

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Helicobacter pylori is a Gram-negative bacterium that colonizes and persists in the stomach.1 It can be transmitted from an infected person to an uninfected person by direct contact via an oral-oral, fecal-oral, or both routes.23 Most people become infected during their childhood, and parents and siblings appear to play a significant role in pathogen transmission.34 Once infected, H. pylori causes lifelong chronic progressive gastric inflammation, which can lead to clinical complications in up to 10% of infected individuals.15 The major clinical complications include peptic ulcer disease, chronic gastritis, gastric cancer, and mucosa-associated lymphoid tissue lymphoma.12567 The prevalence of H. pylori infection varies widely according to geographic area, age, and socioeconomic status.6 Although the prevalence of H. pylori is decreasing due to improving hygiene and standard of living, it remains high, particularly in the Eastern Asian countries.68910
A combination of two to three antibiotics (from a few antibiotics such as amoxicillin, clarithromycin, metronidazole, tetracycline, levofloxacin, and rifabutin) and an acid-suppressive agent with or without bismuth are used to eradicate H. pylori.111213 However, the successful eradication rate of H. pylori has decreased in the past decades, in parallel with increasing antibiotic resistance.14151617181920 Antibiotic resistance of H. pylori is particularly important because this is one of the most common causes of bacterial infections worldwide, affecting millions of people every year.16 Additionally, overuse or inappropriate use of antibiotics can contribute to the development of antimicrobial resistance in H. pylori and other bacteria, which can have serious public health implications.212223 Recently, the World Health Organization listed H. pylori as a serious threat to human health for their resistance against most available treatment regimens.24
The molecular mechanisms underlying antibiotic resistance in H. pylori infection are diverse and complex. Several mechanisms have been proposed to drive the antibiotic resistance of H. pylori, including genetic mutations in the bacterium itself and physiological changes that can upregulate efflux pump expression in bacterial cells.252627282930 Cellular adaptation associated with biofilm or coccoid formation, which protects drug penetration into bacterial cells, is another potential resistance mechanism.3132 Many of these resistance mechanisms can work in concert to confer multidrug resistance (MDR) in H. pylori, making eradication increasingly challenging and highlighting the need for new therapeutic strategies. In this review, the mechanism of resistance of H. pylori to commonly used antibiotics and their clinical implications are explored.
MOLECULAR MECHANISMS OF ANTIBIOTIC RESISTANCE
Mechanism of single-drug resistance
Single-drug resistance refers to a situation in which a microorganism, such as a bacterium, virus, or fungus, is resistant to only one type of drug while remaining susceptible to other drugs. Although the eradication regimen for H. pylori consists of a combination of antibiotics, resistance to a single antibiotic agent could result in eradication failure.33 Antibiotic resistance in H. pylori is mainly from de novo genetic mutations that disrupt the activity of antibiotics by either altering the drug target or inhibiting drug activation within cells (Table 1 and Fig. 1).7 With advances in next-generation sequencing (NGS), many mutations have been observed in resistant clinical isolates.25263435 However, the relative contribution of each mutation to phenotypic resistance and the effect of combinations of mutations remain unclear.36
Table 1
Mechanisms of antibiotic resistance in H. pylori
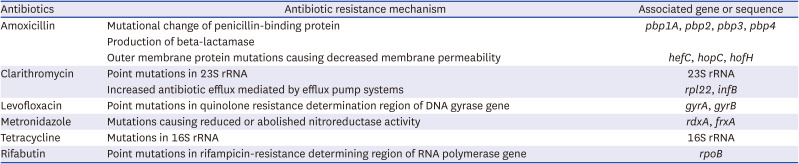
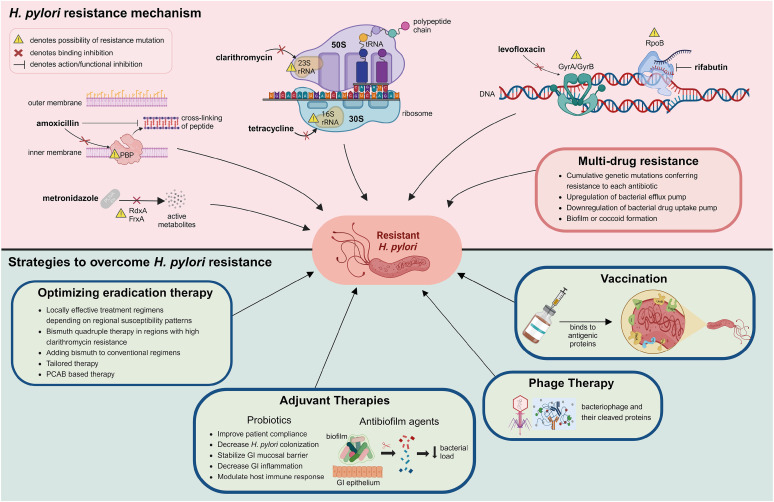
Fig. 1
Overview of molecular mechanism of antibiotic resistance in H. pylori and strategies to overcome this resistance. This image was created with BioRender.com.
FrxA = NAD(P)H flavin oxidoreductase, GI = gastrointestinal, GyrA = DNA gyrase subunit A, GyrB = DNA gyrase subunit B, PBP = penicillin-binding protein, PCAB = potassium-competitive acid blocker, RdxA = oxygen-insensitive NAD(P)H nitroreductase, RpoB = β-subunit of DNA-dependent RNA polymerase, rRNA = ribosomal RNA, tRNA = transfer RNA.
Beta-lactams
Amoxicillin is widely used for H. pylori eradication in combination with acid-suppressive agents to improve drug stability and efficacy. After administration, amoxicillin is well absorbed into bloodstream and then released into the gastric juice.37 In a favorable environment with acid-suppressive agents, amoxicillin exerts its antimicrobial effect by binding to penicillin-binding proteins (PBPs).3839 Binding of amoxicillin to PBPs inhibits the synthesis of peptidoglycan, a major component of bacterial cell walls, resulting in cell wall lysis in replicating bacteria.3940 Amoxicillin generally shows a low antibiotic resistance rate.41424344 In H. pylori, amoxicillin resistance is mainly due to mutational changes in PBP1A.45464748 Mutations in other PBPs (PBP2 and PBP 3) have also reported, and multiple mutations in all three isotypes PBP1, PBP2 and PBP3 was found to confer high level of amoxicillin resistance when compared to the amoxicillin susceptible strain.49 Beta-lactamase activity, which can hydrolyze amoxicillin to attenuate the optimum concentration needed to elicit bactericidal effect, was also found in H. pylori.4050 Furthermore, amoxicillin resistance may be contributed by mutations in hefC, hopC, and hofH, which are likely associated with changes in the composition of the outer membrane and membrane permeability of H. pylori.515253
Macrolides
Clarithromycin is widely used in the frontline regimen to eradicate H. pylori. Clarithromycin has pharmacokinetic advantages over other macrolides, including increased oral bioavailability, higher plasma concentration, and longer elimination half-life.54 Concomitant administration with acid-suppressive agents also increases its stability in acidic environments.55 Clarithromycin exerts antimicrobial effects by binding to the peptidyl transferase loop of domain V in the 23S ribosomal RNA (rRNA) in the bacterial ribosomal subunit 50S. Mutations in domain V of the 23S rRNA gene of H. pylori, A2142G/C and A2143G, can result in reduced binding affinity of the antibiotic agent, making it less effective at inhibiting bacterial growth.5657 Other point mutations are also reported in the 23S rRNA in H. pylori isolates.25262758 In addition, studies using experimentally induced resistant phenotype for clarithromycin found that mutations in rpl22 and infB genes had synergistic effects with mutations in the 23S rRNA genes, resulting in higher minimum inhibitory concentration of clarithromycin.3435 Another relevant mechanism for clarithromycin resistance is attributed to the efflux pump system.2959 However, the role of novel mutations and specific function of efflux pump system in the development of clarithromycin resistance in clinical isolates should be further clarified.
Fluoroquinolones
Among the fluoroquinolones, levofloxacin, moxifloxacin, and sitafloxacin have been used for H. pylori eradication therapy. Due to high resistance rate, fluoroquinolones are generally used in rescue treatment after initial eradication failure.116061 Fluoroquinolones act on microbes by inhibiting bacterial topoisomerase II (DNA gyrase) and topoisomerase IV enzymes involved in bacterial synthesis of nucleic acid, a step proceeding cell division and proliferation.28 The most common mechanism of fluoroquinolone resistance in H. pylori is due to a specific mutation in one or more of gyrA and gyrB genes.62 The region where mutations arise in these genes is a short DNA sequence known as the quinolone resistance-determining region (QRDR).6364 Fluoroquinolone resistance of H. pylori is mainly due to point mutations of codon position 87 and 91 in the QRDR of gyrA.656667 These few mutations associated with most cases of phenotypic resistance indicate that molecular testing for levofloxacin can be a reliable substitute for culture and antimicrobial susceptibility testing. Mutations present outside the QRDR region of gyrA or in the QRDR region of gyrB have also been reported to be associated with levofloxacin resistance; however, the impact of these mutations requires further investigation.26275866
Nitroimidazole
Among the nitroimidazoles, metronidazole is frequently used to eradicate H. pylori infections. Metronidazole is actively released into gastric juice after oral ingestion, with the acidic condition in the stomach rarely affecting its antimicrobial activity.68 Metronidazole is a prodrug that needs to be activated by intracellular reduction of the nitro group attached to the imidazole ring.69 Reductive activation of metronidazole causes imidazole fragmentation and nitro-anion free radicals which are cytotoxic.6970 The reduction of metronidazole is mainly mediated by oxygen-insensitive NAD(P)H nitroreductase (RdxA), NAD(P)H flavin oxidoreductase (FrxA), and ferredoxin-like enzymes (FdxB) in H. pylori. Metronidazole resistance in H. pylori is primarily due to decreased drug activation mediated by mutations in RdxA gene which encodes an oxygen-insensitive NAD(P)H nitroreductase.70717273747576 Mutations involving the FrxA gene were also reported.357477 However, metronidazole resistance was observed in H. pylori isolates without the loss of functional RdxA and FrxA, suggesting that other factors are involved in metronidazole resistance.7278798081 Other putative mechanisms of metronidazole resistance in H. pylori include mutations in FdxB, ferric uptake regulator (Fur), and enhancement of efflux pump (HefA) protein.72828384
Tetracyclines
Tetracycline is stable in gastric pH and acts as a topical agent on the surface of the gastric mucosa against H. pylori.85 At the bacterial cytoplasm, tetracycline binds to bacterial ribosomes and interacts with a highly conserved 16S rRNA target in the 30S ribosomal subunit, arresting translation and protein synthesis.86 Resistance mechanism of H. pylori against tetracycline is not widely studied because tetracycline resistance is not common in clinical isolates.14414487 Among various mechanisms of tetracycline resistance, the major resistance mechanisms are related to mutations in the 16S rRNA genes.888990 However, tetracycline resistance without mutation in the 16S rRNA gene has been reported, suggesting that other mechanisms, such as efflux, are associated with tetracycline resistance.8491
Rifamycins
Rifamycins are transcriptional inhibitors that specifically inhibit the activity of bacterial transcription by binding to RNA polymerase, mostly β-subunit encoded by the rpoB gene.92 Among the rifamycins, rifabutin has better pharmacokinetics than rifampicin and is used for H. pylori eradication. Rifabutin is chemically stable at a wide range of pH values and is not inactivated by gastric acid.93 The resistance rate of H. pylori against rifabutin is low, and most rifabutin-resistant strains were isolated after treatment failure.949596 In H. pylori, the molecular mechanism driving rifabutin resistance is at least one point mutation in the rifampicin resistance-determining region of the rpoB gene.27979899100 However, a previous study reported that rifabutin-resistant strains were successfully eradicated with rifabutin-based triple therapy.101 Correlations between rpoB gene mutation status, phenotypic resistance, and treatment outcome need further clarification.
MDR in H. pylori
The presence of H. pylori strains with MDR profiles poses a significant challenge for H. pylori eradication and complicates the management of H. pylori-related diseases. The MDR profile of H. pylori is expressed as the cumulative result of genetic mutations conferring resistance to each antibiotic agent.7 Other putative mechanisms of H. pylori MDR include physiologic changes in bacterial cells (upregulation of efflux pump systems or downregulation of drug uptake proteins in the outer membrane of bacteria) and cellular adaptation properties (biofilm or coccoid formation).59102103104105
Bacterial biofilms are complex microbiological ecosystems where adherent aggregates of microorganisms surround themselves in multidimensional extracellular polymeric substances.106107 Biofilms are often associated with chronic infectious diseases as they protect the bacteria from unfavorable environments, antimicrobial exposure, and host immune system.31108 Biofilm formation in H. pylori has been observed both in vitro (environmental water body) and in vivo (gastric mucosa).109110 The presence of biofilm was shown to be associated with decreased susceptibility to antibiotics in H. pylori.31 Previous studies showed that mutations in several genes coding for flagellar protein, outer membrane protein, cytotoxin-associated gene pathogenicity island protein, or efflux pumps were responsible for biofilm formation in H. pylori, which can further potentiate antibiotic resistance.84111112 However, the precise mechanisms for H. pylori biofilm formation have yet to be determined. In addition, the clinical implications of biofilm formation on the development of antibiotic resistance in H. pylori and treatment outcomes should be further investigated.
An exceptional feature of H. pylori is the formation of a viable but non-culturable coccoid morphology. In H. pylori, the coccoid form becomes dominant when bacteria are exposed to environmental stress conditions, such as starvation, prolonged culture, and exposure to antibiotics.113114 It has been reported that this dormant state of H. pylori induces ultrastructural modifications in the cell membrane and metabolic pathways that contribute to antibiotic resistance.24107 However, the clinical relevance of coccoid formation in the development of MDR profile and treatment outcome of H. pylori is not fully understood.
Heteroresistance
Heteroresistance refers to a phenomenon where subpopulations of bacteria have different antibiotic susceptibility profiles.115 Heteroresistance in H. pylori has been reported in several studies in which both susceptible and resistant bacterial strains were isolated either from the same biopsy site (intraniche) or from different sites (interniche).87115116117118119120121122 Heteroresistance can be developed through evolutionary change in a single strain or mixed infection of multiple bacterial strains.7 Previous studies reported that heteroresistant H. pylori strains had similar fingerprinting patterns, suggesting that the presence of the same strain with mixed susceptible and resistant phenotype, rather than coinfection of different strains, is associated with the development of H. pylori heteroresistance.117118119120121 The possibility of heteroresistance should be considered during antimicrobial susceptibility testing and eradication therapy for H. pylori infection since underestimation of the presence of antibiotic-resistant strain may lead to treatment failure. To address this issue, multiple biopsies from different sites in the stomach or multiple bacterial colonies from the same sample should be obtained when evaluating the antimicrobial susceptibility of H. pylori.
Antimicrobial susceptibility testing
With increasing antibiotic resistance, it is imperative to develop individualized therapeutic approaches based on the results of antimicrobial susceptibility tests. Common methods for antimicrobial susceptibility testing include culture-based antimicrobial susceptibility testing and molecular detection. Bacterial culture is necessary for the use of conventional antimicrobial susceptibility tests, such as E-test, disk diffusion method, and agar dilution method.3942123 However, H. pylori culture requires specific conditions, is time-consuming, and is affected by several factors, such as transport conditions and the time interval between specimen collection and inoculation, limiting its availability in clinical practice.
Molecular methods are also used to assess antimicrobial susceptibility. Since the resistance of H. pylori to clarithromycin, fluoroquinolones, and tetracycline is mainly driven by specific point mutations in a small region of the responsible gene, molecular methods can be utilized for antimicrobial susceptibility testing. Polymerase chain reaction (PCR) was used to assess antibiotic resistance by detecting resistance-associated mutations. Similarly, PCR-restriction fragment length polymorphism, real-time PCR, multiplex PCR, and droplet digital PCR have been widely used to determine antibiotic resistance in H. pylori.124125126127128129 Currently, several commercial kits are available to detect clarithromycin resistance, levofloxacin resistance, or both.130131132133134135 Another diagnostic tool using loop-mediated isothermal amplification methods, combined PCR and quenching probe method, and single cell-based antimicrobial susceptibility test Ramanometry has been introduced.136137138139
Compared to conventional methods, molecular detection methods have the advantages of high sensitivity, specificity, and reproducibility, and disadvantages such as high cost. Furthermore, as molecular detection methods target specific gene loci, antibiotic resistance caused by other mutations cannot be detected, leading to false-negative results.140 In addition, as metronidazole has complex resistance mechanisms and the presence of metronidazole resistance does not necessarily lead to treatment failure, the role of molecular detection of metronidazole resistance is limited.
Recent advances in high-throughput molecular detection technology, including NGS and metagenomic analysis, have enabled the detection of H. pylori infection and antibiotic resistance.25262734 While NGS provides comprehensive information, applying NGS results to clinical practice requires additional knowledge about the correlation between NGS results and phenotypic resistance as well as treatment outcomes.141 In addition, cost-effectiveness and availability should be considered for the clinical application of NGS to predict antibiotic susceptibility profiles.
CILNICAL IMPLICATION AND FUTURE DIRECTIONS
The main clinical implication of antibiotic resistance in H. pylori is significantly compromised eradication therapy efficacy. It is well-known that the eradication success rate using clarithromycin-based regimens is markedly decreased in the presence of clarithromycin resistance.33142143 Accordingly, clarithromycin containing standard triple therapy is recommended only in areas with a clarithromycin resistance rate of less than 15%.11 On the other hand, a lower decrease in eradication rates has been observed for metronidazole, and successful eradication was reported using bismuth quadruple therapy, especially with higher metronidazole dose, even in the presence of metronidazole resistance.33142143 Multiple different mechanisms leading to metronidazole resistance and diversity of identified mutations may explain the relatively poor correlation between phenotypic resistance against metronidazole and treatment outcome. The increasing number of MDR H. pylori strains has made eradication therapy more challenging. Given that the first-line treatment regimen is usually selected empirically rather than based on antimicrobial susceptibility testing, failure of initial eradication therapy is another important cause of the emergence of MDR H. pylori strains.
The development of antibiotic resistance in H. pylori has reduced available treatment options. Eradication failure necessitates additional rounds of therapy, including alternative antibiotic combinations. With the decline in the eradication rates of standard therapies, physicians face challenges in selecting effective alternatives. However, these options are not always effective, involve higher pill burdens, and can lead to more side effects. There have been some important changes to expert recommendations for H. pylori eradication: more frequent use of bismuth-containing quadruple therapy as a first-line treatment instead of clarithromycin-based triple therapy is recommended.144 The limited arsenal of effective treatments against antibiotic-resistant H. pylori strains underscores the need for novel treatment strategies, including non-antibiotic approaches, to address this growing problem (Fig. 1).
Optimizing eradication therapy
Current treatment regimens for H. pylori eradication are derived from empirical approaches developed by gastroenterologists over the past few decades. A significant decrease in the eradication rate worldwide, along with an increasing trend of H. pylori antibiotic resistances warrants more specific approach to H. pylori eradication therapy, utilizing antimicrobial stewardship.145 Given that antibiotic resistance patterns differ according to geographic regions, it is recommended to use treatment regimens that are locally effective according to regional susceptibility patterns.87145146 However, many regions lack reliable data on the prevalence and characteristics of antibiotic resistance in local populations to guide the selection of empirical eradication therapy. Currently, bismuth quadruple therapy is recommended in regions with high antibiotic resistance to both clarithromycin and metronidazole.11 In addition, adding bismuth to some triple regimens and prolonging the treatment duration to 14 days can increase eradication rates up to 30% or more, even in the presence of antibiotic resistance in some strains.13 Recent meta-analysis also showed that bismuth supplements as the first-line regimen showed better eradication rate compared to non-bismuth containing regimens.147
Tailored therapy
With increasing resistance rates and MDR H. pylori strains, the role of antimicrobial susceptibility testing and subsequent individualized antibiotic treatment has been emphasized.11 Tailored therapy, in which antibiotics are chosen based on the antimicrobial susceptibility profile, is an ideal therapeutic option to improve the efficacy of H. pylori eradication therapy while minimizing unnecessary prescription of antibiotics. Studies have reported better eradication success rates using tailored therapy than empiric therapy, especially when antimicrobial susceptibility testing was performed before treatment.148149150151 However, the benefit of tailored therapy has not been demonstrated in clinical trials comparing tailored therapy with empirical quadruple regimens as a first-line treatment or tailored therapy after previous treatment failure.151152153 This suggests that the benefit of tailored therapy is not obvious when the empirical regimen is highly effective for H. pylori eradication. In addition, the limited availability of H. pylori cultures and antimicrobial susceptibility testing has made this approach difficult. More evidence is required to establish the generalized use of tailored therapy for H. pylori eradication.
Acid suppression with potassium-competitive acid blocker
To increase eradication success, antibiotic resistance patterns and patient characteristics, such as compliance and cytochrome P450 2C19 genetic polymorphisms, should be considered. Potassium-competitive acid blocker provides fast and long-lasting acid suppression and is recently used for H. pylori eradication therapy in combination with various antibiotics.154155156157 Vonoprazan-based triple therapy showed higher eradication rate compared to proton pump inhibitor (PPI), especially in the subpopulation with clarithromycin resistance, potentially overcoming clarithromycin resistance.158159 Recent meta-analysis of randomized controlled trials also showed that vonoprazan-containing regimens achieved a higher eradication success rate compared to PPI-based regimens.160 In line with this, a Japanese guideline recommends vonoprazan-based triple therapy or PPI-based triple therapy as the first-line treatment for H. pylori eradication.161 Vonoprazan-based dual therapy consisting amoxicillin may be another treatment option while minimizing unnecessary antibiotic use; however, the dosage and duration of dual therapy need to be further determined.159162163 Notably, most studies on vonoprazan-based regimens were conducted in Japan, and further studies are needed to confirm these promising results in different regions.164165
Adjuvant therapies
Adjuvant therapies aim to enhance the efficacy of antibiotic treatment either by overcoming the bacterial mechanisms of antibiotic resistance or by modifying the host response. These include the use of probiotics and anti-biofilm agents. As supplementary to conventional eradication therapy, probiotics can reduce gastrointestinal adverse events and thus improve patient compliance.166167 In a recent meta-analysis, it has been found that most probiotics added to triple therapy provided better treatment outcomes.167 The potential mechanisms of probiotic action against H. pylori include direct and indirect inhibitory effects against H. pylori colonization, stabilization of gastric mucosal protective barrier and reduction of gastric mucosal inflammation, and modulation of host immune response to the infection.168169 Probiotic supplementation also reduced antibiotic-induced alteration of gut microbiota and helped the restoration of dysbiosis caused by eradication therapy.170171 However, further research is needed to better understand the role and mechanism of action of probiotics in H. pylori eradication therapy, as the species and strains, dose, and duration of investigated probiotics are heterogeneous.
An alternative therapeutic approach is to target and disrupt bacterial biofilms. Previous studies have shown that the use of N-acetylcysteine (NAC) reduces bacterial load and enhances eradication rate.172173 The effect of NAC was also found in a clinical trial, showing better clearance of H. pylori in patients treated with NAC before antibiotic treatment.174 However, the exact mechanism underlying the reported therapeutic effect of NAC in the disruption of biofilms and overcoming H. pylori antibiotic resistance has yet to be defined. In a recent study, the combination of antibiotics and rhamnolipid, a glycolipid biosurfactant capable of disrupting biofilm and potentially inhibiting bacterial adhesion, was reported to effectively inhibit biofilm formation in vitro.175 Although the results are promising, the roles of rhamnolipid and anti-biofilm compounds need further investigation in vitro and in vivo.
Phage therapy
The rise in antibiotic resistance has increased interest in studying bacteriophages, particularly lytic bacteriophages. Phage therapy has various potential advantages over antibiotics because phages and their cleaved proteins are highly specific, affecting the target strain but not the microbiome.176 Furthermore, phages exclusively replicate at the site of infection, and no secondary effects have been reported.177 Few studies have investigated the presence of phages in H. pylori strains, including prophages and lytic phages.178179180181 However, the exact function and properties of phages to be used therapeutically are yet to be determined. Although phage therapy appears to be a promising approach for future treatment options for H. pylori infection, further investigations are required to improve our understanding of phage and H. pylori interactions, which are still in the exploratory stage.
Vaccination
Developing an effective vaccine against H. pylori could be a game-changer in preventing infections and reducing the reliance on antibiotic treatment. Several vaccine candidates are currently under investigation, aiming to elicit a protective immune response against H. pylori; however, few have shown a protective effect.182183184185186187188189190191192193194 In a randomized, double-blind, placebo-controlled, phase 3 clinical trial, three doses of oral recombinant H pylori vaccine were introduced in children and were followed up for the next three years.194 The vaccine was effective against H. pylori in 71.8% of subjects without any serious adverse events. However, the authors suggested a longer follow-up period to confirm protective effects against H. pylori-associated diseases. The search for an effective vaccine is in the exploratory stage and needs further investigations, considering better design of vaccine strategies, optimal combination of antigens, selection of suitable adjuvants, and proper delivery carriers. Additionally, given that H. pylori infection usually occurs in early childhood, the optimal timing of vaccination and subsequent follow-up strategies to ensure the protective effects of vaccination should be further elucidated.
CONCLUSIONS
The increasing rates of H. pylori antibiotic resistance and MDR strains pose significant challenges for eradication therapy. Substantial progress has been made in understanding the fundamental mechanisms underlying antibiotic resistance in H. pylori, including genetic mutations, efflux pump systems, and biofilm formation. To overcome antibiotic resistance of H. pylori, antibiotic stewardship and tailored therapy based on antimicrobial susceptibility testing are recommended. Strategies such as adjuvant treatment, phage therapy, and vaccine development are currently being explored. In addition to optimizing currently available treatment options, continuous monitoring of local resistance profiles, ongoing research, and the development of innovative therapies are required to effectively manage antibiotic-resistant H. pylori infections and associated gastrointestinal diseases.
 XML Download
XML Download