

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Effective antiviral agents have played a significant role in the management of chronic hepatitis B (CHB) infection.12 Since the introduction of potent nucleos(t)ide analogs such as entecavir and tenofovir, the treatment landscape for CHB has undergone remarkable progress. These antiviral agents effectively suppress viral replication, alleviate liver inflammation, and impede disease progression, thereby significantly reducing the risk of complications such as cirrhosis, liver failure, and hepatocellular carcinoma (HCC).345 As a result, it can be anticipated that the epidemiology of hepatitis B has undergone significant changes compared to the past.67 However, despite the gradual progress in combating hepatitis B, it remains a significant medical challenge in endemic regions and continues to be a major cause of HCC.89
The coronavirus disease 2019 (COVID-19) pandemic has had a significant impact on healthcare systems worldwide, affecting the delivery and accessibility of care for patients with chronic illnesses, including individuals with CHB.10 As healthcare resources were redirected to manage the COVID-19 outbreak, the availability and timely administration of antiviral agents for patients with CHB may have been disrupted, potentially resulting in suboptimal treatment outcomes.11 Furthermore, the COVID-19 pandemic has likely had multiple impacts on the epidemiology of CHB. Disruptions in routine immunization programs, diagnostic services, and treatment availability may have affected the prevalence and incidence of CHB. Moreover, changes in social determinants of health, including socioeconomic conditions, employment, and housing, may have influenced the risk factors associated with CHB infection and transmission.12 The pandemic may have also impacted the adherence of CHB patients to their treatment regimens due to various factors, including limited access to healthcare providers, financial constraints, or concerns about visiting healthcare facilities and contracting the virus.13
Therefore, this study aims to analyze nationwide cross-sectional data in a hepatitis B virus (HBV) endemic area, providing a comprehensive overview of the epidemiological changes and patterns of hospital utilization among patients with CHB over the past 15 years, including the COVID-19 pandemic. Understanding these changes and their impacts is crucial for healthcare providers, policymakers, and researchers in developing evidence-based strategies to ensure the continuity of care and enhance outcomes for CHB patients during public health emergencies.
METHODS
Data source
We used the claim data of National Health Insurance Service (NHIS) in Korea. The Republic of Korea operates a universal health coverage system with mandatory social health insurance. This system covers approximately 98% of the total population, and the number of patients claiming health insurance each year amounts to around 46 million, accounting for approximately 90% of the registered resident population. To examine the overall pattern of CHB changes over a span of 15 years, data from the Korean NHIS were collected for the years 2007, 2011, 2015, 2019, 2020, and 2021. Due to limitations in the NHIS data retrieval system, data retrieval until 2019 followed a reverse chronological order rather than continuous retrieval over the full 12-year period. Starting from 2019, data were obtained for three consecutive years to analyze the impact of COVID-19 on the treatment of patients with CHB, as the COVID-19 outbreak occurred towards the end of 2019.
The HBV group consisted of patients aged 18 years and above who had been diagnosed with CHB or any of its subcategories. The severity of liver disease was analyzed by subclassification into 1) cirrhosis, 2) decompensated cirrhosis, 3) HCC, and 4) liver transplantation. To compare the characteristics of CHB patients with the general population, the control group was defined as the general population without hepatitis B. The control group is not the concept of non-CHB patients who have visited a medical institution at least once, but rather the non-CHB population registered for health insurance eligibility. The control group of this study is the population with no CHB history in the current year among the population registered with health insurance in Korea. Therefore, even if populations who do not visit a medical facility can be included in the control group of this study. Propensity score matching (PSM) analysis was used to match the chronic HBV group with a 1:4 ratio to a control group with similar demographic characteristics. The adjusted variables used in PSM were age and sex. This analysis allowed for a comparison of medical costs, medication costs, number of hospital visits, comorbidities, and concomitant medications between the HBV group and the control group.
Definition
HBV was defined as a case with a diagnosis code of International Classification of Diseases 10th Revision (ICD-10) B18.0 or B18.1. Liver cirrhosis was defined by the presence of one of the following ICD-10 codes: K702, K703, K74, K766, or K767. Decompensated cirrhosis was defined as meeting two criteria: 1) having an ICD-10 code for cirrhosis, and 2) having one of the following: a procedure code (abdominal paracentesis [C8050], endoscopic treatment of esophageal or gastric varices sclerotherapy [Q7631], endoscopic treatment of esophageal or gastric varices ligation [Q7633]), a drug code (spironolactone [Anatomical Therapeutic Chemical {ATC} code: C03DA01], terlipressin [ATC code: H01BA04], other systemic hemostasis [ATC code: B02BX], somatostatin [ATC code: H01CB01], propranolol [ATC code: C07AA05]), or a diagnosis code (hepatorenal syndrome [K767], bacterial peritonitis [K658], hepatic failure [K729], esophageal varices with bleeding [I983], hepatic encephalopathy [K76.82]). HCC was defined by either the ICD-10 code C22.0 or the ICD-10 reimbursement benefit extension coverage code V193. Liver transplant was defined based on one of the following conditions: 1) cases with disease code Z944 and treatment code Q80, or 2) the ICD-10 reimbursement benefit extension coverage code V013. Additionally, we investigated whether antiviral treatment was administered, and the targeted drugs included tenofovir alafenamide, tenofovir disoproxil fumarate (DF), entecavir, besifovir, lamivudine, adefovir, telbivudine, clevudine, and peg-interferon alpha.
We assessed the presence of nine comorbidities based on ICD-10 codes, including cerebrovascular disease, coronary heart disease, diabetes, hyperlipidemia, hypertension, rheumatoid arthritis, osteoarthritis, fracture or osteoporosis, and chronic kidney disease. Additionally, comorbidity was evaluated using the Charlson Comorbidity Index. We also examined the use of 7 concomitant medications, which included anti-diabetic medication, dyslipidemia medication, anti-hypertension medication, osteoporosis medication, diuretics, systemic (oral or intravenous) corticosteroids, and nonsteroidal anti-inflammatory drugs (NSAIDs). Detailed definitions for each comorbidity and medication can be found in the Supplementary Tables 1 and 2.
Statistical analysis
Continuous variables were presented as means ± standard deviations, while categorical variables were expressed as proportions, unless otherwise specified. Differences between the groups were analyzed using Student’s t-test for continuous variables and χ2 test for categorical variables. PSM analysis was conducted to compare the hepatitis B group and the control group. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R version 3.2.3 (The R Foundation for Statistical Computing, Vienna, Austria, http://www.r-project.org). A two-sided P value < 0.05 was considered statistically significant.
Ethics statement
The study protocol was approved by the Institutional Review Board of Soonchunhyang University Bucheon Hospital (2023-03-004, date of registration: March 20, 2023), and it adhered to the ethical guidelines of the World Medical Association Declaration of Helsinki. Due to the retrospective nature of the study, the requirement for informed consent from individual subjects was waived.
RESULTS
Trends in the prevalence of hepatitis B patients
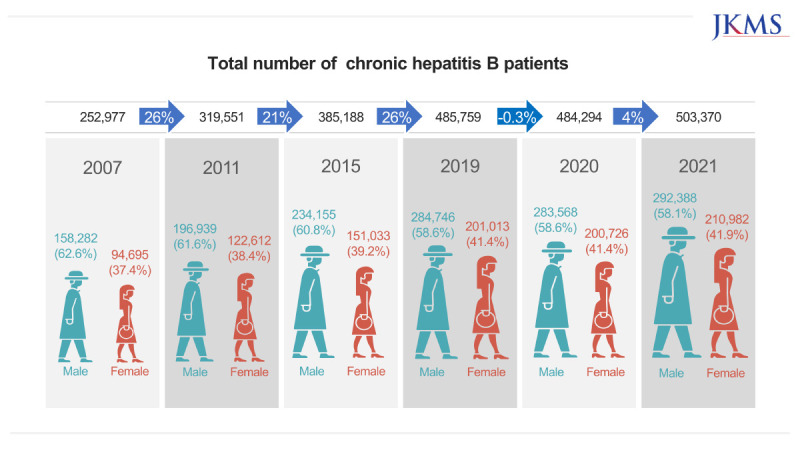
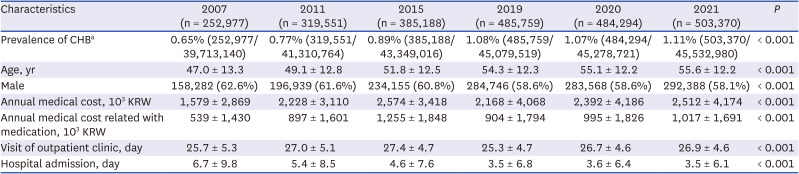
Table 1 displays the prevalence and total number of hepatitis B patients categorized by year. The number of patients with CHB consistently increased from 252,977 in 2007 to 319,551 in 2011, further rising to 385,188 in 2015, and reaching 485,759 in 2019. Examining the gender ratio (Table 1, Supplementary Fig. 1A), the proportion of males was 62.6% in 2007. Nevertheless, the proportion of males has continuously declined over time, reaching 58.1% in 2021 (P for trend < 0.001). Concurrently, the average age of hepatitis B patients continued to rise (Table 1). In 2007, the average age was 47.0 ± 13.3 years, whereas in 2021, it was 55.6 ± 12.2 years, reflecting a consistent increase over the span of 15 years. Analyzing the age composition ratio (Supplementary Fig. 1B), it is evident that the patient groups aged 55–64 years and 65 years or older experienced significant growth, while the group aged younger than 35 years decreased significantly each year.
Table 1
Demographics and characteristics of patients
Subsequently, the characteristics of the patients in the antiviral drug group were examined (Supplementary Table 3). The proportion of patients taking antiviral drugs steadily increased from 31.5% in 2007 to 52.3% in 2021. However, similar to the overall hepatitis B patient population, the proportion of males decreased over time. Additionally, the proportion of patients taking antiviral drugs increased among both men and women aged 55–64 years and those aged 65 years or older. Conversely, the proportion of patients taking antiviral drugs decreased in all patients under 35 years of age.
Medical expenditures and healthcare utilization in CHB
Compared to the control group, patients with CHB exhibited significantly higher medical costs (Fig. 1A, all P < 0.001). The annual per-person medical costs for CHB patients increased from 1,579 ± 2,869 (103 KRW) (equivalent to $1,179) in 2007 to 2,574 ± 3,418 (103 KRW) (equivalent to $1,923) in 2015. Subsequently, there was a decrease to 2,168 ± 4,068 (103 KRW) (equivalent to $1,620) in 2019. In 2021, medical costs began to rise again. Additionally, CHB patients experienced significantly higher medical costs related to medication compared to the control group (Fig. 1B, all P < 0.001). Similar to total medical costs, medication costs increased from 2007 to 2015, decreased in 2019, and increased in both 2020 and 2021.
Fig. 1
Healthcare resource utilization: total medical costs (A) and number of visits to medical institutions (B).
HBV = hepatitis B virus.
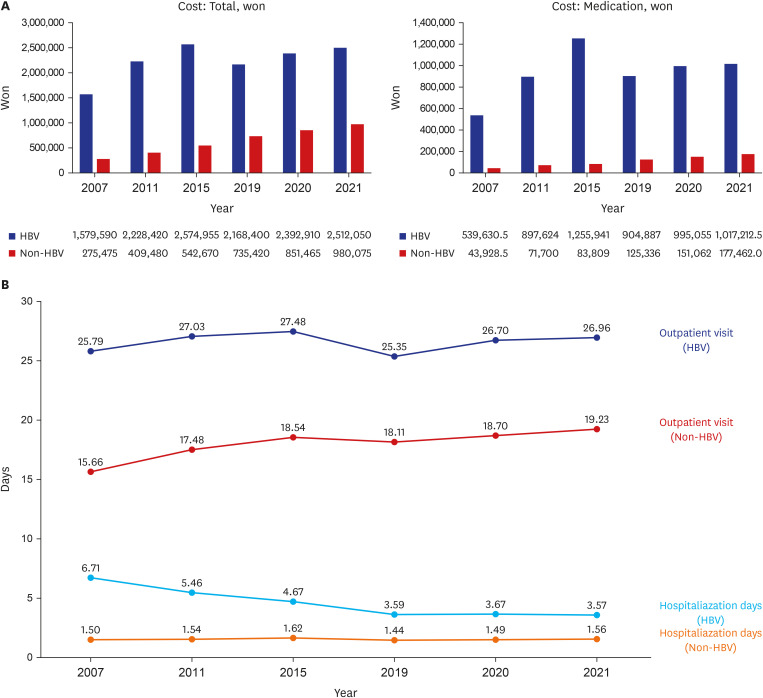
The use of medical facilities was analyzed by categorizing the number of outpatient visits and hospitalization days. CHB patients had a significantly higher number of outpatient visits and hospitalization days compared to the control group (Fig. 1B, all P < 0.001). Throughout the 15-year observation period, the number of outpatient visits for CHB patients remained relatively stable at an average of 26 visits per year. Conversely, the number of hospitalization days displayed a continuous decreasing trend, declining from 6.7 days in 2007 to 3.57 days in 2021.
Geographical variations in healthcare utilization by residential areas
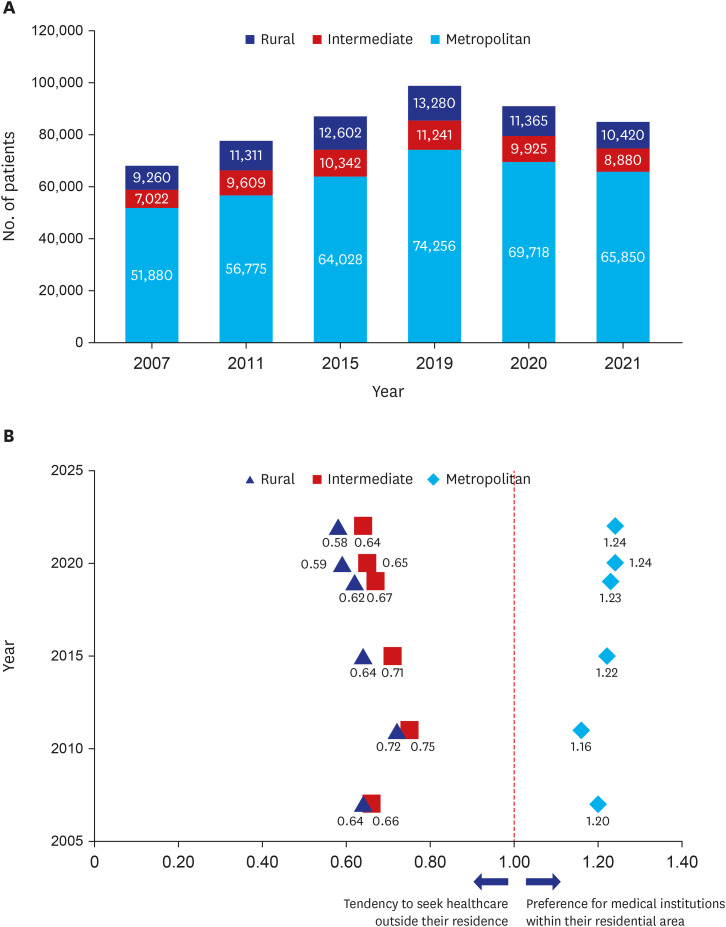
Subsequently, we conducted an analysis on the utilization patterns of medical institutions based on the patients' residential areas. The residential areas were classified into urban residents (Seoul, Gyeonggi-do, Incheon, Gwangju, Daegu, Daejeon, Busan, Ulsan), intermediate residents (Gyeongsangnam-do, Jeollabuk-do, Chungcheongnam-do), and rural residents (Gangwon-do, Gyeongsangbuk-do, Jeollanam-do, Jeju-do, Chungcheongbuk-do) based on the population distribution.
The majority of patients resided in metropolitan areas, followed by rural and intermediate areas (Fig. 2A). We then examined whether patients sought medical care within their residential area or opted for medical institutions outside their residential area (Fig. 2B). If the concentration factor exceeds 1, it indicates a preference for medical institutions within their residential area, while a factor below 1 suggests a tendency to seek healthcare outside their residence. Metropolitan residents demonstrated a higher likelihood of utilizing medical institutions within their residential area (concentration factor > 1), while intermediate or rural area residents tended to seek medical care outside their residential area (concentration factor < 1).
Subgroup analysis based on severity of liver disease: liver cirrhosis, decompensation, HCC, and liver transplantation
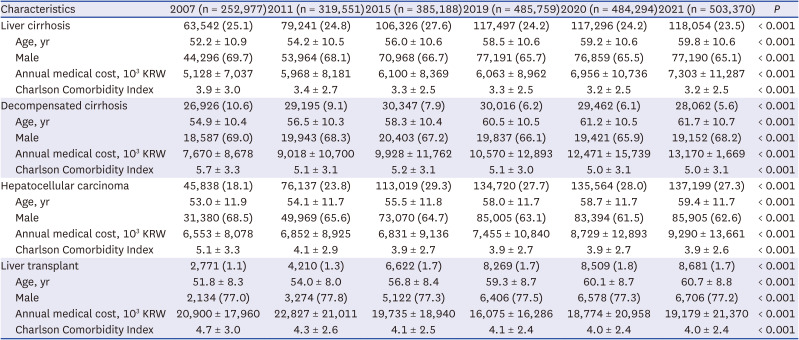
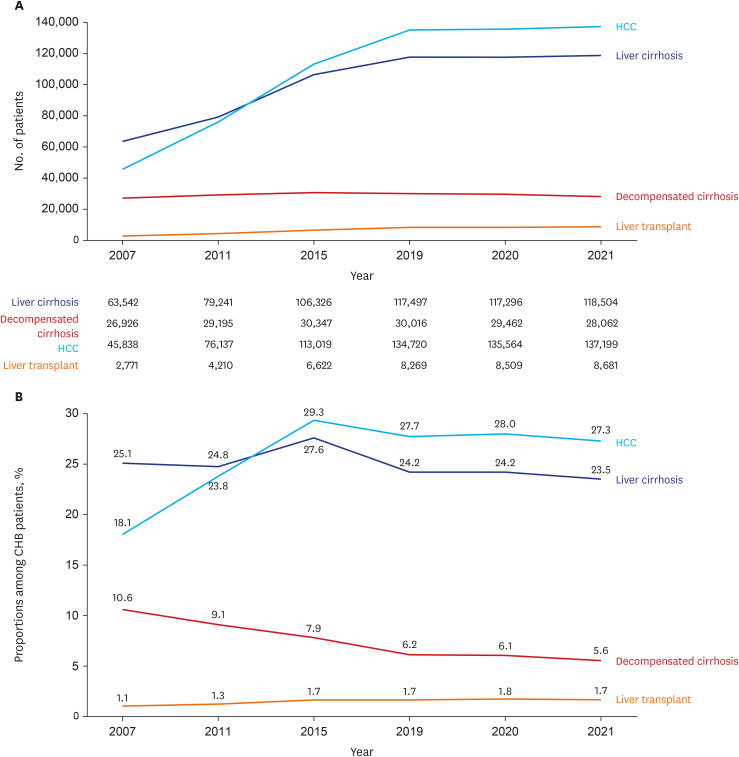
We conducted a subgroup analysis based on the severity of liver disease, including liver cirrhosis (all), decompensated cirrhosis, HCC, and liver transplant groups (Table 2). The number of patients in the liver cirrhosis, HCC, and liver transplant groups showed a continuous increase, while the number of decompensation patients began to decline from 2019 (Fig. 3A, P for trend < 0.001). Examining the proportions of each subgroup among all HBV patients, HCC, liver cirrhosis, and decompensation demonstrated a decreasing trend, whereas the proportion of liver transplants consistently increased (Fig. 3B). In terms of medical expenses and comorbidities, there was an increasing trend in medical costs following the order of liver cirrhosis, decompensation, HCC, and liver transplant. Additionally, the Charlson Comorbidity Index showed a significant increase.
Table 2
Characteristics and medical costs by severity of liver disease
Comorbidities and concurrent medications in patients with CHB
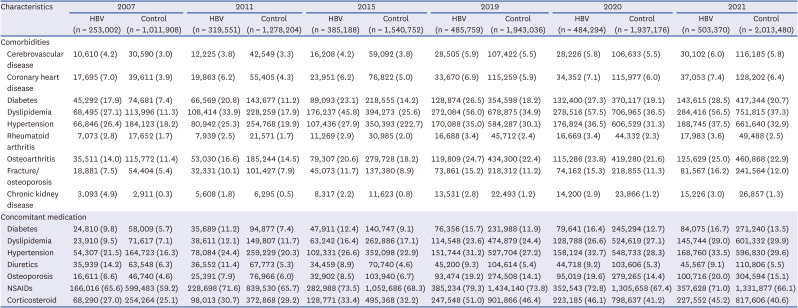
Comorbidities and concurrent medications of patients with CHB were analyzed in comparison to age- and sex-matched non-HBV controls (Table 3, Supplementary Fig. 2). In terms of comorbidities, the prevalence of cerebrovascular disease, coronary heart disease, diabetes, hyperlipidemia, hypertension, rheumatoid arthritis, osteoarthritis, osteoporosis or fracture, and chronic kidney disease was significantly higher in patients with CHB compared to the control group (all P < 0.001). Additionally, patients with CHB had a higher rate of taking concomitant medications, including antidiabetic, hypertension, osteoporosis, diuretics, systemic (intravenous or oral) corticosteroids, and NSAIDs, in comparison to the control group (all P < 0.001).
Table 3
Comparison of comorbidities and concurrent medication between the HBV group and the control group
Comparison before and during COVID-19 pandemic
During COVID-19 pandemic, the number of CHB patients slightly decreased to 484,294 in 2020, coinciding with the onset of the COVID-19. Additionally, compared to 2019, the prevalence of CHB decreased from 1.08% to 1.07% in 2020. A decrease in medical facility utilization due to COVID has been observed since 2019, and the total medical cost (2,574,955 won to 2,168,400 won) and number of outpatient visit days (27.48 days to 23.35 days) decreased in the HBV group. Other than this decrease in medical facility utilization patterns, the severity of the disease or comorbidities did not show any significant changes before and after COVID-19.
DISCUSSION
Through our study, we have gained insights into the changing trends in the prevalence, severity, medical costs, and comorbidities of CHB over a 15-year period in South Korea, which is considered an endemic region for HBV. Additionally, we have obtained valuable information on how the healthcare utilization by CHB patients has evolved during the COVID-19 pandemic.
The initial finding of our study challenges the common perception that CHB is gradually being overcome. Instead, we have observed a consistent increase in the number of CHB patients each year. It might be related with an increase in health checkups. To find out whether the increase in the number of hepatitis B patients was due to an increase in detection due to an increase in health checkups, we additionally investigated the number of people tested for hepatitis B surface antigen (Supplementary Table 4). From 2007 to 2021, the number of people tested for hepatitis B surface antigen was confirmed to increase overall. The second hypothesis is cohort effects. In the case of hepatitis B, a cure is rare, and cohort effects accumulate over several decades, contributing to the ongoing rise in the number of patients.1415 In other words, individuals born before 1992, when the hepatitis B vaccine was actively recommended, continue to exhibit a high prevalence of the disease due to the cohort effect. It was not until 2002 that the South Korean government initiated medical support for the hepatitis B vaccine, specifically targeting newborns.161718 Given that the positive rate of hepatitis B surface antigen remains notably high among individuals in their 30s to 60s (30s: 3.0%; 40s: 3.3%; 50s: 5.0%; 60s: 4.4%), we anticipate that this cohort effect will persist for at least another 30 years into the future.6 Furthermore, the rise in hepatitis B prevalence could be attributed to the increasing number of North Korean defectors and foreign workers (such as those from China and Mongolia) who have a higher prevalence of hepatitis B compared to South Koreans.1920 Therefore, despite the declining HBsAg positivity rate, it is imperative to maintain ongoing public health concerns and research pertaining to hepatitis B.21
The second significant finding of our study is the changing global characteristics of hepatitis B patients. Historically, a substantial proportion of patients with CHB were middle-aged men in their 50s and 60s. However, we have observed a declining trend in male dominance, and similar to hepatitis C, there has been a rapid increase in the number of patients aged 65 years or older. This shift indicates a shift in the demographics of hepatitis B patients. The observed increase in the average age of hepatitis B patients can be interpreted as a collective decrease in the severity of liver disease. This can be attributed to the availability of effective antiviral drugs and an improvement in the prognosis of individuals with hepatitis B. These factors might have contributed to an overall improvement in the management and outcomes of hepatitis B patients.2223 With the increasing number of elderly patients and improving prognosis of HBV, clinicians need to prioritize the aspects of quality of life. It is crucial for clinicians to be prepared to address the needs of elderly patients with CHB who often have comorbidities and require multiple concomitant medications. Specifically, given the higher prevalence of renal dysfunction and osteoporosis among CHB patients compared to the control group, careful consideration is necessary when selecting antiviral treatments.24 Another notable change in patients with CHB is the declining the proportion of decompensated cirrhosis, and this might be related with effectiveness of antiviral therapies.2526 This can be inferred from the decreasing proportion of decompensation patients, as well as the rates of liver cirrhosis and hospitalization days.27 However, it is essential to note the increasing incidence of HCC and liver transplantation. We think that there are some putative reasons to explain the increasing number of HCC among CHB since the effective antiviral therapy was introduced. Age is well-known risk factor of HCC. If more patients with CHB could survive longer, more patients could have a chance to have HCC. Also, the early diagnosis and more sophisticated treatment for HCC might lead to longer survival of HCC patients, which might attribute the increase or maintenance of the number of HCC forward.
The third significant finding of our study pertains to the medical costs associated CHB patients. Notably, a considerable portion of the medical expenses incurred were attributed to the costs of antiviral drugs. In contrast to the control group, the overall medical costs for the CHB group showed a decline between 2015 and 2019. This reduction can be attributed to the introduction of generic drugs like tenofovir DF or entecavir after the expiration of the patent period, leading to a decrease in the overall drug prices. Although patients with CHB exhibited higher medical costs compared to the control group, the majority of these costs demonstrated a significant surge following the development of decompensated cirrhosis or HCC.28 Given the recent surge in the use of costly antiviral medications, which often require long-term administration, there is a potential for further escalation in medication costs. However, considering the significant reduction in the incidence of HCC and complications related to cirrhosis due to the use of these drugs, it can be concluded that the active use of antiviral medications is cost-effective when considering the overall disease progression.29
Lastly, the present study showed the potential impact of the COVID-19 pandemic on changes in healthcare utilization patterns among CHB patients. Among them, both the number of outpatient visits and overall medical costs significantly decreased during the COVID-19 pandemic compared to the control group. Several factors may explain this finding. First, South Korea, with its relatively small land area and a national medical insurance system that is affordable and accessible, had limited adoption of telemedicine and remote care compared to Western countries during the COVID-19 pandemic. Second, healthcare systems had to prioritize essential services during the pandemic, resulting in the postponement or cancellation of non-urgent medical procedures and consultations.30 This likely caused delays in routine liver monitoring, imaging, and other elective procedures for CHB patients. To ensure that CHB patients receive appropriate care and support throughout future endemic situations, it is crucial for healthcare providers to monitor and adapt to these changes effectively.
In conclusion, the number of CHB patients in South Korea continues to increase annually. The patient population is aging, and the dominance of males among CHB patients is gradually declining. CHB patients experience higher medical costs, medication costs, outpatient visits, and longer hospitalization days compared to the control group, particularly as the disease progresses to cirrhosis and HCC. Furthermore, the CHB group exhibits a higher prevalence of comorbidities and greater medication use compared to the control group. Fortunately, effective antiviral treatment has led to a gradual reduction in the severity of liver disease among CHB patients. During the COVID-19 pandemic, the CHB patient group experienced a significant decrease in the number of visits to medical institutions, but there were indications of a slow recovery. Future research should focus on understanding the long-term implications of these changes on disease progression, management strategies, and health outcomes for CHB patients.
 XML Download
XML Download