

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vaccination is recognized as a crucial component of public health policies, and various national immunization programs (NIPs) have been implemented in Korea.123 As vaccination rates increase and the incidence of infectious diseases decreases, attention has shifted from diseases to adverse events following vaccination. The phenomenon of “vaccine hesitancy” has become a significant public health issue and the World Health Organization has designated it one of the top ten threats to global health.456 While vaccination is usually safe and effective in most patients, it is associated with unavoidable safety concerns, and proactive monitoring of adverse events is essential to maintain public trust.
In the United States (US), there are two large-scale vaccine safety monitoring systems: a passive surveillance called Vaccine Adverse Event Reporting System, an active surveillance called Vaccine Safety Datalink (VSD) and Post-licensure Rapid Immunization Safety Monitoring (PRISM).789 Canada also conducts both passive surveillance for all vaccines and active surveillance for pediatric vaccines through the Canadian Adverse Event Following Immunization Surveillance System (CAEFISS).10 In addition, Canada operates a hospital-based active monitoring system for serious adverse events following vaccination (Immunization Monitoring Program ACTive, IMPACT).11 Australia has an enhanced passive surveillance system called the AusVaxSafety.12
Although vaccine safety is also monitored in Korea, vaccines that are not included in the NIP are not monitored. The current NIP primarily targets children, except for a limited number of vaccines for adults in certain populations, such as the influenza vaccine for pregnant women and pneumococcal polysaccharide vaccine-23 valent and influenza vaccine for older adults. Additionally, the monitoring system for adverse events is fragmented between the Korea Disease Control and Prevention Agency (KDCA) which receives reports from patients and healthcare workers, and the Ministry of Food and Drug Safety (MFDS) which received data from pharmaceutical companies.1314 In both instances, passive surveillance is utilized.
As various adverse events of the coronavirus disease 2019 vaccine have emerged over the past few years, public interest in vaccine adverse events has increased.15 Therefore, systematic safety monitoring has become more important than ever, extending beyond the NIP to include non-NIP vaccines, especially in adult populations. Therefore, we aimed to establish a safety monitoring system for non-NIP vaccines in adults and propose mid- to long-term operational strategies for this system by analyzing the collected data. This ongoing research has been conducted since 2022 as a project supported by the MFDS.
METHODS
Selection of vaccines to be monitored
Vaccines to be monitored for adverse events were selected based on the following criteria: 1) vaccines with high administration rates in tertiary hospitals, and 2) vaccines suspected to have adverse events that are currently overlooked or require post-market surveillance due to recent introduction. We investigated the indications, sales volumes, and prescription statuses of various vaccines. As the Health Insurance Review and Assessment Service cannot provide information on non-reimbursed vaccines, pharmaceutical companies were contacted to inquire about domestic distribution and sales volumes. Subsequently, a literature review of the safety profile of each vaccine was conducted to determine any unusual adverse events that should be monitored. The target AEs to be monitored were selected if they are 1) commonly monitored by at least two surveillance systems among AEFI and SPEAC of WHO, VAERS and VSD of the United States, and ADVANCE-VAC4EU of Europe; 2) relevant to the population to be monitored (adults); and 3) considered to have reliable diagnostic codes.
Participating institutions
Data on vaccinations and cases treated for adverse events were collected from participating tertiary hospitals. At first, only tertiary hospitals were chosen because 1) they have dedicated research personnel, enabling the systematic collection of medical information and 2) data on emergency department visits and hospitalizations are available. The number of participating institutions was determined based on the number of recruited cases and the research funding. However, due to the limited number of collected cases, a decision was made to increase the number of participating hospitals and to include primary care clinics, which have the advantage of higher vaccination volumes compared to tertiary hospitals. Each institution assigns two dedicated personnel to complete case report forms, collect and distribute survey forms, register subjects, and collect medical records. In the cases of primary care clinics, researchers from nearby tertiary hospitals perform the tasks on their behalf. At tertiary hospitals, cooperation was requested from nurses in the injection room to ensure those who received vaccinations from doctors that did not participate in the study could be included as well.
Data collection by questionnaires
Individuals who received or were about to receive a vaccination were enrolled in the study. Informed consent was obtained before collecting information through questionnaires (Supplementary Table 1). The questionnaire included basic demographics, medical history, vaccination history, and adverse event history. Lot numbers, sites of injection, and concurrent vaccinations were also collected. Because most solicited adverse events that occur early after vaccination do not require hospital treatment, analyzing medical records is unsuitable, and spontaneous reporting from vaccinated individuals is necessary. Therefore, the participants were sent links via text messages to input multiple-choice or open-ended survey responses on days 1, 3, 7, 28, and 90 after vaccine administration. On days 1, 3, and 7, the occurrence and severity of the solicited local and systemic adverse events and the occurrence of unsolicited events were assessed. On Days 28 and 90, only the occurrence of unsolicited events was recorded.
Data collection by retrospective chart review
The medical information team provided a list of patients with a discharge diagnosis of an adverse event of special interest (AESI) every month. To double-check, hospitalized patient lists were screened weekly for AESIs, and medical records were reviewed for clinical information, including vaccination history within three months. Causality assessments were performed according to the KDCA guidelines.16 The evaluation results are presented as follows: 1) definitely related, 2) probably related, 3) possibly related, 4) probably not related, and 5) definitely not related.
Ethics statement
This study was reviewed and approved by the Institutional Review Board (IRB) of each participating hospital (IRB No. Korea University Guro Hospital, 2022GR0339; Kangnam Sacred Heart Hospital, 2022-07-014; Korea University Ansan Hospital, 2022AS0238; International St. Mary’s Hospital, IS22ENME0051). All individuals who participated in early adverse event surveillance provided written informed consent. The requirement for informed consent was waived for the retrospective chart review of the AESI cases.
RESULTS
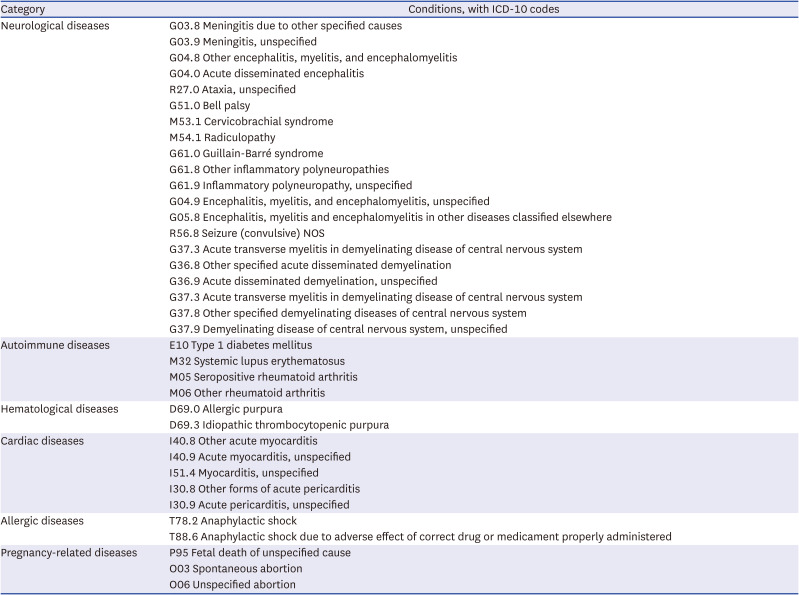
Four vaccines were selected: tetanus-diphtheria-pertussis vaccine (Tdap only; DTaP and Td were excluded), pneumococcal conjugate vaccine 13-valent (PCV13), zoster vaccine live (ZVL), and recombinant zoster vaccine (RZV). Inclusion of PCV15 and PCV20 is planned if approved for use in South Korea. No serious adverse events other than the commonly monitored AESI were identified in the literature review. The AESIs and diagnosis codes observed in this study are listed in Table 1. Initially, four tertiary hospitals participated, with 600–1,100 inpatient each. Ten primary care clinics were added later due to low vaccination volumes. All included institutions were located in the Seoul Metropolitan Area, where approximately half of the Korean population resides.
Table 1
List of the monitored adverse events of special interest
Enrolment started on October 1, 2022, and as of June 23, 2023, a total of 1,056 individuals were enrolled. The numbers of participants for each vaccine were as follows: PCV13, 240 (22.7%); Tdap, 300 (28.4%); ZVL, 222 (21.0%); and RZV, 293 (27.7%). Seven hundred and eighty-six (74.4%) participants were enrolled in tertiary hospitals, and 270 (25.6%) were enrolled in primary clinics. The number of responders on post-vaccination day 1 was 1,048 (99.2%), 988 (93.6%) on day 7, 855 (81.0%) on day 28, and 514 (48.7%) on day 90. The survey results are summarized in Supplementary Table 2.
Retrospective surveillance of AESIs began on September 1, 2022. As of July 15, 2023, 555 AESI cases had been identified. Ten (1.8%) patients received at least one vaccination within three months (Tdap in four cases, PCV13 in three, ZVL in three). Except for one case in which Tdap administration was possibly related to preeclampsia, all other cases were considered probably or definitely unrelated to vaccination.
DISCUSSION
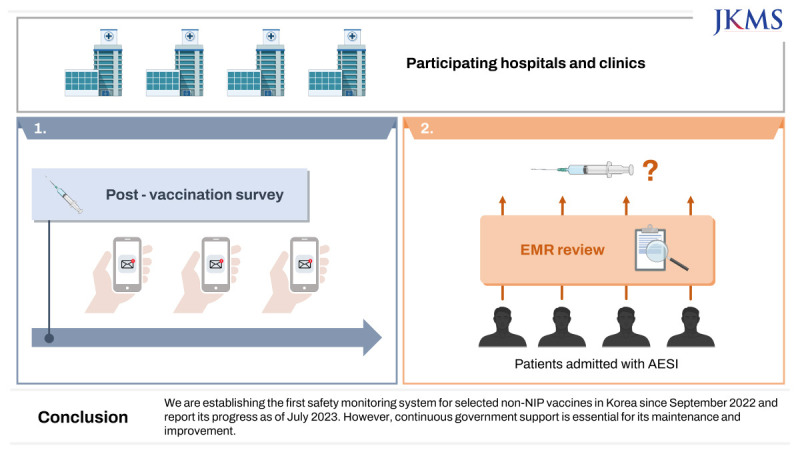
To establish a safety monitoring system for non-NIP vaccines, we conducted a survey of patients who received vaccinations at participating institutions, retrospectively reviewed inpatients with AESI diagnoses, and assessed the causal relationship between AESI and vaccination. This was the first attempt to monitor the safety of non-NIP vaccines in South Korea.
However, our system has some limitations. First, participant recruitment itself and survey completion at all time points was difficult. Despite the difficulty of operation and the similarity in the pattern of early adverse events between the present study and the existing literature, this monitoring approach should be maintained due to the significant time lag associated with the methods described later, especially in the event of unexpected AESI occurrences.1718192021222324252627 Second, retrospective screening was not efficient based on the scale of efforts, and the number of participants included in this study was too small to observe rare AESI cases. Moreover, the rate of AESI may have been underestimated. In South Korea, where many individuals visit more than one healthcare institution for different health conditions, a considerable proportion of patients with AESI are expected to receive treatment at hospitals other than those where they were vaccinated. In this case, confirming vaccination history is difficult because of the inability to access medical records across hospitals.
The VSD, operated by the US Centers for Disease Control and Prevention, combines data from nine large healthcare institutions to collect all medical records.8 It periodically compares the incidence rates of AESI between vaccinated and unvaccinated individuals and reviews medical records for certain major conditions. PRISM, another US surveillance system, combines data from three national health insurance databases and eight immunization registries.9 Canada’s CAEFISS monitors hospitalizations due to pre-specified serious adverse events and verifies vaccination history to report suspected vaccine-attributable cases to health authorities.10 In Australia, patients who receive NIP vaccines at institutions participating in the AusVaxSafety system receive text message notifications, and in cases of serious adverse events, public officers contact them to collect additional information. The collected adverse reaction data are analyzed weekly.12
The approach used in this study was similar to that used in Canada and Australia. To enable more thorough data collection, combining multi-institutional data, as in the US, would be desirable. In this regard, we are planning to combine anonymized data from participating hospitals with National Health Insurance Service (NHIS) data. Korea has a universal, single-payer healthcare coverage that enables the identification of AESI diagnosed at any institution. However, even if such an integrated dataset is built, it will mainly consist of data from tertiary hospitals, and lacking data from primary clinics, the main source of vaccine administration data. This is so as electronic medical record systems are weak in clinics. In addition, because the NHIS only provides data for claims that have been reviewed, real-time analysis is impossible because only outdated data are available.
For the expansion and long-term operation of this safety monitoring system, substantial maintenance workload is required. Therefore, consistent support from the MFDS is crucial. Ultimately, for more comprehensive monitoring, it is desirable to include vaccines administered in primary clinics. For this purpose, we propose to reimburse vaccination service fees (for injections and monitoring) for non-NIP vaccines. By doing so, non-NIP vaccinations can be identified in the NHIS data, making it easier to monitor not only safety but also effectiveness. In addition, we are planning to combine multi-center pseudonymized electronic medical records (common data model) and public health big data of NHIS or Health Insurance Review and Assessment Service to monitor AESIs of non-reimbursed vaccines.
In conclusion, we are establishing a safety monitoring system for selected non-NIP vaccines for the first time in Korea and its progress is demonstrated here. Efforts to build a sustainable and effective vaccine surveillance system will continue and update results will be reported.
 XML Download
XML Download