

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
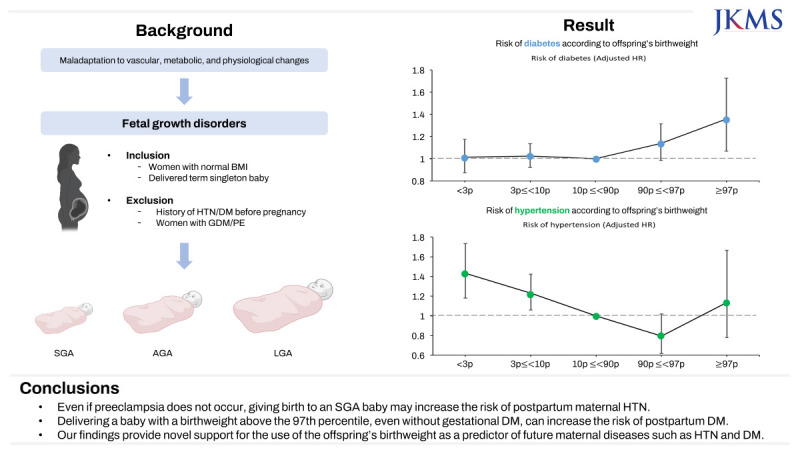
In response to the increasing demands of a rapidly growing fetus and placenta, pregnant women undergo several vascular, metabolic, and physiological changes. When these changes, including insulin resistance, adipose deposition, hypercoagulability, cardiac remodeling, and decreased vascular resistance,1 act as stressors or do not adapt well in the body of certain women, they may manifest as adverse outcomes such as fetal growth disorders. Recently, adverse pregnancy outcomes have amplified the cardiovascular and metabolic risk factors, which contribute to a higher risk of future maternal diseases.23456789
Fetal development is determined by the maternal provision of the substrate and its placental transfer.10 Insulin and insulin-like growth factors are potent stimulators of cell division and differentiation.11 Elevated cord C-peptide levels, which represent fetal hyperinsulinemia, are associated with excessive fetal weight gain.12 Similarly, high maternal free fatty acids13 and excessive placental fatty-acid metabolism14 are associated with fetal overgrowth. Thus, delivering a large-for-gestational-age (LGA) baby may indicate a pre-existing metabolic dysfunction in the mother, which later predisposes her to metabolic diseases.
Fetal growth restriction may result from placental or vascular insufficiency. Placenta-mediated fetal growth restriction occurs through chronic fetal hypoxia owing to maternal vascular malperfusion,15 chorion regression16 or uteroplacental vascular insufficiency.17 An abnormal trophoblast invasion or the remodeling of the spiral artery can be caused by immunological abnormalities18 or vascular factors, such as atrial natriuretic peptide-converting enzyme.192021 Therefore, delivering a growth-restricted baby represents a pre-existing vascular dysfunction in the mother, which later predisposes her to cardiovascular diseases.
Several studies have investigated the impact of fetal growth disorders on the future health of mothers22232425; however, previous research had limited control over covariates that could influence fetal growth,26 and few studies have assessed the effects of the frequency and severity of growth disorders. This study aims to evaluate the risk of hypertension (HTN) and diabetes mellitus (DM) according to offspring’s birthweight among women with normal body mass index (BMI) scores, who did not experience gestational DM or hypertensive disorders during pregnancy.
METHODS
Study population
The study population data were obtained from the Korean Health Insurance Review and Assessment (HIRA) service database, which comprises all claims data from the National Health Insurance Service of most (97%) of the Korean population enrolled in the single-payer healthcare system. The HIRA database provides information on beneficiaries including demographic, socioeconomic, diagnostic, procedural, and prescription data. In addition, data from the biannual National Health Screening Examination (NHSE) and National Health Screening Program for Infants and Children were used to evaluate pre-pregnancy HTN, DM, and offspring’s birthweight.
Study design
The study population included pregnant Korean women who met the following criteria: 1) gave birth to a singleton baby after 37 weeks of gestation; 2) delivered between 2015 and 2016; 3) participated in the NHSE within a year before pregnancy; 4) had pre-pregnancy blood pressure levels of < 140/90 mmHg; 5) had fasting glucose levels of < 126 mg/dL; and 6) had normal BMI scores (18.5 ≤ BMI < 23). Women with multifetal pregnancies, gestational DM, or hypertensive pregnancy disorders were excluded.
Offspring’s birthweight was classified according to the percentage of birthweight as follows: 1) a birthweight less than the 3rd percentile for gestational age (very small for gestational age [very SGA]); 2) a birthweight between the 3rd and 10th percentiles; 3) a birthweight between the 10th and 90th percentiles (average for gestational age [AGA]); 4) a birthweight between the 90th and 97th percentiles; and 5) a birthweight greater than the 97th percentile (very LGA).
Outcomes
The primary outcome was a new occurrence of HTN or DM, which was monitored postpartum. HTN was defined as any HTN diagnosed > 12 weeks postpartum, to distinguish chronic HTN from gestational HTN. DM was defined as any DM diagnosed > 6 weeks postpartum to differentiate it from gestational DM. HTN and DM were diagnosed according to the International Classification of Diseases (ICD) tenth revision.
Covariates
Other maternal characteristics associated with offspring’s birthweight and the risk of HTN or DM were identified using the NHSE database. The following maternal variables were included in the adjusted models: maternal age, parity, gestational age at delivery, fetal sex, maternal BMI scores, and a history of smoking.
Statistical analysis
Continuous variables were described as mean and standard deviation and were compared using the Student’s t test or the analysis of variance model for multiple group comparisons. Categorical variables were presented as numbers and percentages and were compared using the chi-square test. To evaluate the new occurrences of HTN or DM, a Cox proportional hazards model was used to calculate the hazard ratios (HRs) and the 95% confidence intervals (CIs). The analyses were performed using SAS for Windows (version 9.4; SAS Inc., Cary, NC, USA), and statistical significance was set at a P value of < 0.05.
RESULTS
Subject population
Of the 506,415 women enrolled in this study, 64,037 met the inclusion criteria and were analyzed. Each birthweight category comprised 3,002, 6,267, 51,138, 2,814, and 816 women, respectively (Fig. 1).
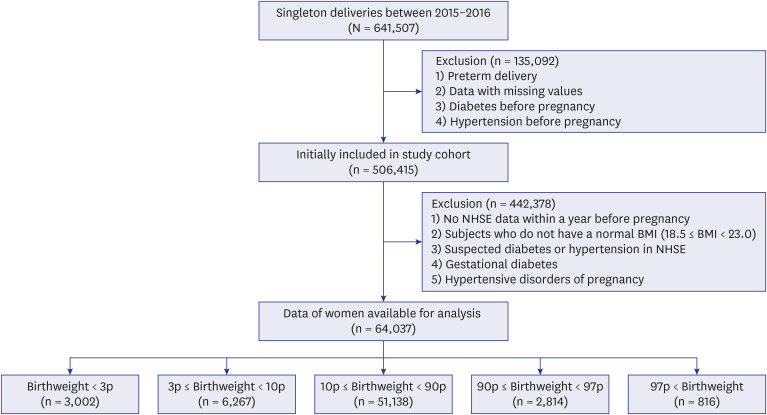
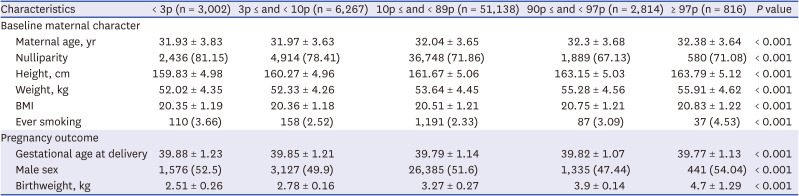
Table 1 shows the baseline characteristics of the study population. Women who delivered SGA babies were more likely to be nulliparous, had lower BMI scores, had lower fasting blood glucose levels, or had a history of smoking. Women who delivered LGA babies had higher BMI scores or a history of smoking.
Table 1
Baseline clinical features and prevalent diseases of the study population
Laboratory result before pregnancy
The physical and laboratory results obtained from the health checkups conducted within a year prior to pregnancy are presented in Table 2. Women who delivered very SGA babies had higher levels of systolic and diastolic blood pressure than those of women who delivered AGA babies. Women who delivered very LGA babies had higher fasting blood glucose levels and lower high-density lipoprotein cholesterol levels than those of women who delivered AGA babies.
Table 2
Physical and laboratory results before pregnancy

Risk of new occurrence of HTN and DM
The median follow-up duration was 5.7 years, and 1,803 women developed HTN and 3,807 developed postpartum new-onset DM. Table 3 shows the number of occurrences and the HRs of each outcome using a Cox proportional hazards regression analysis. Fig. 2 shows the adjusted HRs for HTN in women according to the offspring’s birthweight after adjusting for age, parity, BMI scores, gestational age at delivery, fetal sex, and a history of smoking. A lower birthweight was strongly associated with a maternal HTN risk (HR = 1.431; 95% CI = 1.181–1.734). No apparent association between the birthweight of an LGA offspring and the risk of maternal HTN was detected. The HRs for DM in women according to the offspring’s birthweight after adjusting for age, parity, BMI scores, gestational age at delivery, fetal sex, and a history of smoking are presented in Fig. 3 (HR = 1.358; 95% CI = 1.068–1.727).
Table 3
Incident diagnosis of outcomes

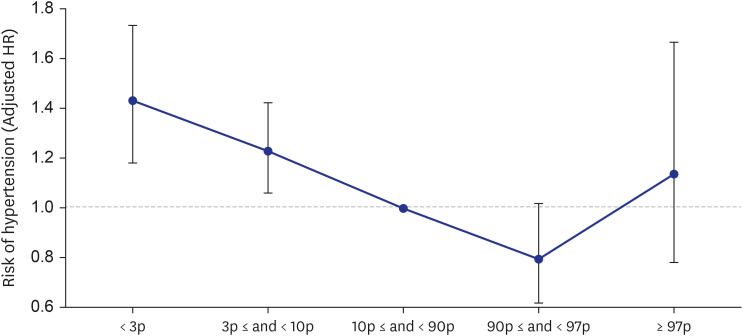
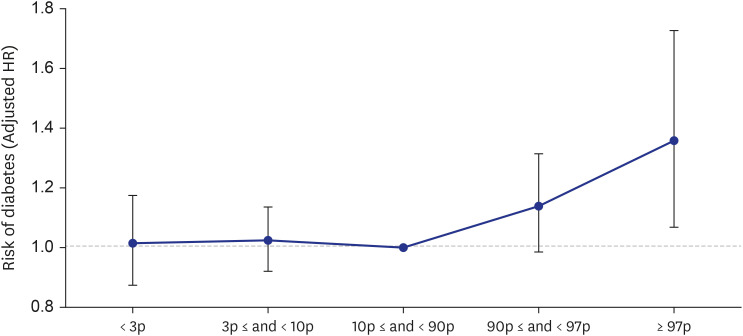
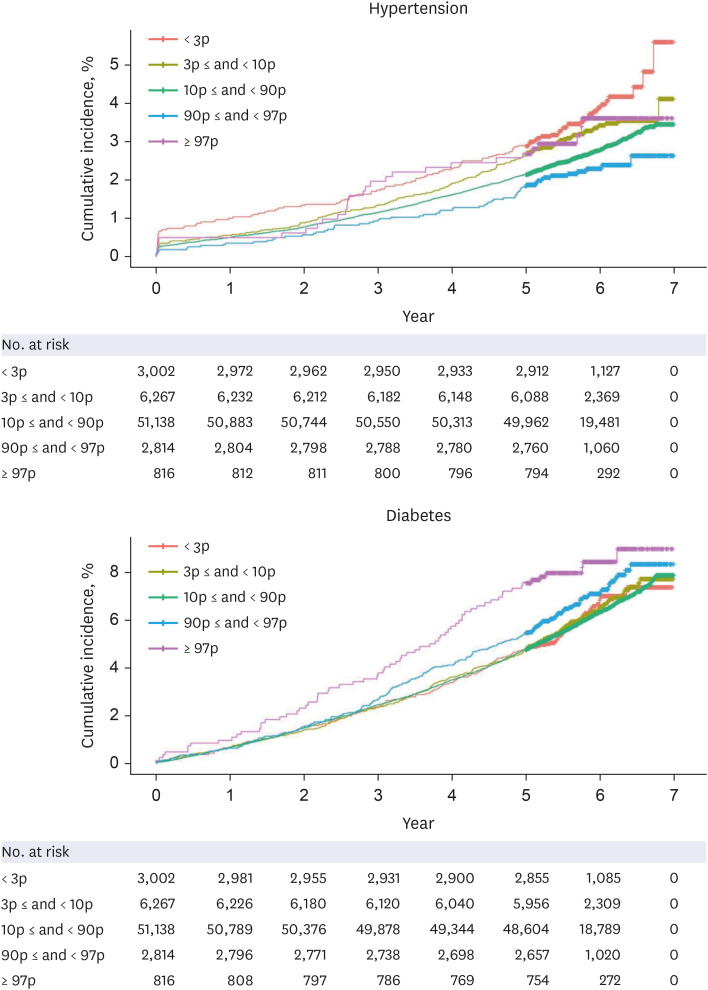
Fig. 4 compares the cumulative incidence of each outcome according to the offspring’s birthweight plotted against the follow-up duration. A low offspring’s birthweight was associated with the risk of maternal HTN, although only a few years had passed since delivery. In addition, a correlation between a high offspring’s birthweight and the risk of maternal DM was observed.
DISCUSSION
In this study, women who delivered SGA babies had an increased risk of HTN compared with that of women who delivered AGA babies. Moreover, in the case of giving birth to SGA babies, the lower the birthweight percentile, the greater the risk of developing HTN. However, the risk of DM only increased in the case of delivering a very LGA baby (birthweight > 97th percentile) after adjusting for maternal age, parity, gestational age at delivery, fetal sex, maternal BMI scores, and a history of smoking.
Pregnant women experience a multitude of vascular, metabolic, and physiological changes due to the increased demand placed on their bodies by the rapidly growing fetus and placenta. If these changes, including insulin resistance, adipose deposition, hypercoagulability, cardiac remodeling, and decreased vascular resistance, become a source of stress or fail to adapt properly in the body of certain women, adverse outcomes such as fetal growth disorders may occur. Consequently, these adverse outcomes can pose significant cardiovascular and metabolic challenges.252728 Therefore, pregnancy is often referred to as a physiological stress test because women who experience adverse outcomes during pregnancy have a higher risk of developing chronic diseases at a relatively young age after their first challenging pregnancy.
Most previous studies on inadequate fetal growth have focused on intrauterine growth retardation as a manifestation of ischemic placental disease. Women with pregnancies complicated by intrauterine growth restriction (IUGR) have an increased prevalence of HTN.2 Moreover, hypertensive pregnancy disorders are strong risk factors for subsequent postpartum HTN.2930 Most symptoms related to hypertensive pregnancy disorders are caused by an endothelial dysfunction31 caused by HTN.32 Furthermore, hypertensive pregnancy disorders can contribute to IUGR by reducing blood flow to the placenta, which can affect the fetal growth.33 In our study, we excluded hypertensive pregnancy disorders to analyze the relationship between the fetal growth and the risk of developing HTN. Therefore, we were able to investigate the relationship between these two factors after removing the influence of hypertensive pregnancy disorders. Researchers are increasingly exploring whether IUGR is an autonomous risk factor for cardiovascular disease in the future and whether it correlates with well-established indicators of cardiovascular health. Bijl et al. found that even in the absence of HTN, there are changes in cardiometabolic risk factors such as lipid profiles in IUGR. This substantiates the increased risk of future cardiovascular disease in individuals with non-hypertensive IUGR.34 This study corroborates our research, which revealed that a lower birthweight at the gestational age was associated with an increased risk of postpartum maternal HTN.
Several studies have investigated that the delivery of LGA babies increases the risk of maternal DM,2728353637 which is controversial especially since some studies have suggested that having both a history of gestational DM and the delivery of LGA babies increase the risk of DM.2728 In the current study, we used a large sample size to investigate the risk of DM based on the birthweight percentiles, after excluding women with a history of gestational DM. Our results showed that the risk of DM increased significantly only when the birthweight was above the 97th percentile, and no increase in the risk for birthweights between the 90th and 97th percentiles was observed.
HTN and DM are the most common chronic diseases that often coexist and have a significant impact on health. HTN can damage the blood vessels, heart, kidneys, and other organs and is a major risk factor for cardiovascular diseases. DM, a condition characterized by high blood glucose levels, can damage the blood vessels and organs, such as the kidneys, eyes, and nerves, and is similarly a major risk factor for cardiovascular diseases. Currently, pregnancy outcomes provide potential insights into women’s health.38 However, specific postpartum management strategies, such as targeted screening, lifestyle modification, and early treatment, have not been well-established. Therefore, it is necessary to develop appropriate postpartum follow-up systems for women who deliver LGA or SGA babies.
Limited research has been conducted on the relationship between the offspring’s birthweight and the postpartum maternal health. However, we conducted this research using large-scale national data and analyzed the results by categorizing birthweights according to percentiles. We targeted women with normal BMI scores and excluded other pregnancy complications that could affect the fetal weight. Controlling for other covariates that could affect HTN and DM, we confirmed the relationship between the offspring’s birthweight and the future risk of HTN or DM. In previous studies, the delivery of a SGA baby has been associated with later elevations in maternal systolic and diastolic blood pressures,39 as well as with HTN,6 although another study found no such associations.40 SGA birth has also been linked to later development of DM39 and elevated fasting glucose levels.40 In this study, we have added evidence that lower percentiles, especially < 3%, of SGA births are associated with a significantly increased risk of HTN, particularly within 2 years after delivery. Additionally, we addressed the inconsistency in previous research regarding maternal DM risk following LGA deliveries. We found that very LGA (> 97%) women had an increased risk of developing DM within 2 years after delivery, highlighting the importance of tracking and observing outcomes in the very SGA (< 3%) and very LGA (> 97%) births shortly after childbirth. This represents a significant strength of our study.
The current study had several limitations. First, diagnoses might be misclassified, as our definitions of comorbidities and cardiovascular outcomes were based on ICD codes. Second, because this study was conducted on Korean women, further research on other ethnic groups is required. Thirdly, the occurrence of HTN and DM tends to increase with advancing age, and it would have been beneficial to track them over a longer period. However, due to the characteristics of the data used in this study, extended long-term tracking beyond this point was challenging. Nevertheless, through this study, we were able to confirm that the risk of HTN and DM increases shortly after childbirth, depending on the offspring's birthweight category. Further long-term research will be needed in the future. Fourthly, the association between the development of HTN and DM and factors such as BMI, hyperlipidemia, and other metabolic parameters is well-established. Therefore, conducting additional analyses on metabolic status or lipid profiles in postpartum women could have potentially mitigated bias. However, these analyses were not conducted in the present study.
In conclusion, even if preeclampsia does not occur, giving birth to an SGA baby may increase the risk of postpartum maternal HTN. Similarly, delivering a baby with a birthweight above the 97th percentile, even without gestational DM, can increase the risk of postpartum DM. Our findings provide novel support for the use of the offspring’s birthweight as a predictor of future maternal diseases such as HTN and DM.
 XML Download
XML Download