

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is the third most common cancer in terms of incidence and the second leading cause of cancer-related deaths worldwide.1 In 2020, the Republic of Korea (hereafter, Korea) had the third-highest CRC incidence and mortality rates in the world, at 54.3 and 17.4 per 100,000 people, respectively.23 In most cases, premalignant or malignant lesions are asymptomatic for a prolonged period; therefore, the stage at diagnosis is critical to the prognosis.4 CRC screening plays a crucial role in detecting precancerous lesions or early-stage CRC,5 and reducing CRC mortality by up to 25%.6
To address the growing burden of cancer, the World Health Organization has recommended the establishment of National Cancer Control Plans that focus on prevention, early detection, diagnosis, treatment, and palliative care.7 In 1999, the Korean government launched the National Cancer Screening Program (NCSP) as a component of the comprehensive 10-year National Cancer Control Plan initiated in 1996.8 As per this program, CRC screening is conducted for individuals aged 50 years and older, primarily via an annual fecal occult blood test (FOBT). The NCSP is a population-based, organized CRC screening program that provides annual FOBTs for adults aged 50 years and older. Since 2004, the NCSP has also offered colonoscopy or a double-contrast barium enema test to individuals who show positive FOBT results.9 Although the CRC screening rate in Korea has increased from 25.7% in 2012 to 40.3% in 2021, it remains the lowest compared with the screening rates for cancers of the stomach, liver, lung, breast, and uterine cervix in 2021.10 This is a concerning issue, given that CRC is the third most common cancer globally and domestically, and early detection through CRC screening is critical for successful treatment and improved outcomes. Another salient issue is whether CRC screening can be sustained over time. Vernon conducted a comprehensive review of several studies on adherence to FOBT and found that it was challenging to achieve an annual compliance rate of over 50% among the general population.11
Understanding the factors that influence adherence to CRC screening over a long-term period is crucial for enhancing the regular uptake rate of CRC screening and improving CRC prognosis. Previous research conducted in Korea on the uptake of CRC screening and its determinants revealed that numerous factors, such as age, income, educational level, residential area, occupation type, marital status, and family history of CRC, have contributed to gradients in the CRC screening rate.1213141516 These studies utilized data from the Korean National Health and Nutrition Examination Survey (KNHANES) and Korea National Cancer Screening Survey, employed a cross-sectional design involving self-reported questionnaires, and captured the rate of CRC screening uptake at a single time point. It is challenging to obtain information on the regular uptake of CRC screening over a long period. The prevalence of benign tumors or precancerous lesions in the colorectal area can be a crucial determinant of the need for CRC screening. However, obtaining this information from cross-sectional survey data is nearly impossible. Therefore, to investigate the various factors influencing the regular uptake of CRC screening over an extended period, we utilized individual-level linked data from three public health databases for a period of 12 years: the Korean Disease Control Agency (KDCA), the Korean National Health Insurance Service (KNHIS), and the Korean Health Insurance Review and Assessment Service (KHIRA).
METHODS
Data source and study population
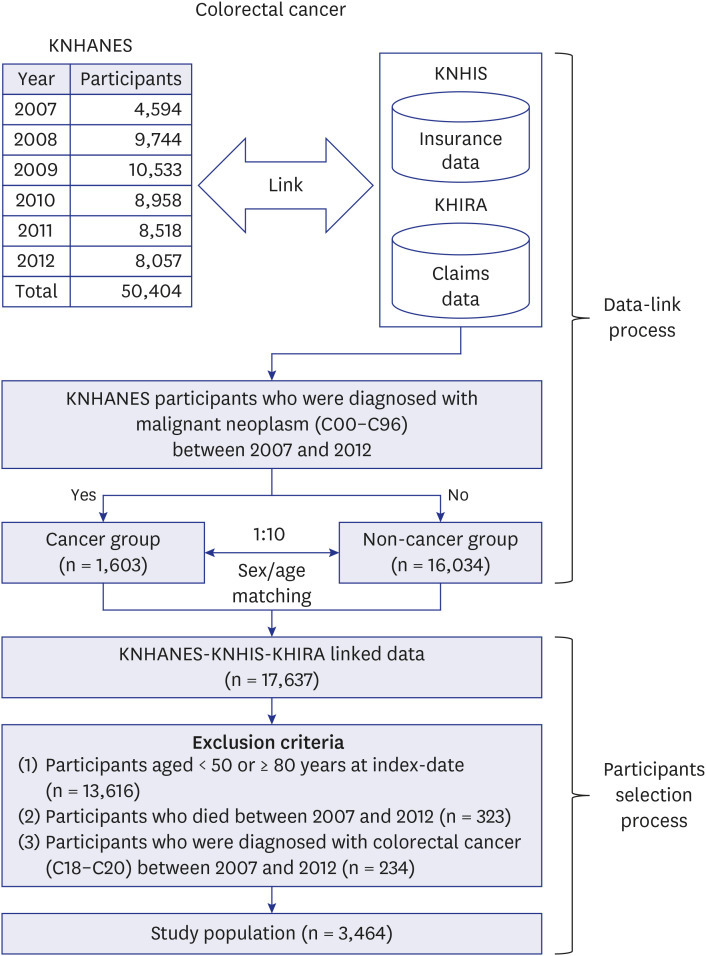
In 2019, the Korean National Evidence-based Healthcare Collaborating Agency (KNECA) initiated a healthcare data linkage project that integrated individual-level data from multiple sources, including the KDCA, KNHIS, KHIRA, and the Korean National Cancer Center. In our study, we used individual-level data from three sources: 1) KNHANES data from the KDCA, 2) information on CRC screening uptake and insurance from the KNHIS, and 3) claims data from the KHIRA. We received data from the KDCA on 50,404 respondents to the KNHANES from 2007–2012 and linked it to CRC screening and insurance data from the KNHIS and claims data from the KHIRA at the individual level.17 Each participant with malignant neoplasms (Korean Standard Classification of Diseases [KCD] codes C00–C96) from the KHIRA database between 2007 and 2012 was selected by KNECA and matched by sex and age to 10 KNHANES participants without malignant neoplasms. A total of 17,637 of 50,404 participants in the 2007–2012 KNHANES were included: cancer group (n = 1,603) and non-cancer group (n = 16,034). A total of 3,464 from 17,637 participants in the 2007–2012 KNHANES aged 50–79 years were selected as the study population and included in the final analysis. Three exclusion criteria were applied: 1) age < 50 or ≥ 80 years at index-date (January 1, 2007) (n = 13,616), 2) death between 2007 and 2012 (n = 323), and 3) diagnosed with CRC (KCD codes C18–C20) between 2007 and 2012 (n = 234). The process of data linking and sample selection is shown in Fig. 1.
Fig. 1
Flow diagram of the recruitment process of the study participants.
KNHANES = Korean National Health and Nutrition Examination Survey, KNHIS = Korean National Health Insurance Service, KHIRA = Korean Health Insurance Review and Assessment Service.
The KNHANES contains participants’ unique socioeconomic information, such as household income, education, marital status, and private health insurance status, that is impossible to obtain from the KNHIS and KHIRA. The KNHIS provides unique and important information about participants having undergone a public CRC screening service, treated as an outcome variable, disability condition, and family history of CRC. The KHIRA records data on factors associated with CRC screening such as inflammatory bowel diseases (IBDs), e.g., ulcerative colitis and Crohn’s disease, benign neoplasms of the colorectal area, gastrointestinal bleeding, and changes in bowel habits. The process for deriving predictors and outcome variables from linked data sources including the KNHANES, the KNHIS, and the KHIRA, was elaborated in Supplementary Table 1.
Measures of main interest
Outcome variable
The outcome variable was the level of adherence to CRC screening, categorized into three ordinal groups: nonadherent, intermittently adherent, and consistently adherent. Adults who underwent CRC screening were operationally defined as those included in the 2007–2018 CRC screening data table obtained from the KNHIS database. If either the FOBT or colonoscopy was performed, CRC screening was considered complete for that year. The follow-up period for this study commenced on January 1, 2007, and concluded on December 31, 2018, with censoring performed for deaths and new CRC diagnoses. To account for the biennial uptake of CRC screening in Korea that was converted to annual uptake by the Korean Ministry of Health and Welfare in 2012,18 we tracked CRC screening data throughout the follow-up period. Specifically, we ensured that participants born in odd-numbered years underwent CRC screening in 9 years (i.e., 2007, 2009, 2011, 2013, 2014, 2015, 2016, 2017, and 2018), and those born in even-numbered years underwent screening in 9 years (i.e., 2008, 2010, 2012, 2013, 2014, 2015, 2016, 2017, and 2018). Since we excluded participants from the KNHANES who died between 2007 and 2012, we were able to guarantee the assessment of at least three CRC screenings. The participants were then categorized into three adherence groups based on their CRC screening history: nonadherent (no prior CRC screening), consistently adherent (participation in at least half of the CRC screening assessments), and intermittently adherent (did not meet the criteria for nonadherence or consistent adherence).
Medical conditions of affecting adherence to CRC screening
We generated four variables, namely gastrointestinal bleeding, changes in bowel habits, neoplasm of the colorectal area, and IBD, using claims data from the KHIRA. The four variables were based on the following KCD codes for which the patients required medical services: 1) gastrointestinal bleeding (KCD codes K55.21, K57.31, K57.53, K57.91, K62.5, K92.1, and K92.2), 2) changes in bowel habits (KCD code R19.4), 3) neoplasm of the colorectal area (carcinoma in situ of lower intestine with KCD codes D01.0, D01.1, D01.2, D01.3, and D01.4, benign neoplasm of colorectal area with KCD codes D12, D12.0, D12.1, D12.2, D12.3, D12.4, D12.5, D12.6, D12.7, D12.8, and D12.9), and 4) IBD (Crohn’s disease with KCD codes K50, K50.0, K50.1, K50.8, and K50.9 and ulcerative colitis with KCD codes K51, K51.0, K51.2, K51.3, K51.4, K51.5, K51.8, and K51.9).
Demographic data of the study sample
The KNHANES encompasses demographic data including sex, age, place of residence, and marital status. Age, as of January 1, 2007, was categorized into three groups: 50–59, 60–69, and 70–79 years. We compared the adherence to CRC screening in three distinct regions: metropolitan cities, small-to-medium-sized cities, and rural areas. The relative poverty line was used as an indicator of household income, defined as 50% of the median household income by household size provided annually by the Korea Statistics Office.19 Household income by household size was categorized in the KNHANES data as less than 50% (below the relative poverty line), 50% to < 100%, 100% to < 150%, 150% to < 200%, and ≥ 200%. Marital status was classified as unmarried, divorced (including separated), or married. Based on the International Standard Classification of Education,20 education levels were classified into the following categories: elementary school graduates or less, middle school graduates, high school graduates, and college graduates or higher.
The occupational categories in the KNHANES dataset were classified according to the Korean standard classification of occupations21 and grouped into three categories: manual workers (service workers; sales workers; skilled agricultural, forestry, and fishery workers; craft and related trade workers; equipment, machine operating, and assembling workers; and unskilled workers), non-manual workers (managers, professionals, and clerks), and others (armed forces, housewives, and students). Furthermore, the KNHANES dataset comprises information on current employment status (employed or not), shift work (performed or not), employee status (self-employed or employed by others), occupation position (regular, temporary, or daily), and working hours. Following the classification used in previous studies,222324 we categorized occupational classes into six types: high-level professionals and managers; low-level professionals; clerical, sales, and service workers; manual workers; self-employed entrepreneurs and farmers; and individuals who have never worked or fall into other categories. The KNHIS compiles disability registry data indicating the presence or severity of physical or mental disabilities based on the Korean Disabled Persons Welfare Act.25 The study population was categorized into disabled and non-disabled individuals. The National Health Insurance (NHI) in Korea provides coverage to approximately 97% of the country’s total population, whereas Medicaid is available for those in the lowest 3% income range. Health insurance types were categorized as Medicaid, self-employed NHI, or employment-based NHI. We extracted information on whether individuals received services from local public health organizations between January 1, 2007, and the endpoint for the KHIRA data. Local public health organizations include public health clinics, centers, and units and mother-and-child health organizations.26 The medical history of patients with any type of malignant cancer (KCD codes C00–C96), except for CRC (KCD codes C18–C20), was obtained from the KCD list of the KHIRA as well as from the self-reported cancer survey data in both the KNHANES and the KNHIS cancer screening data tables. Additionally, the family history of patients who underwent CRC was extracted from self-reported information in the KNHIS cancer screening data table.
Statistical analysis
Statistical analyses were performed using the R 4.0.0 software (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at P < 0.05. significant. All variables in this study were categorical variables and presented as frequencies and percentages in Table 1. The differences in predictor distributions among the three levels of adherence to CRC screening were examined by univariate analysis with χ2 test (Table 2). As the outcome variable of this study, adherence to CRC screening, was ordinal in nature, ordinary logistic regression27 was used to estimate the adjusted effect of predictors on compliance with CRC screening (Table 3).
Table 1
Distribution of variables in the study population by age groups
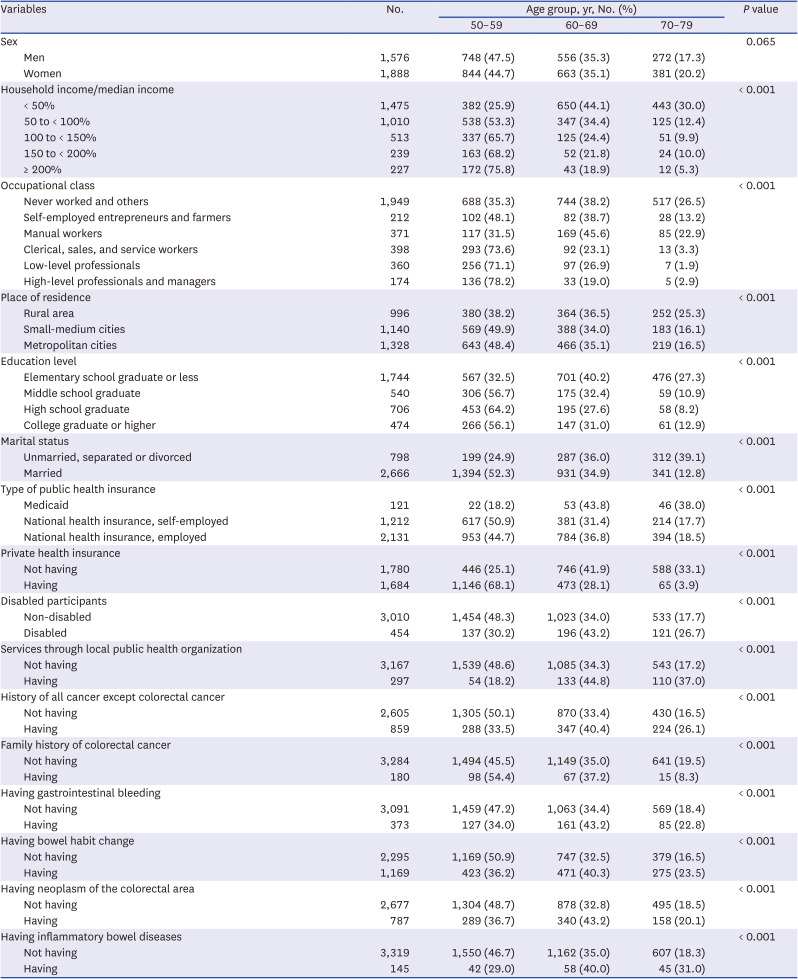
Table 2
Adherence level with colorectal cancer screening between 2007–2018
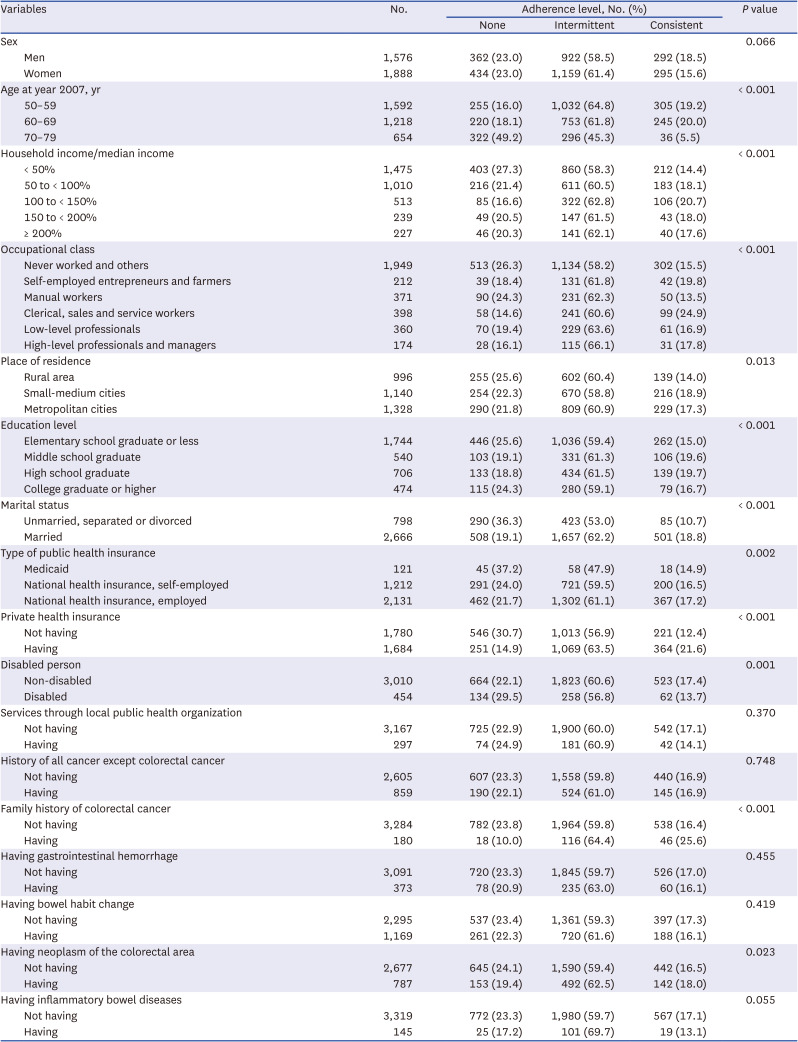
Table 3
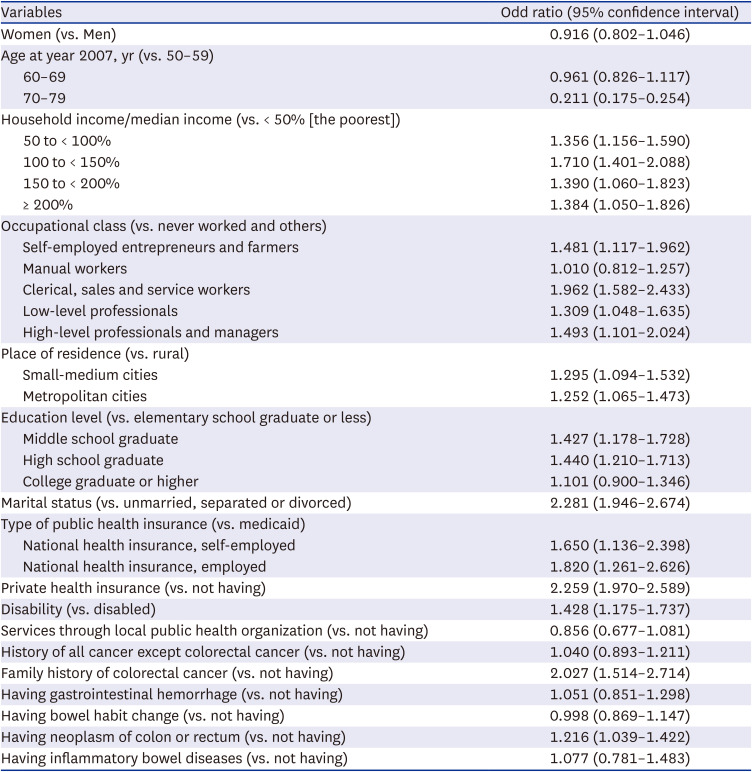
Adherence with colorectal cancer screening based on multivariate ordinal logistic regression
Ethics statement
The study protocol was approved by Konyang University’s Institutional Review Board (IRB) (IRB approval No. 2019-10-022) and the data linkage protocol was approved by the IRB of the KNECA (IRB approval No. NECAIRB20-016-1). The requirement for informed consent was waived by both IRBs because personal information that could identify the individuals was not used in this study.
RESULTS
Table 1 shows the distribution of predictors by age group, categorized as 50–59 years, 60–69 years, and 70–79 years. Among the participants, those aged 50–59 years, the youngest group, had the highest distribution in numerous socioeconomic categories including the highest household income (75.8%), highest occupational class (78.2%), residing in large cities (48.4%), having completed higher education (56.1%), being married (52.3%), having self-employed NHI (50.9%) and employed NHI (44.7%), having private insurance (68.1%), and having a family history of CRC (54.4%) (P < 0.001). The participants aged 60–69 years displayed the highest distribution in the following six categories: receiving services through local public health organizations (44.8%), having a medical history of any type of cancer except CRC (40.4%), being diagnosed with gastrointestinal hemorrhage (43.2%), bowel habit changes (40.3%), neoplasm of the colorectal area (43.2%), and IBD (40.0%).
Table 2 presents the distribution of adherence to CRC screening according to the predictors. All predictors, except sex, experience of visiting a public health center, having a medical history of any type of cancer except CRC, being diagnosed with gastrointestinal bleeding, bowel habit changes, and IBD, were found to be statistically significant (P < 0.05). Most predictor categories were observed in the intermittently adherent group. The following groups showed the lowest distribution of and statistical significance for consistent adherence to CRC screening: age group of 70–79 years (5.5%), lowest income (14.4%), manual workers (13.5%), living in rural area (14.0%), having completed the lowest education level (15.0%), unmarried or separated/divorced (10.7%), Medicaid (14.9%), no private health insurance (12.4%), disabled (13.7%), no family history of CRC (16.4%), and no medical history of colorectal neoplasm (16.5%).
Table 3 shows the results of the multivariate ordinal logistic regression analysis of CRC screening adherence according to the independent variables. The odds of regular screening were the lowest in the 70–79 age group (odds ratio [OR], 0.211; 95% confidence interval [CI], 0.175–0.254). The odds of adherence to regular CRC screening were the highest among those in the 100–150% income group (OR, 1.710; 95% CI, 1.401–2.088); clerical, sales and service workers (OR, 1.962; 95% CI, 1.582–2.433); those residing in medium-sized cities (OR, 1.295; 95% CI, 1.094–1.532); high-school graduates (OR, 1.440; 95% CI, 1.210–1.713), married participants (OR, 2.281; 95% CI, 1.946–2.674); participants with employment-based NHI (OR, 1.820; 95% CI, 1.261–2.626); privately insured participants (OR, 2.259; 95% CI, 1.970–2.589); non-disabled participants (OR, 1.428; 95% CI, 1.175–1.737); participants with a family history of CRC (OR, 2.027; 95% CI, 1.514–2.714); and participants with a colorectal neoplasm (OR, 1.216; 95% CI, 1.039–1.422).
DISCUSSION
Only 16.9% of the participants showed consistent adherence to CRC screening programs during the study (2007–2018). Adherence to cancer screening programs is an important public health issue. We considered that it is important to assess adherence to CRC screening not only at a single point in time, but also over a long period of time. Cross-sectional annual screening rates for CRC in Korea are low compared to other cancers and compared to other countries. In this study, we found that long-term adherence CRC screening is also significantly low. Since the inclusion of CRC screening in the NCSP in 2004, there has been an annual increase in participation rate of 3.3%. In 2017, the participation rate for CRC screening exceeded 40%.10 On the other hand, participation rates for screening for all other cancer types, except CRC, surpassed 40% in 2011.9 Despite a steady increase in CRC screening rates in Korea, these rates remain lower than those observed in other countries. In the United States, the CRC screening rate for individuals over 50 years of age was approximately 63% in 2015, and 60.3% of the participants were screened by endoscopy.28 Several European countries have implemented population-based organized CRC screening programs, with screening rates for fecal immunochemical tests exceeding 50% in countries such as the United Kingdom (55.4%), Finland (66.6%), the Netherlands (71.3%), Portugal (62.8%), and Sweden (60.2%).2930
Despite the dearth of evidence from long-term observational studies regarding routine participation rates in CRC screening, there are a few possible explanations for the < 50% CRC screening participation rates reported annually by the Korean government and < 20% distribution in the category of consistent adherence to CRC screening in this study. The first explanation is the high accessibility of colonoscopy. The NCSP does not offer endoscopy as the primary screening modality, allowing individuals to opt out of the NCSP and undergo private screening with colonoscopy at their own expense. Colonoscopy is a highly accessible and cost-effective option for CRC screening in Korea as many experienced endoscopists perform colonoscopies. This makes it relatively easy for individuals to undergo colonoscopy for CRC screening, provided that they are willing to cover the expenses.31 Another possible explanation is the lack of continuity of care. The strength of the primary care system in Korea has been reported to be the weakest among the Organization for Economic Cooperation and Development countries.32 The weakness of the primary care system can be partially attributed to the referral system lacking a gatekeeping function.33 Lasser et al.34 reported that general practitioners and family doctors significantly increased CRC screening rates through a gatekeeping function. Korea’s NCSP has an open certification system for cancer screening units without a mandatory gatekeeping function, meaning that many types of medical facilities, including primary care facilities, hospitals, and screening facilities, can be certified. Additionally, invitees from the NCSP for CRC screening can visit any certified screening unit. Therefore, the invitees experience a lack of continuity in CRC screening due to the lack of a close relationship with the physician at the screening unit, and this could negatively affect the rates of regular participation in CRC screening. The third possible explanation stems from the potential inconveniences associated with FOBT. Suh et al.9 suggested that the low participation rate in CRC screening could be attributed to the process of screening via FOBT, which is used as the primary screening test in the Korean NCSP. Individuals invited for CRC screening are required to collect stool samples at home and then visit a screening unit to submit the samples. This procedure typically involves two separate visits to the screening unit: the first to pick up the container, and the second to submit the sample. This process may present a challenge for sustained participation in CRC screening among the participants of this study.
As shown in Tables 2 and 3, this study provides evidence of socioeconomic inequalities in consistent adherence to CRC screening in Korea, and various socioeconomic factors have been identified as barriers to or facilitators of consistent participation in CRC screening. The lowest rates of consistent adherence to CRC screening were significantly distributed in groups with low socioeconomic status (SES) that included those aged 70–79 years, those residing in a rural area, unmarried participants (including those who were separated/divorced), those who were Medicaid beneficiaries, and those with a disability. A previous study35 explained the low participation rate in CRC screening among individuals of low SES. The study had identified several barriers to CRC screening among underserved populations, including lack of time to visit CRC screening facilities, insufficient knowledge about CRC screening, physical disabilities, and lack of accessibility to transportation services. This study revealed an intriguing finding of a reverse U-shaped pattern in the rates of consistent adherence to CRC screening among predictors with four or more categories, including household income, occupation, and education. The pattern observed in this study indicates that the rates of consistent adherence to CRC screening increased from the most underserved group to the less underserved group, and subsequently decreased up to the least underserved group. Cho et al.36 argued that Korean adults prefer colonoscopy over FOBT as a primary screening method owing to its accuracy and ability to provide therapeutic options and that individuals with high income levels tended to prefer colonoscopy. Moreover, similar to the findings of our study, Cho et al.36 demonstrated that the participation rates in CRC screening were lower among NHI recipients of high-income status than among those with low income status; this could be attributed to the possibility that NHIS recipients of high-income status opted to undergo colonoscopy through a private screening program instead of participating in the NCSP. Considering that income, education, and occupation are highly interrelated socioeconomic indicators, previous studies indicating that individuals with high income levels are more likely to undergo colonoscopies can be extrapolated to education and occupation. Two previous studies1237 have shown a significant positive correlation between private health insurance and regular participation in CRC screening. Individuals enrolled in private health insurance plans that cover cancer care services are more likely to continue CRC screening. Consequently, if patients are diagnosed with CRC, the financial burden of subsequent diagnosis and treatment costs would be reduced. Our study identified family history of CRC as a facilitator of consistent adherence to CRC screening. A previous study38 suggested that individuals without a family history of CRC may perceive themselves as being less susceptible to CRC, which can lead to low participation in CRC screening.
In addition to socioeconomic factors, this study examined several medical conditions that may affect CRC screening. We examined the relationships between CRC screening and gastrointestinal bleeding, changes in bowel habits, colorectal neoplasms, and IBD. Of the four factors, colorectal neoplasms were significantly associated with consistent adherence to CRC screening (OR, 1.216; 95% CI, 1.039–1.422). Colorectal neoplasms, represented by colorectal adenomas, are associated with CRC development. Most CRCs are thought to develop through a stepwise progression known as the adenoma-carcinoma sequence, in which normal colon tissue progresses from colorectal adenoma (a premalignant lesion) to colon cancer.39 After endoscopic resection of a colorectal adenoma, doctors typically explain to patients that adenomas are precancerous lesions and educate them on the importance of early detection and treatment to prevent CRC. Therefore, people who have been treated for colorectal neoplasms will be more likely to undergo cancer screening owing to their increased knowledge of CRC prevention than those who do not receive such treatments. A 2021 nationwide study conducted by the Korean National Cancer Center found that 80.3% of the participants believed that cancer is a preventable disease.40 This study demonstrates a high level of knowledge and interest in cancer among Koreans, and we expect a high level of interest in CRC among Koreans.
Conversely, participants with IBD were less likely to consistently adhere to CRC screening than those without IBD (13.1% vs. 17.1%, P = 0.055), suggesting that patients with IBD tended to be less likely to be screened for CRC, although statistical significance was not demonstrated. Because colonoscopy plays an important role in the differential diagnosis of IBD and is effective in assessing the response to treatment, patients with IBD frequently undergo colonoscopy.4142 In addition, IBD is associated with a high risk of dysplasia or malignancy and requires periodic surveillance colonoscopies.43 The American Society for Gastrointestinal Endoscopy and European Society of Gastrointestinal Endoscopy recommend that surveillance colonoscopy be performed 8–10 years after the onset of IBD.4445 Even in the remission period, surveillance colonoscopy should be performed every 1–5 years, depending on the patient’s individual risk factors, resulting in the need for frequent colonoscopies. Therefore, it can be expected that patients who have already had a colonoscopy for clinical purposes are unlikely to undergo FOBT-based CRC screening. There was no significant difference in the rate of consistent CRC screening between participants with a history of gastrointestinal bleeding or bowel habit changes and those without. Colonoscopy is recommended for diagnosing and treating gastrointestinal bleeding.46 However, periodic follow-up endoscopy is not recommended after full recovery from gastrointestinal bleeding; therefore, it can be assumed that this may not have affected the long-term CRC screening behavior. Changes in bowel habits can be a symptom of CRC; therefore, diagnostic colonoscopy is indicated.47 As with gastrointestinal bleeding, once a colonoscopy is performed to differentiate the cause of a change in bowel habits, follow-up examinations are not usually performed multiple times; therefore, it can be assumed that long-term examination behavior is not affected.
This study has several limitations. First, the findings of this study may not be representative enough to extrapolate to the entire population of Korea. The KCDA conducted the KNHANES with a total of 50,404 participants between 2007 and 2012 and produced representative health outcomes for the entire Korean population. Unfortunately, we received combined KNHIS and KHIRA data for only 17,637 KNHANES participants, accounting for approximately one-third of the 50,404 participants in the 2007–2012 KNHANES. Therefore, the findings of this study cannot be generalized to the entire Korean population. Second, similar to the limitations of other national data-based big data studies, our study was designed based on KCD codes, which leaves a lot of room for physician subjectivity in determining the codes, and therefore may not perfectly reflect the actual situation of the study subjects. This inconsistency has the potential to negatively impact the high reliability of the study. Third, despite the availability of both population-based and opportunistic CRC screening in Korea, the database employed in this study was not capable of capturing opportunistic screenings conducted outside the NCSP that involved undergoing a colonoscopy as the first screening test in CRC screening, skipping the FOBT. Therefore, it is impossible to determine regular participation in the overall CRC screening using data from public and private screening data. Fourth, it was difficult to identify the reasons for nonparticipation in CRC screening using the data obtained in this study. There is a need to explore the influence of psychological factors such as discomfort, concern about complications, and anxiety about the procedure. Fifth, this study is based on the KCD code and is a big data study linking multi-year data from multiple institutions. Therefore, due to the structural characteristics of the study, it was not possible to identify and evaluate in detail the timing of diagnosis and recovery of comorbid medical conditions that may affect CRC screening uptake. Sixth, this study was conducted as part of multi-institutional data linkage project of the KNECA, which involved a data link process and 1:10 matching of cancer patients to non-cancer patients. Therefore, there is the potential for selection bias that occurred before the data was available to the researchers. And, we excluded deaths and subjects diagnosed with CRC during the period 2007–2012. This was done to ensure a minimum of three assessments to assess consistent uptake of CRC screening, but this exclusion could also introduce selection bias.
Despite these limitations, this study is valuable because it examined the level of regular participation in CRC screening and various influencing factors through 12 years of retrospective follow-up observation by linking individual-level data from three public health databases. Additionally, the study examined whether a history of one of the four types of colorectal diseases, in addition to socioeconomic factors, influenced regular participation in CRC screening. Although the NCSP is designed to ensure CRC screening for all Koreans aged 50 years and older, the high accessibility of colonoscopy in Korea limits the ability of studies to identify the overall regular participation rates in CRC screening and its determinants using only NCSP data. Therefore, a longitudinal survey, such as a panel survey, is necessary to produce nationally representative estimates of regular participation in CRC and the influencing factors.
 XML Download
XML Download