gradient vanishing and exploding problems. Additionally, it offers excellent generalization capabilities, facilitating rapid learning and convergence.2930 For comparative purposes, recurrent neural network (RNN) and long short-term memory (LSTM) models were also evaluated. RNNs are primarily employed in time series analysis,3132 whereas LSTM models address long-term dependencies inherent in RNNs.333435
Supplementary Data 1 provides detailed descriptions of RNN and LSTM models.
Model optimization and implementation
Training was conducted using the AdamW3637 optimizer, with a learning rate of 0.0001, a batch size of 32, and over 50 epochs. However, early stopping was implemented at the 12th epoch to prevent overfitting. Cross-entropy loss served as the loss function.
All mobile ECGs underwent preprocessing using Python 3.9. Pytorch 2.0.1 was utilized for model implementation, with training conducted on a computer equipped with an NVIDIA GeForce RTX3090 TI graphics processing unit (Nvidia, Santa Clara, CA, USA).
Data analysis
The performance of the model was evaluated and compared using accuracy, recall, and precision. These evaluation measures are defined as:
, where TP represents true positive, TN signifies true negative, FP is false positive, and FN stands for false negative. To provide a comprehensive assessment of model performance, the F1-score and the area under the receiver operating characteristic (ROC) curve (AUC) were calculated. The F1-score, representing the harmonic average of precision and recall, is calculated as follows:

The ROC curve plots the true positive rate (recall) against the false positive rate (1 − Specificity), varying the classification threshold. The AUC value was determined by integrating the ROC curve.
RESULTS
Data characteristics
The dataset includes a total of 31,767 segments, each 10 seconds long. Of these segments, 15,157 (47.7%) were categorized as AF and 16,610 (52.3%) as Healthy. The training set comprised 19,060 of these 10-second segments, with 9,094 labeled as AF and 9,966 as Healthy. The test set contained 6,354 segments, of which 3,031 were identified as AF and 3,322 as Healthy. Additionally, the internal validation set consisted of 6,353 segments, with 3,032 labeled as AF and 3,321 as Healthy.
Performance comparison of different models
Three deep learning models—RNN, LSTM, and one-dimensional convolutional ResNet50—were employed to analyze the dataset refined through specific exclusion criteria. The one-dimensional convolutional ResNet50 model exhibited F1-score, recall, precision, and accuracy values of 71.9%, 79.3%, 65.8%, and 70.5%, respectively, for identifying AF in the test set. In contrast, the RNN model achieved an F1-score of 59.5%, recall of 50.1%, precision of 73.1%, and accuracy of 67.4%, while the LSTM model recorded an F1-score of 62.2%, recall of 53.7%, precision of 73.8%, and accuracy of 68.8%. In the training set, ResNet50 demonstrated F1-score, recall, precision, and accuracy values of 79.3%, 77.8%, 80.8%, and 80.6%, respectively. The RNN in the training set yielded an F1-score of 66.0%, recall of 64.1%, precision of 68.0%, and accuracy of 68.5%. Furthermore, the LSTM’s performance in the training set included an F1-score of 65.5%, recall of 63.0%, precision of 68.2%, and accuracy of 68.3%. For the internal validation set, ResNet50 showed F1-score, recall, precision, and accuracy values of 69.1%, 76.2%, 63.2%, and 67.4%, respectively. The RNN in the internal validation set exhibited an F1-score of 59.6%, recall of 51.3%, precision of 71.1%, and accuracy of 66.8%. Similarly, the LSTM model in the internal validation set displayed an F1-score of 61.1%, recall of 53.2%, precision of 71.5%, and accuracy of 67.6% (Table 1).
Table 1
Performance of proposed models in predicting atrial fibrillation in mobile electrocardiogram during normal sinus rhythm
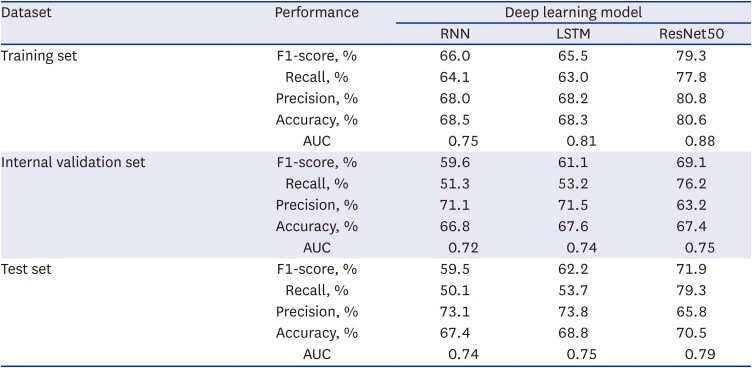
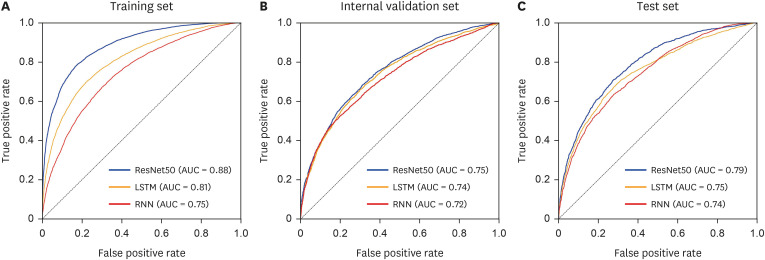
Confusion matrices were employed to visually assess and compare the classification performance of each model. Fig. 4 depict the confusion matrices for the classification results of ResNet50, RNN, and LSTM, respectively. In the context of classifying AF from NSR, ResNet50 demonstrated the highest AUC of 0.79, followed by RNN at 0.75, and LSTM at 0.74 for the test set. For the training set, the AUCs of ResNet50, RNN, and LSTM were 0.88, 0.75, and 0.81, respectively. Additionally, ResNet50, RNN, and LSTM exhibited AUCs of 0.75, 0.72, and 0.74, respectively, for the internal validation set. The ROC curves and AUC values for identifying potential AF in the training set, internal validation set, and test set are presented in Fig. 5.
Fig. 4
Performance evaluation of proposed models using confusion matrices on the test set.
(A) Confusion matrix of ResNet50, (B) Confusion matrix of RNN, (C) Confusion matrix of LSTM.
ResNet = residual neural network, RNN = recurrent neural network, LSTM = long short-term memory.
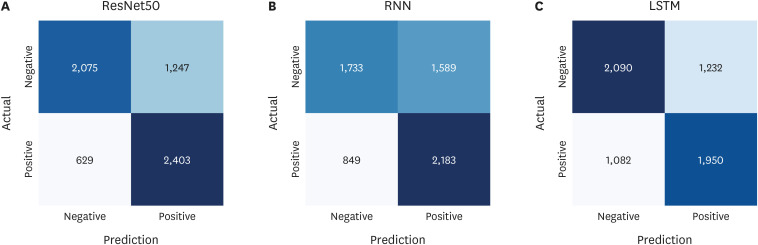
Fig. 5
ROC curves demonstrating the performance of proposed models for atrial fibrillation prediction in mobile electrocardiogram during normal sinus rhythm.
(A) ROC curve for the training set. (B) ROC curve for the internal validation set. (C) ROC curve for the test set.
ROC = receiver operating characteristic, AUC = area under the receiver operating characteristic curve, ResNet = residual neural network, LSTM = long short-term memory, RNN = recurrent neural network.
Performance on external validation set
In the external validation, we employed the same filtering approach as in the pre-existing dataset of labeled 72-hour Holter ECGs, ensuring consistency in our analysis. This process involved dividing the ECGs into 10-second segments. We then utilized random sampling without replacement to select these segments. Consequently, we extracted 3,555 (54.21%) segments labeled as Healthy and 3,003 (45.79%) segments labeled as AF. In this external set, ResNet50 demonstrated an F1-score of 64.1%, a recall of 68.9%, a precision of 60.0%, an accuracy of 63.4%, and an AUC of 0.68.
DISCUSSION
In this study, we developed and evaluated a deep learning-based algorithm for detecting potential AF in NSR using single-lead mobile ECG. The algorithm achieved an AUC of 0.79, with external validation yielding 0.68. An AUC value of 0.7 or higher from the test set is generally regarded as indicative of good performance.38 Our results were also compared with previous studies that detected AF using 12-lead ECG,910 revealing that single-lead ECG is adequate for obtaining reliable results. These outcomes indicate that potential AF can be identified in NSR ECG using only single-lead data, rather than relying on all 12-lead data.
Few studies have employed a single-lead ECG, collected using single-lead mobile ECG devices, to classify potential AF from ECG during NSR. Most prior research has focused on identifying AF using 12-lead ECG.78910 The single-lead mobile ECG device utilized in this study offers convenient body attachment and high versatility, enabling extended ECG monitoring and real-time data collection. Considering the paroxysmal nature of AF, long-term ECG monitoring is often essential for its detection.39 This study’s results validate the reliability of single-lead ECG collected with a single-lead mobile ECG device and demonstrate its potential as a convenient, highly useful method for ECG recording. Such recordings can be analyzed to identify arrhythmia occurrences, thereby allowing healthcare providers to mitigate the risk of arrhythmias and other diseases and to develop innovative patient management strategies, such as timely medication.
The study also implemented crucial steps to acquire the necessary single-lead ECG for identifying potential AF. Our data collection involved 6,720 patients, facilitating the acquisition and analysis of 13,059 mobile ECGs. A common issue in many medical datasets is the data imbalance problem, where specific health conditions are underrepresented in classification algorithms. This problem was evident in our study, particularly with the scarcity of ECGs labeled as AF. Predominantly, the data were marked as Healthy, which could hinder the detection of AF. To mitigate this data imbalance and enhance the generalization capabilities of our models while minimizing bias, a random under-sampling technique was employed. This involved randomly discarding 38,760 10-second Healthy-labeled segments, effectively addressing the data imbalance and leading to more accurate classification outcomes. For the external validation dataset, the same methodology was applied as with our training, testing, and internal validation sets. The 160 72-hour Holter ECGs from 160 distinct patients were divided into 10-second segments, and random sampling without replacement was conducted to form a representative subset for validation. This method of random sampling without replacement ensures a more unbiased analysis by avoiding potential bias from the researchers’ preferences or assumptions. Furthermore, three deep learning models—RNN, LSTM, and ResNet50—were utilized to detect potential AF in mobile ECGs during NSR, and their performances were compared. The ResNet50 model exhibited superior performance, with an F1-score, recall, precision, accuracy, and AUC of 71.9%, 79.3%, 65.8%, 70.5%, and 0.79, respectively. These results suggest that ResNet50 is more accurate in identifying the subtle patterns indicative of potential AF. The methodologies of data collection, preprocessing, and model selection are critical in determining the efficacy of a detection model. Through this approach, we demonstrated the viability of using single-lead mobile ECG and highlighted the potential of deep learning algorithms to discern subtle signals in ECGs for the detection and identification of cardiovascular events such as AF.
Further research is necessary to enhance the performance and generalizability of deep learning models for use in clinical settings. Although our model, which uses a single-lead ECG, demonstrated promising results in identifying AF with an AUC above 0.7 in the test set, its performance was less impressive in the external validation set. Previous studies have indicated that the RR interval, P-wave morphology, and QT interval are significant factors affecting AF risk.4041 Our study relied solely on ECGs to train the deep learning algorithm, but future research could improve model accuracy by incorporating additional relevant features as AF indicators.
About 30% of patients with cardiogenic stroke, specifically embolic stroke of unknown source (ESUS), exhibit AF during long-term ECG monitoring.4243 In instances of cryptogenic strokes where the cause is unclear, detecting AF is crucial; the presence of AF necessitates a shift in treatment from standard antiplatelet therapy to anticoagulation to lower the recurrence risk of strokes. Therefore, more studies focused on detecting AF in patients with ESUS are imperative. Employing our developed deep learning model in specific cohorts, such as those with ESUS, will aid in verifying its clinical utility. The data processing methods and deep learning models developed in this study are foundational for broader clinical investigations. As we continue this research and enhance our models, their significant impact on patient healthcare and cost-effectiveness will become increasingly evident in the future.
This study presents several limitations. Firstly, the constraints of a single-lead mobile ECG device compromise data quality compared to 12-lead ECGs. As a result, rhythms that were unidentified or vague were systematically excluded from the analysis, leading to a higher prevalence of exclusions and a more restrictive analysis. Secondly, the study lacks prospective validation. However, to address this limitation, ongoing studies are currently applying and validating the algorithm in acute ischemic stroke patients. These patients are undergoing serial follow-up with 72-hour Holter ECGs at three-month intervals. The primary objective of this validation is to identify AF and evaluate the algorithm’s performance.
Finally, we developed an AI model in this study for detecting potential AF using short-read ECG data from a single-lead mobile ECG device, and we validated its performance to ensure reliable results. The data and AI techniques utilized in this study have the potential to significantly enhance early identification and patient management of potential heart diseases.
 XML Download
XML Download