

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
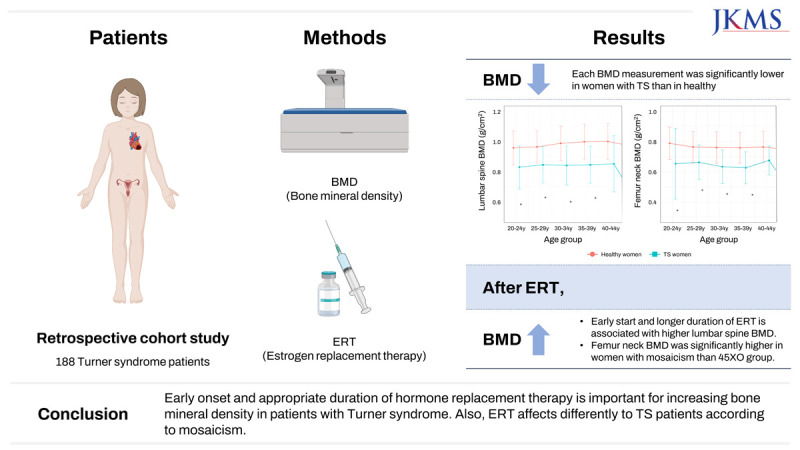
Turner syndrome (TS) is a common chromosomal abnormality that occurs in about 1 in 2,000 to 2500 surviving fetus and is caused by loss of all or part of one X chromosome. TS includes not only the typical 45, X karyotype, but also various mosaic karyotypes with structural abnormalities of the X chromosome, and clinical features differ according to these karyotypes.1
TS is diagnosed at around 15 years old on average but can be diagnosed at the intrauterine stage, childhood, adolescence, or adulthood. Clinically, TS is characterized by short stature and sexual infantilism and is accompanied by systemic disorders in major organs such as heart and kidney, with a high incidence of autoimmune diseases, osteoporosis, and bone fractures.23456 Unlike normal oocyte decline that continues for decades, it occurs within several months or years after birth in TS patients. Therefore, ovaries degenerate during the fetal stage, childhood, or adolescence and as a result, only 10–30% of TS patients undergo puberty naturally. TS patients without spontaneous pubertal development need estrogen supplementation to induce secondary sexual characteristics.78 Puberty plays an important role in sexual development normal growth, and acquisition of bone density. Since the peak bone mass formed at puberty is essential for protecting from bone loss due to aging, achieving normal bone density at this time is important for future quality of life.9101112 Therefore, hormone therapy based on estrogen is the most important treatment for improving the quality of life, morbidity, and mortality in TS patients.
The positive effect of hormone therapy in postmenopausal or young women with oophorectomy have been proven by many studies, but there is no standard protocol for hormone therapy in TS patients.1314 Clinical practice guidelines for girls and women with TS recommend hormone replacement therapy (HRT) for the induction, maintenance of secondary sexual characteristics; however, best strategy for HRT to achieve better bone mineral density (BMD) in adulthood has not yet been established.1 Some studies emphasized early introduction of estrogen replacement therapy (ERT) in TS patients.151617 Typically, the peak bone density is achieved from the beginning of puberty to the age of 18 in healthy girls.18192021 The general therapeutic goals of TS patients are to increase final adult height, to develop secondary sexual characteristics of puberty, and to improve the quality of life, morbidity, and mortality of TS patients throughout the lifetime. TS patients often show bone fragility, which might be due to X chromosome abnormality, estrogen deficiency or combination of the two.20
There are several reports on the relationship between ERT and BMD in patients with TS.1617 Nguyen HH. et al revealed that BMD can be preserved with early initiation and continued use of ERT in TS, and Nakamura et al.17 also reported ERT, especially with early initiation, was effective for increasing BMD in women with TS. The response to hormone therapy may vary by race and geographical environment, and such a study to reveal the effects of HRT on BMD in TS patients has never been conducted in Korea. We analysed a large dataset of TS patients in tertiary hospital to investigate the effects of HRT on BMD in Korean adults with TS. Therefore, the purpose of this study was to 1) investigate BMD in women with TS in Korea, 2) evaluate clinical parameters, especially their relationship with ERT, and 3) investigate longitudinal changes in BMD.
METHODS
Study design and participants
This was a retrospective case–control study analysed medical records of patients with TS treated at Severance Hospital, Yonsei University College of Medicine (Seoul, South Korea) from 1997 to 2019. BMI, age, height, weight, chromosome karyotype, ERT starting age, duration of ERT, and BMD were obtained at each age point. TS was diagnosed by chromosome analysis from peripheral blood and karyotype containing other than 45XO is considered mosaicism. A total of 188 TS patients who had a bone density test at least once was included in the study. All patients received regular and appropriate doses of ERT during the visiting period. Bone density was measured at the lumbar spine L1-L4 and femur neck (FN) and calculated as an absolute value (mg/cm2) and Z-score. The Z-score was the mean BMD with reference to BMD (similarly adjusted for body surface and vertebral volume) of a population of age-matched healthy people.21
Control group
To recruit the healthy control group, we used the Korean National Health and Nutrition Examination Survey (KNHANES), which is a nationwide, population-based, cross-sectional health examination and survey conducted annually by the Korea Centers for Disease Control and Prevention on the basis of the National Health Promotion Act. They select a representative sample of the noninstitutionalized civilian Korean population using a stratified, multilevel, clustered probability sampling method. Approximately 10,000 individuals were selected each year without overlap with previous samples and socioeconomic conditions, health-related behaviors, quality of life, health care, anthropometric measures, and biochemical and clinical profiles for non-communicable diseases were collected. We used female subjects who participated in the KNHANES in 2010–2011 and excluded participants who had a thyroid disease, end-stage renal disease, or malignancy, or whose information on dual-energy X-ray absorptiometry (DXA) was incomplete. The average BMD value and Z-score of Korean women according to KNHANES were considered to represent the BMD value and Z-score of the healthy control group.
Statistical analyses
SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) and R version 4.2.0 for Windows (R studio, Boston, MA, USA) were used for all statistical analyses. Summary statistics were expressed as mean ± SD, and frequency counts were expressed as a percentage. An independent t-test and Mann–Whitney U test were used for group comparisons. To compare the variables, independent t-test for unrelated samples was used if the distribution of the variable was consistent with normal distribution and the variances were equal, or the Mann–Whitney test was used in the case of incompatibility with normal distribution. Repeated measures ANOVA was calculated to investigate changes in the analyzed parameters over time. To investigate the relationship between continuous variables, the Pearson r correlation coefficient was calculated if the distribution of both variables was consistent with normal distribution. Shapiro-Wilk test was used to confirm that the data satisfies the assumption of normality in age 40–44 years. ANOVA was used to analyze differences between the groups. Regression analysis was used to determine the relationship between treatment age and treatment period in the cross-sectional analysis. In all analyses, P < 0.050 was considered statistically significant.
Ethics statement
The KNHANES was conducted under ethical approval by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (2010-02CON-21-C, 2011-02CON-06C) and all participants provided written consent forms before enrollment. This study was approved by the Institutional Review Board (IRB) of Severance Hospital on 2020 (#4-2020-0429).
RESULTS
Patient characteristics
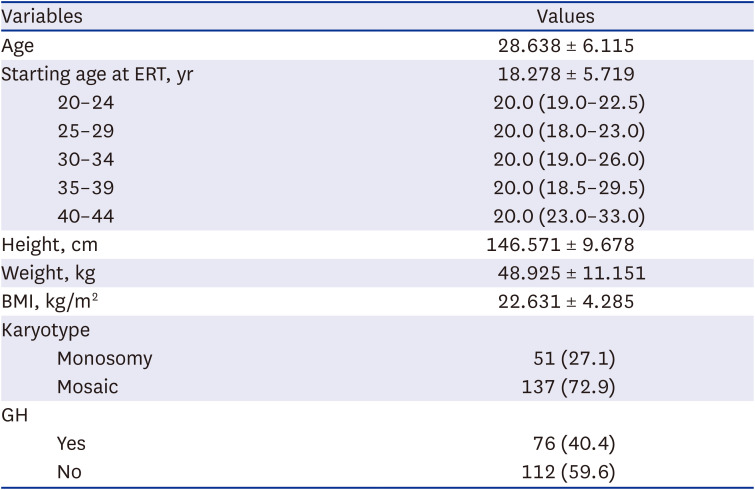
The baseline characteristics of 188 TS women were presented in Table 1. We stratified the age into intervals of 5 years and conducted the analysis. And there was no significant difference in the hormone start age between age groups (P = 0.069).
Table 1
Clinical features of the study group (N = 188)
Comparison of BMD in women with TS and healthy Korean women
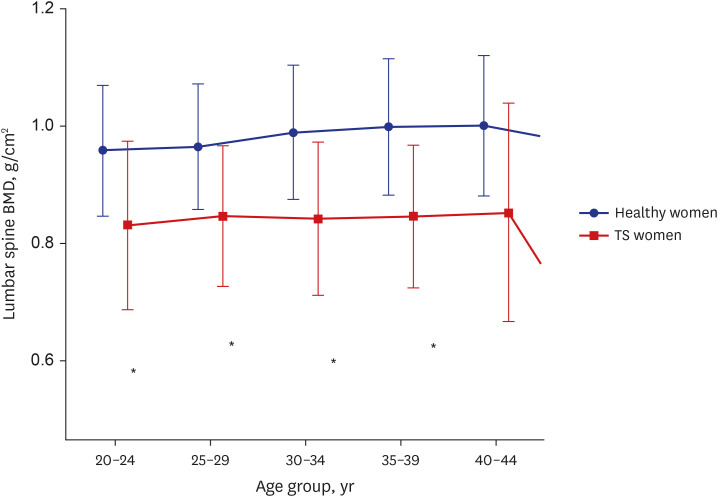
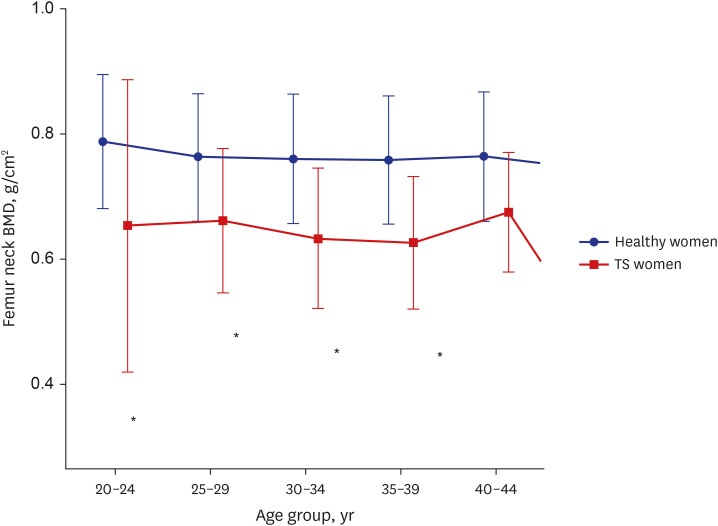
The BMD values and Z-score value of TS patient were compared with healthy Korean women by using KNHANES data. Fig. 1 revealed lumbar spine BMD was lower in TS patients compared to normal controls and it was statistically significant before in every age subgroup before 40 years old (Table 2, Fig. 2). Also, FN BMD was lower in TS patients and statistically significant in every age subgroup from 20 years to 45 years old (Table 2, Figs. 3 and 4).
Fig. 1
Lumbar spine L1–L4 BMD of Turner syndrome women compared to healthy Korean women according to age.
BMD = bone mineral density.
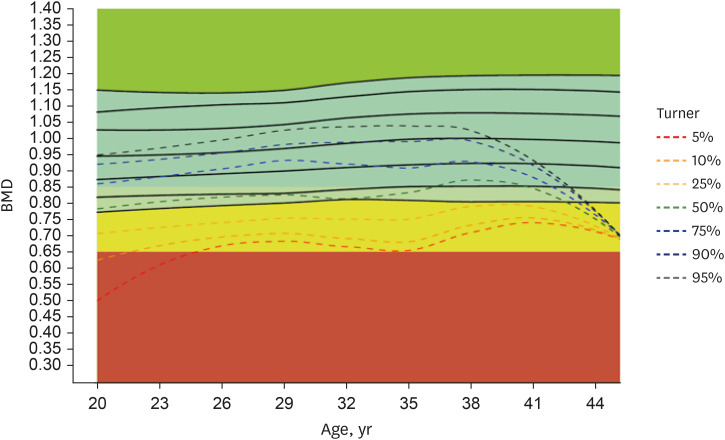
Table 2
Lumbar spine and femur neck BMD of TS women compared to healthy Korean women
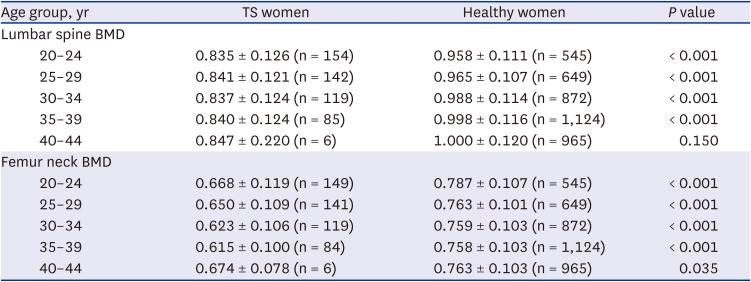
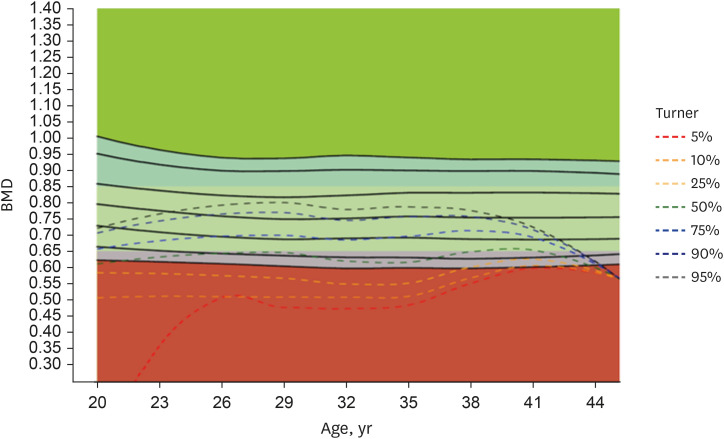
Fig. 2
Lumbar spine L1–L4 BMD of TS women compared to healthy Korean women.
BMD = bone mineral density, TS = Turner syndrome.
Effects of ERT start age on BMD in women with TS
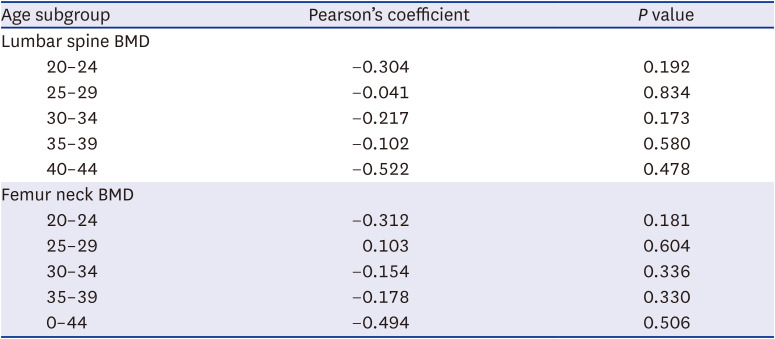
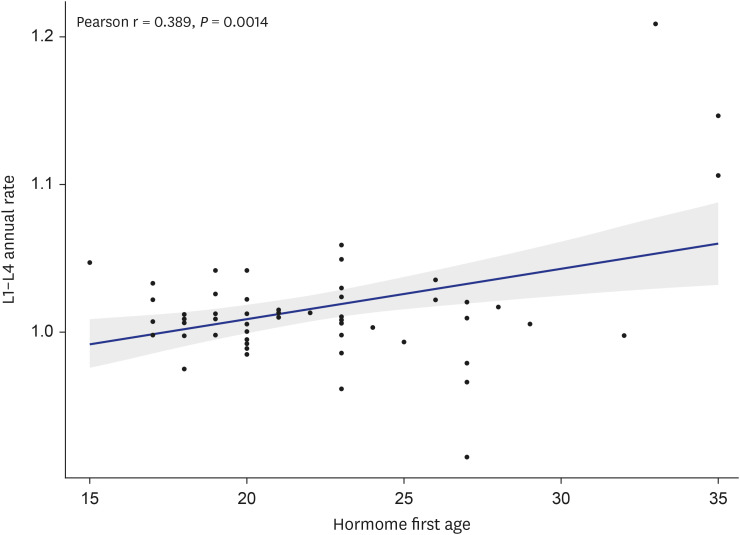
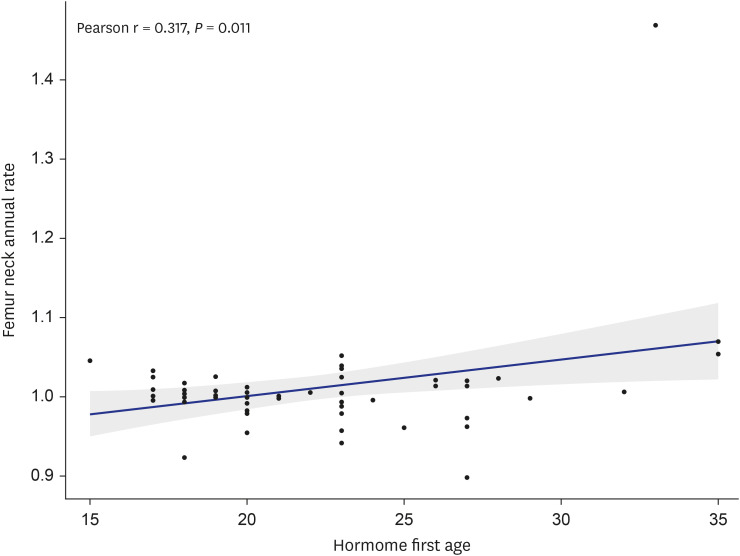
Effect of ERT start age on lumbar spine and FN BMD was analyzed by age subgroup. Pearson’s correlation coefficient was negative in almost every age subgroup, meaning the later ERT started, the lower the BMD, however there was no statistical significance (Table 3). Also, annual change rate of lumbar spine and FN BMD was positively correlated with ERT start age (P = 0.001 and 0.011, respectively, Figs. 5 and 6).
Table 3
Correlation between estrogen replacement therapy start age and BMD by age subgroup
Effects of duration of ERT on BMD in women with TS
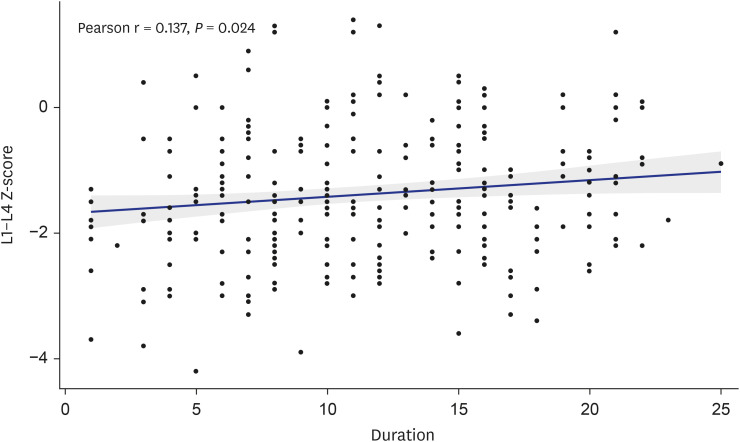
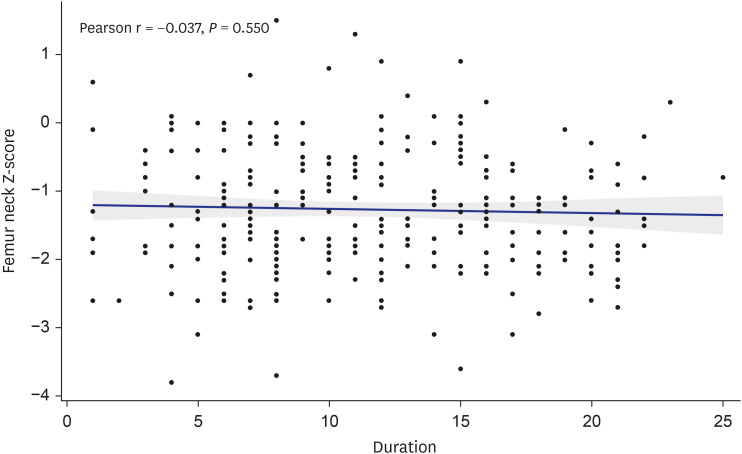
The effects of ERT duration on BMD were evaluated by using multiple regression analysis. ERT duration was significantly positively associated with lumbar spine BMD Z-score with Pearson correlation coefficient 0.137 (P = 0.024, Fig. 7). However, there was no correlation between ERT duration and FN BMD (P = 0.550, Fig. 8).
Comparison of TS patients according to the mosaicism
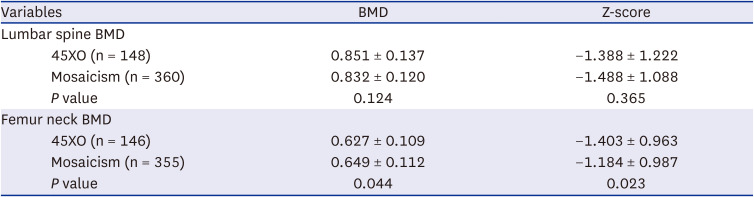
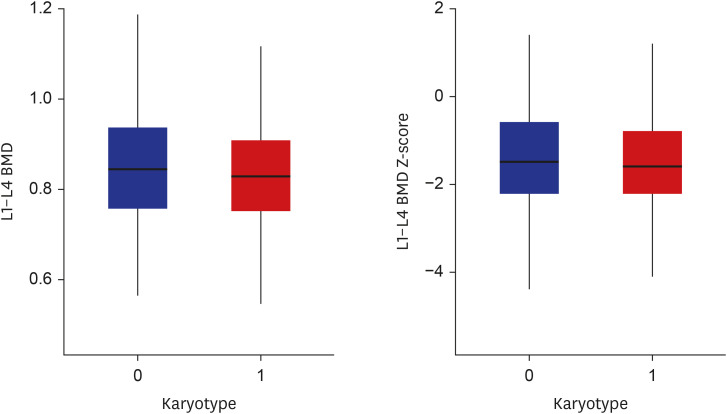
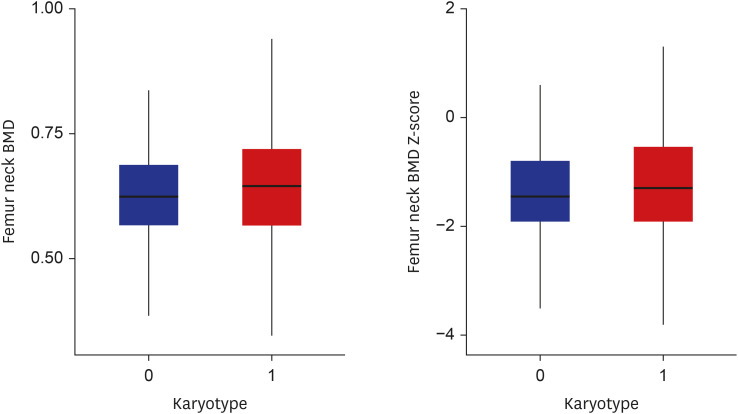
TS patients were categorized into 45XO group and mosaicism group according to karyotype. There was no difference in lumbar spine BMD value or Z-score between TS patients with and without mosaicism (P = 0.124 and 0.365, respectively; Table 4 and Fig. 9). However, FN BMD value and Z-score were significantly higher in women with mosaicism than 45XO group (P = 0.044 and 0.023, respectively; Table 4 and Fig. 10).
Table 4
Lumbar spine and femur neck BMD according to karyotype
Analysis of factors affecting low BMD in TS patients
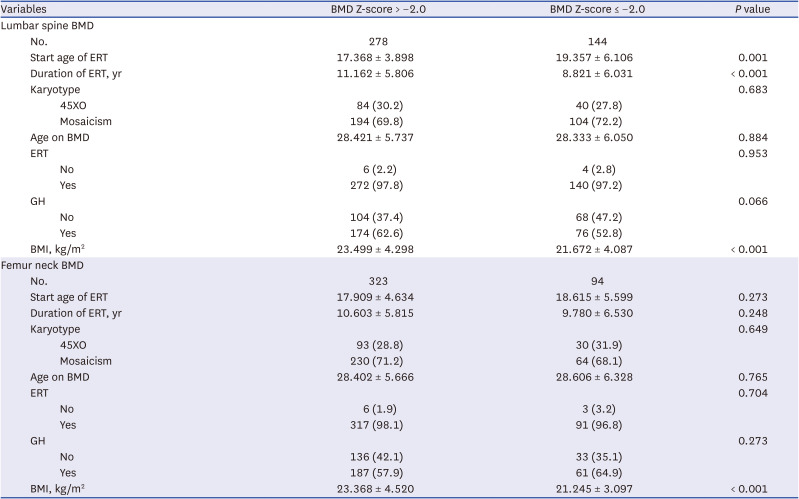
TS patients were divided into two groups according to whether their BMD Z-score was > –2.0 or ≤ –2.0. ERT start age, ERT duration, karyotype, ERT status and GH use in each group was analyzed. ERT start age, ERT duration, and BMI were significantly associated with lumbar spine BMD, whereas BMI was the only factor that significantly affected FN BMD (Table 5).
Table 5
Analysis of factors affecting low BMD based on Z-score −2.0
DISCUSSION
In this study, we investigate the effects of HRT on BMD in Korean TS patients and this is the largest study done in Korea. Similar to results obtained in other countries, women with TS had lower BMD than healthy Korean women.162223 Also, this study revealed ERT start age, duration of ERT, and karyotype affects the lumbar spine and FN BMD in Korean TS patients.
Estrogen plays a critical role in BMD of TS women. Only few girls with TS exhibit spontaneous puberty, and most of them need ERT to initiate or maintain pubertal development.24 Secondary sexual characteristics and maximum bone mass can be achieved by ERT.1 The BMD of cortical bone is lower than that of trabecular bone in girls with TS.25 There are some studies indicate ERT contributed to the increase and maintenance of lumbar BMD, and the early induction of ERT is beneficial for achieving higher BMD in adults with TS.151622232627282930 Nishigaki et al.29 reported that the starting age of HRT showed a negative and significant association with BMD, indicating the importance of early introduction of ERT to acquire better bone mineral density.
Our study revealed the group with lumbar spine BMD below -2.0 had significantly later ERT onset age and shorter ERT period than BMD over -2.0. This showed importance of early hormone induction and continuation of treatment. According to this result, it is recommended to start ERT before the age of 17 at the latest, and continue the treatment at least 10 years. The discrepancy in results for the effect of starting age of ERT on Tables 3 and 5 might because the trend may not be apparent when viewed as continuous, however dividing the patients based on a cutoff point reveals significant differences. Also, each person may have a different rate of response to bone mineral density depending on ERT.
There was no statistically significant difference in FN BMD, which means hormone therapy benefit lumbar spine, predominantly composed of trabecular bone, more than FN mostly made up of cortical bone. Trabecular bone and cortical bone could be affected by hormones differentially, and bone loss is known to more rapid in trabecular bone after menopause or estrogen deficiency status.3132 BMD of cortical bone is lower than that of trabecular bone in girls with TS and seems to be relatively unaffected by ERT.25 Khastgir et al.33 showed increased BMD due to augmented trabecular bone volume with unchanged cortical bone in TS patients after estradiol implants. Nevertheless, our study also obtained results that annual change rate of lumbar spine and FN BMD was positively correlated with ERT start age. This means TS patient could catch up BMD quickly even though they start hormone therapy late.
Another interesting point of this study is conflicting results for lumbar spine and FN BMD in TS with mosaicism. About 45% of Turner’s syndrome patient have non-mosaic monosomy 45XO, 20–35% have mosaic aberrations of chromosome X, and other 10–35% X chromosome rearrangements.3435 Generally, BMD is higher in mosaic TS, since spontaneous menarche is more common.2336 In our study, BMD was significantly increased in TS with mosaicism only in FN. According to this result, karyotype seems to affect cortical bone more than trabecular bone in TS patients and further study is needed.
This study has strength on large size and relatively homogeneous follow-up done in single institution. However, there are some limitations. First, since this is the retrospective study, the ERT protocol was not unified. Second, we did not analysed bone quality, such as trabecular bone score, which is also important for bone strength.2837 Also, several factors affecting BMD, such as physical fitness, vitamin D deficiency, and GH administration were not included in the study.2838 A potential effect of GH on bone density in TS patient has been reported, and combination therapy with both estrogen and GH may lead to higher spinal BMD than ET alone.3940 In this study, the effect of GH was not statistically significant, but larger cohort studies are needed to confirm the results.
All women with TS in this study had low BMD, which was associated with late ERT start, and short ERT duration. Despite some limitations, this study revealed that early induction and long-term use of estrogen in TS patients can increase BMD. Further study with a larger cohort will be needed.
 XML Download
XML Download