

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
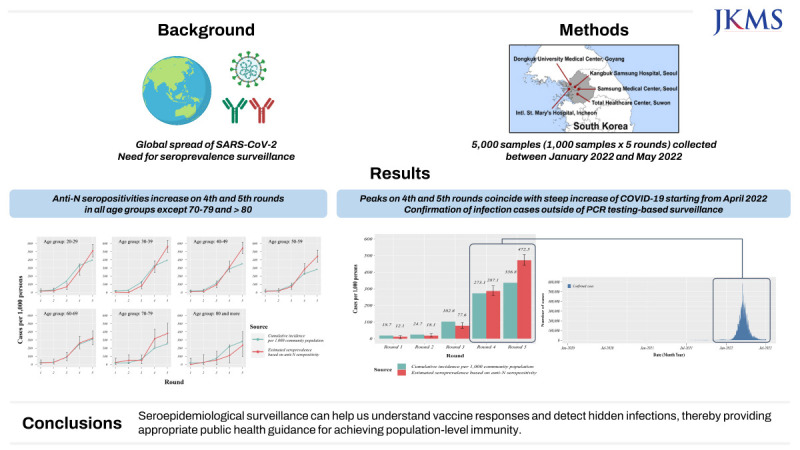
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread globally, leading to the coronavirus disease 2019 (COVID-19) global pandemic. In South Korea, since the first domestic case in January 2020, more than 29 million people have been infected with COVID-19 as of January 2023.12 Real-time reverse transcription polymerase chain reaction (RT-PCR) is used to confirm COVID-19 in individuals who are infected or in close contact with an infected person.3 However, approximately 40% of SARS-CoV-2 infections are caused by asymptomatic cases that can still transmit the virus.45 Therefore, PCR testing can underestimate the overall COVID-19 infection status in asymptomatic individuals, and those in contact with them may not undergo voluntary PCR testing. The World Health Organization and Center for Disease Control recommend the use of COVID-19 antibody tests to identify the extent of infection spread in a community at the population level.67 To gain insight into the seropositivity rates resulting from the substantial transmission of asymptomatic and subclinical patients, population-based seroprevalence surveys should be performed.
Population-based seroprevalence studies have been conducted in South Korea since the onset of the COVID-19. In the earliest stages, domestic serosurveys were conducted on a small number of participants in a restricted area, revealing low seropositivity rates.89 In January 2020, 0.07% (1/1,500) was anti-nucleocapsid (N) seropositive in Southwestern areas in Seoul, the capital city of South Korea.9 In May 2020, 7.6% (15/198) was anti-N and anti-spike (S) seropositive in Daegu, a Southeastern city in South Korea.8 Subsequently, larger-scale population-based serosurveys were conducted, which also reported low seropositivity rates. Between late 2020 and early 2021, less than 1.0% was seropositive in approximately 5,000 individuals across major cities in South Korea according to the serosurveys conducted on health examinees.101112 Between September and December of 2020, overall seroprevalence was 0.39% among 4085 subjects.12 Between April and December 2020, 0.09% was seropositive among 5,284 subjects.10 Between January and March 2021, it was 0.55% in women and 0.38% in men among 4,942 subjects.11 However, these studies were conducted when the pandemic was still in its early stages and did not take into account the distribution of the general population. Moreover, they were conducted before the initiation of a nationwide vaccination targeting the general population, highlighting the need for population-based serosurveys after the implementation of the vaccination program.
A nationwide vaccination program against COVID-19 began in South Korea in February 2021, and as of January 2023, the total number of vaccine doses administered per 100 people was 264.37.13 By May 2022, approximately one-third of the total population of South Korea (33%, 17 million/51 million) had been infected with SARS-CoV-2, according to official PCR testing, while 85% of the population had received at least two doses of COVID-19 vaccines.14 Particularly in January 2022, when 30,702,960 confirmed cases were officially reported in South Korea, 52.2% (cumulative incidence of 5,962,320 in Seoul; 1,782,454 in Incheon; and 8,298,093 in Gyeonggi province) were residents of the capital metropolitan area of South Korea.1
Because a significant proportion of the COVID-19 confirmed cases were concentrated in the capital metropolitan area of South Korea, and a large proportion of the population in the area had been adequately vaccinated against COVID-19, we conducted a seroprevalence surveillance study focusing on the residents of the capital metropolitan area in South Korea. This study aimed to estimate humoral immune status by assessing vaccine-induced seroconversion and COVID-19 infection among participants. The significance of this study lies in the fact that it is the first prospective consecutive study focusing on the general population conducted after the initiation of a nationwide vaccine program.
METHODS
Study design and population
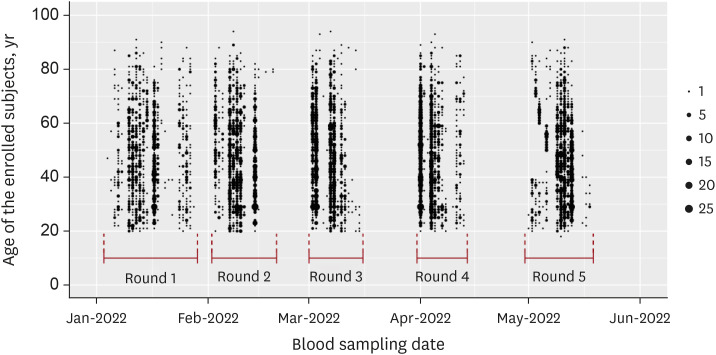
To ensure that the sample size was representative of the general population living in South Korean capital metropolitan areas including Seoul, Incheon, and Gyeonggi province, we used a quota sampling method and determined 5,000 participants to represent the population of the metropolitan area (Fig. 1). We determined the sample size based on the population data retrieved from the official government website of South Korean Ministry of Interior and Safety. The retrieved data included male and female population number of registered residents over 20 years old living in Seoul, Incheon, and Gyeonggi province counted at the middle day of the year 2020.15 The population data according to age intervals and sex is shown in Supplementary Table 1. To ensure that the enrollees were the representatives of each residents living in the metropolitan area, five medical institutions from two in Seoul, two in Gyeonggi, and one in Incheon were selected (Fig. 1). To assess changes in seropositivity over time, we conducted five consecutive cross-sectional survey rounds from January 2022 to May 2022 which included 1,000 individuals per month. Each 1,000 enrollees per month were equally stratified across seven age categories (20–29 years, 30–39 years, 40–49 years, 50–59 years, 60–69 years, 70–79 years, and > 80 years) and sex determined by quota sampling method across five medical institutions located in Seoul, Incheon and Gyeonggi province. These monthly enrollment and blood sampling were aimed to be done at the middle of each month (Fig. 2).
Fig. 1
A flow chart explaining study design and interpretation of anti-N and anti-S antibody test results. Map of South Korean metropolitan area indicates the five medical institutions (No. 1–5 indicated by red dots) that participated in sample collection. The gray shaded area includes Seoul, Incheon, and Gyeonggi province. Individuals who visited outpatient/healthcare clinics or emergency department of each medical institution were selected to meet inclusion and exclusion criteria. Age and gender determination for enrollment was made according to official population survey data from South Korea Ministry of the Interior and Safety.
N = nucleocapsid, S = spike, SKKU = Sungkyunkwan University Department of Social and Preventive Medicine.
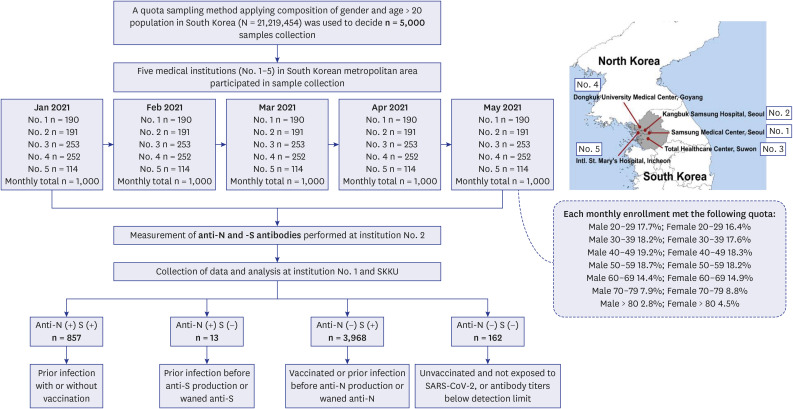
Fig. 2
Distribution of sample collection date for SARS-CoV-2 antibody tests according to age groups over the five survey rounds from January 2022 to May 2022. The black dots represent the size of samples while the vertical positions indicate the collection date in each round (month), with each block representing a 15-day interval.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
The individuals who had visited outpatient clinics of Samsung Medical Center, Kangbuk Samsung Hospital, International St. Mary’s Hospital, Dongguk University Medical Center and visitors of Total Healthcare Center at Suwon were included. Among these individuals who were confirmed as residents of the corresponding areas, factors potentially affecting human immune responses were carefully reviewed. Therefore, individuals with hematological malignancies, cancer, autoimmune disorders, severe cardiopulmonary diseases, infectious diseases other than COVID-19, or a history of organ or stem cell transplantation were excluded. We also excluded patients receiving immunosuppressive therapy, such as steroids, immunosuppressants and immunotherapeutic agents. We applied strict exclusion criteria at five medical institutions to ensure that the enrolled individuals were representative of the general population. The samples were anonymized, labelled with barcode stickers (including institution number, sex, age, specimen type and collection date information) developed for this study and stored at −20°C until delivery to the central laboratory (Kangbuk Samsung Hospital).
Laboratory methods
To differentiate between immune responses induced by infection and vaccination, two types of immunoglobulin G antibodies against SARS-CoV-2 were assessed (Fig. 1).16 Anti-S and anti-N antibodies were measured using the Roche Elecsys anti-SARS-CoV-2 S immunoassay kit and Elecsys® Anti-SARS-CoV-2 assay kit (Roche Diagnostics, Rotkreuz, Switzerland), respectively in the sera of 5,000 individuals using Cobas® e801 analyzer (Roche Diagnostics GmbH, Mannheim, Germany). The cut-off value for anti-S antibody was ≥ 0.80 U/mL, and the cutoff index for anti-N antibody was ≥ 1.0 cut-off index (COI). The sensitivity and specificity of the anti-S antibody were 98.8% (98.1–99.3%) and 99.98% (99.91–100.0%), respectively. For the anti-N antibody, the sensitivity and specificity of the anti-N antibody were 99.5% (97.0–100.0%) and 99.8% (99.69–99.88%), respectively.17
During the pandemic period, performing real-time RT-PCR testing for SARS-CoV-2 was mandatory for COVID-19 confirmation, asymptomatic individuals screening, and differential diagnosis in South Korea and all the data were reported to Korea Disease Control and Prevention Agency (KDCA).1 Therefore, the sampling using nasopharyngeal swabs and the interpretation of the test results were based on molecular tests that targeted two or more sites of the viral genome—e.g., the PowerCheck 2019-nCoV kit, Kogene Biotech, Seoul, Korea, which targets the E and RdRp genes; and the DiaOlexQ 2019-nCoV kit, SolGent, Daejeon, Korea, which targets orf1a and N genes, etc.— and consider the test positive only when all targets were positive. These guidelines were strictly adhered to the recommendations from the Korea Society of Laboratory Medicine and KDCA.31819
Statistical methods
In each survey round, we determined seroprevalence estimates for SARS-CoV-2 infection and vaccine-induced seropositivity by age groups. The formula used for the estimated seroprevalence was prevadj
= (prevobs
+ Sp
– 1)/(Se
+ Sp
– 1). The unadjusted seroprevalences of anti-N and anti-S antibodies were determined by dividing the number of positive specimens by the total number of tested specimens. We calculated the sampling weights by weighing the samples from each age group stratum relative to the assigned population. Finally, we adjusted the diagnostic tool results because combining multiple estimated parameters is necessary for seroepidemiological studies owing to the operational characteristics of the diagnostic tools. We used the bootComb R package to estimate the SARS-CoV-2 seroprevalence, adjusted for test sensitivity and specificity in addition to the abovementioned formula. This R package using bootstrap sampling method was developed to estimate the seroprevalence of SARS-CoV-2 considering the sensitivity and specificity of serologic testing. Estimating confidence intervals (CIs) considering test sensitivity and specificity requires distribution calculation of several parameters. The BootComb R package derived 95% CIs using the highest density interval for the adjusted prevalence parameters.2021
To compare the seroepidemiological findings with the cumulative incidence based on the officially confirmed cases by RT-PCR in the capital metropolitan population, we employed official COVID-19 data provided by the KDCA.1 We obtained the number of confirmed SARS-CoV-2 infections in the capital metropolitan area by age and period from the COVID-19 dashboard of the KDCA.1 We divided the number of cases in each age group using the official population data from the South Korean capital metropolitan area for 2022.15 Finally, we calculated the number of cases per 1,000 community members and compared the results with the seroepidemiological results.
Ethics statement
The study protocol was approved by Institutional Review Boards (IRB) of Samsung Medical Center (IRB No. SMC 2021-12-072-001), Kangbuk Samsung Hospital (KBSMC 2021-12-028-004), International St. Mary’s Hospital (IS21TNME0094) and Dongguk University Medical Center (DUIH 2021-12-013). The requirement for informed consent was waived by the IRB.
RESULTS
SARS-CoV-2 seroprevalence
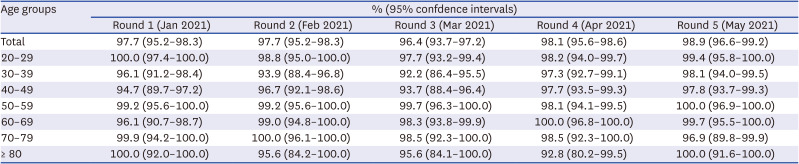
The anti-S seropositivity rates were remarkably high, ranging from 92.8% to 100.0% across all age groups over the five survey rounds of surveys conducted from January 2022 to May 2022 (Table 1). Interestingly, the 30–39 years and 40–49 years age groups had lower anti-S seropositivities compared to other age groups during the first three surveys (96.1% and 94.7% in the first, 93.9% and 96.7% in the second, and 92.2% and 93.7% in the third, respectively), but reached nearly 97% to 98% from the fourth survey, similar to the other groups.
Table 1
Anti-S seropositivities and 95% confidence intervals during the five survey rounds (from Janurary 2021 to May 2021) across age groups
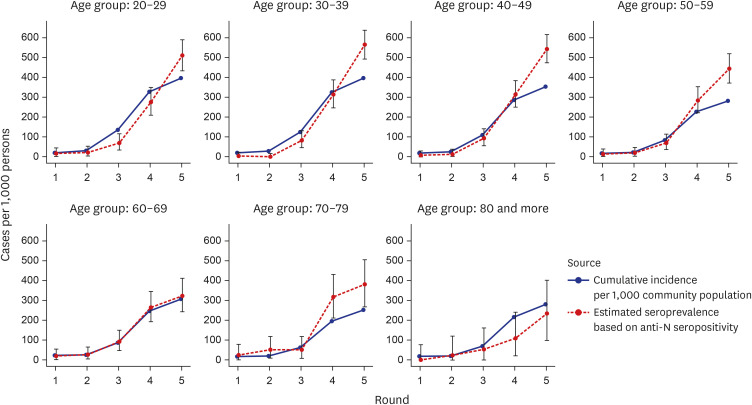
The anti-N seropositivity rates showed a substantially increasing tendency across all age groups over the five survey rounds and coincided with an increased cumulative incidence based on RT-PCR-confirmed cases from January 2022 to May 2022 (Fig. 3, Supplementary Table 2). In the fifth round, the anti-N seroprevalence was higher in all age groups except for the group aged > 80 years. In particular, both the cumulative incidence based on RT-PCR-confirmed cases per 1,000 community members and the estimated seroprevalence based on anti-N seropositivity increased in the fourth and fifth surveys, which correspond to April 2022 and May 2022, the period of the SARS-CoV-2 omicron surge. The result of anti-N and anti-S seropositivities observed in each institution and distribution of combined anti-N and anti-S seropositivities in 5,000 study individuals from January 2021 to May 2021 is shown in Supplementary Tables 3 and 4.
Comparison of SARS-CoV-2 infection rate based on serologic tests
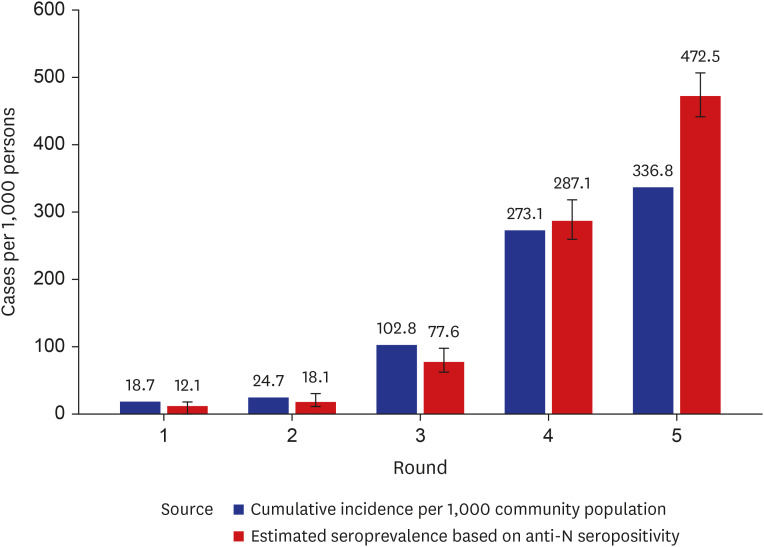
The overall estimated seroprevalence based on anti-N seropositivity was lower than the cumulative incidence based on RT-PCR testing per 1,000 people in the capital metropolitan area. The results indicated that seroprevalence was comparable to the PCR-confirmed cumulative incidence during the first three surveys but exceeded the PCR-confirmed cumulative incidence from the fourth round onwards. In the fifth round, a larger gap was observed between the reported cumulative incidence and estimated anti-N seropositivity-based prevalence (472.5/1,000 persons vs. 336.8/1,000 persons) (Fig. 4). Thus, the proportion of concealed cases reached 13.6% in May 2022. Supplementary Table 2 shows the 95% CI for the fifth round (May 2021) to be 441.56–506.79.
Fig. 4
Estimation of SARS-CoV-2 infection occurrence per 1,000 community population by comparing the cumulative incidence based on real-time polymerase chain reaction positivity and the estimated seroprevalence based on SARS-CoV-2 anti-N seropositivity.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, N = nucleocapsid.
DISCUSSION
By conducting a meticulously designed population-based seroprevalence study, we obtained a realistic estimate of humoral immune responses elicited by vaccination and natural infection with SARS-CoV-2 during the most active pandemic surge period in South Korea. Our investigation was conducted during the peak transmission period of COVID-19 in the country while at least two doses of vaccination were completed by the majority of individuals. This seroepidemiologic survey enabled the identification of unconfirmed COVID-19 cases that were either asymptomatic, undiagnosed, or under-reported and the evaluation of the extent of infection spread in the community.
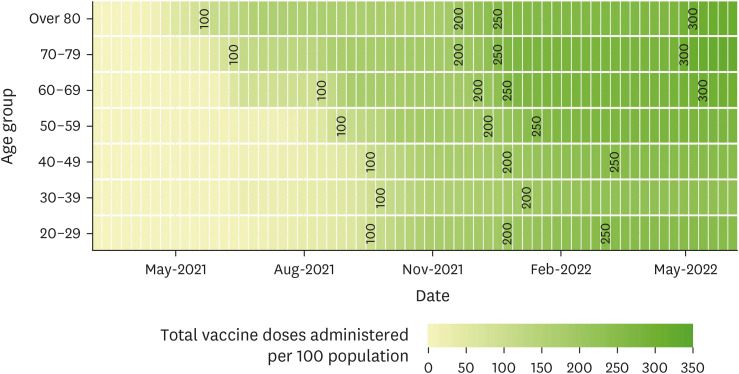
The high anti-S seropositivity rates observed in this study indicated high vaccine responses across all age groups. In South Korea, vaccinations for high-risk groups, including people above 65 years started between February to May 2021, and the vaccinations for the rest of the age groups started in July 2021. The second dose of vaccination was administered on an average of a month after the first dose.22 Therefore, by the time this survey was initiated in January 2022, most individuals had received a second dose. As shown in Fig. 5, between November 2021 and February 2022, persons across all age groups fell within the 200–250 range. Because the third dose of vaccination was continued afterwards, high anti-S seropositivity was maintained throughout the survey period. The increased anti-S seropositivity mirrored the vaccination policy in South Korea, as older individuals were prioritized and gradually expanded to include younger individuals.
Fig. 5
Cumulative vaccine doses administered per 100 persons in South Korea from May 2021 to May 2022. The numbers 100, 200 and 300 refer to the 1st, 2nd, and 3rd doses of vaccination, respectively.
The positive correlation between the extent of vaccination coverage and anti-S positivity has been observed in SARS-CoV-2 antibody surveillance studies conducted in other countries. In Spain, when 1,461 inhabitants of Navarre were studied for the presence of anti-S antibodies in May 2022, 92.7% were seropositive, which was consistent with the 91% vaccination coverage in the region.23 In Canada, when 149,522 blood donors were screened between January and November 2021, anti-S seroprevalence also corresponded with the roll out of vaccines targeting oldest to youngest, as well as reaching 100% seropositivity by November 2021.24
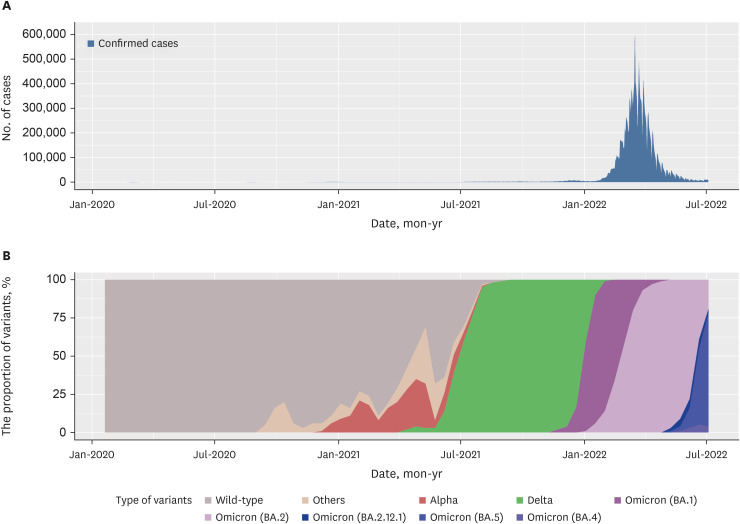
Anti-N seropositivity rates showed a substantially increasing trend across all age groups during the five survey rounds. Given that the highest number of COVID-19 confirmed cases in South Korea occurred in April 2022 (Fig. 6A), mainly due to the omicron (BA.2) variant (Fig. 6B), anti-N seropositivity essentially reflected humoral immunity due to natural infection. This observation was similar to that of the anti-N seroprevalence survey conducted during an overlapping period in the United States,25 where there was an increase in the infection-induced seroprevalence percentage from January 2022 to February 2022 in all age groups from 0 to over 65 years. The distribution of the omicron variant and the speed of spread was comparable to our results and coincided with an increased cumulative incidence of RT-PCR-confirmed cases from January 2022 to May 2022. The anti-N seropositivity rates across all age groups exhibited an increasing trend during the survey periods.
Fig. 6
Nation-wide status of COVID-19 infection in South Korea during the pandemic. (A) Number of confirmed COVID-19 cases in South Korea. Data from ‘Daily and cumulative number of confirmed cases’ in Cases in Korea, Korea Disease Control and Prevention Agency (https://ncov.kdca.go.kr/en/bdBoardList.do). (B) Proportional distribution of SARS-CoV-2 variants in analyzed sequences from January 2022 to May 2022. Data from Global Initiative for Sharing All Influenza Data (https://covariants.org/per-country?country=South+Korea.
COVID-19 = coronavirus disease 19, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
In particular, we observed that the estimated seroprevalence based on anti-N antibodies started to outnumber the cumulative incidence per 1,000 community members based on RT-PCR confirmation in the fourth round, which might reflect the concealed, or hidden, cases of infection. This reversal of two rates became bigger in the fifth round and the prevalence of anti-N antibodies increased from 12.1 cases per 1,000 individuals in the first round to 472.5 cases per 1,000 individuals in the fifth round. Moreover, they were generally higher in the younger groups than in the older groups. Although the discrepancy between the estimated seroprevalence and the cumulative incidence might be influenced by intrinsic factors such as sampling issues, differences in the definition of the two parameters, and duration of antibody retention, it is plausible that the discrepancy represents a population of concealed infection cases, mainly due to asymptomatic individuals who were not subject to the test-trace-isolate-quarantine strategy of KDCA to control the spread of infection. Yoon et al.,11 who conducted a relatively large seroprevalence study, suggested that the infection control strategy of RT-PCR screening seemed to be effective and the rate of undetected cases was low; however, it was performed from January to March 2021, which was before the active spread of the delta and omicron variants in Korea (Fig. 6B). Actually, a recent Korean study performed in a large scale including 9,945 individuals across 258 communities in August 2022 has reported the proportion of unreported infections among all COVID-19 infection as high as 33.9%.26 The detection of anti-N positivity not only reveals hidden infection cases at the population level but also confers the potential establishment of hybrid immunity.2327 Hybrid immunity, which refers to a combination of vaccine-induced and natural immunity, offers better protection against subsequent COVID-19 than either vaccination or infection alone.272829 The effectiveness of hybrid immunity may eventually contribute to controlling COVID-19.
The present study presented has certain limitations that must be considered. First, samples were collected from individuals who visited outpatient clinics or healthcare centers of general hospitals, were relatively healthy, or had mild symptoms. This may have introduced a bias by recruiting health-conscious individuals rather than a representative sample of the general population. Consequently, it might have affected the lower estimated seroprevalence based on anti-N seropositivity than the cumulative incidence per 1,000 community members during the first to third rounds of surveys in younger age groups (20–29 years and 30–39 years). Second, the sensitivities and specificities of the anti-S and anti-N antibodies used in this study were based on the assumption that the window period for antibody formation had passed after vaccination or SARS-CoV-2 infection. Third, the 95% CIs calculated using the bootComb R package were based on the assumption that all the parameter estimates were independent. This has the drawback of making the 95% CIs too wide if the independence assumption is violated. However, given the large sample size used in this study, these parameters were largely negligible.20 Lastly, the actual incidence per 1,000 community population may be underestimated in cases of which anti-N may no longer be detected, given that anti-N persists for five to seven months in the bloodstream. Also, the cumulative incidence per 1,000 community population based on RT-PCR results may be overestimated than the actual incidence per 1,000 community population because reinfection cases have been calculated as two separate events in the RT-PCR results retrieved from the KDCA data.
In summary, our study provided realistic estimates of the spread of SARS-CoV-2 during the most active pandemic surge period in South Korea. Specifically, we demonstrated evidence of a remarkably high response to vaccination and the detection of hidden infections that were underestimated by PCR testing-based surveillance strategies. These seroprevalence surveys are crucial for comprehending the significance and duration of humoral immunity and can ultimately provide appropriate public health guidance for achieving population-level immunity.
 XML Download
XML Download