

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) remains a significant global health issue, which infected about 10.6 million people and caused 1.6 million deaths in 2021.1 To end this TB epidemic, the World Health Organization (WHO) suggested the END TB strategy to achieve the milestones and targets for 2030 and 2035.23 Integrated, patient-centered care is one of the pillars of End TB strategy and it focuses on individual patient preferences, needs, and values and addresses not only the medical care but also social and economic factors.45 The management of TB has traditionally prioritized biomedical and public health approaches that focus on rapid detection, case notification, and close monitoring for adherence, with less emphasis on the needs and preferences of individual patients. However, recent efforts have sought to shift towards a patient-centered approach, recognizing the importance of tailoring care to the unique needs and experiences of each patient. Patient-centered care has been primarily used to improve adherence, reduce lost to follow-up (LTFU), and improve treatment outcomes in various settings.67
South Korea has experienced continuing decline in TB incidence, at a rate of 39.8 per 100,000 in 2022.8 After Korea Disease Control and Prevention Agency (KDCA) launched public-private mix (PPM) collaboration which deployed TB management-dedicated nurses to private healthcare institutions, the quality of TB management improved and the success rate of treatment by enhancing patient adherence through education programs and counseling increased.9 Despite these efforts, the success rate of treatment has remained stagnant at 80–81%10; South Korea had the highest incidence of TB among member countries of Organization for Economic Cooperation and Development in 2021.1 Thus, we need to know the detailed risk factors for unfavorable outcomes including LTFU, not evaluated (NE), death, and treatment failure (TF) to enforce patient-centered care approaches for management of individuals with TB. This study aimed to analyze the risk factors for unfavorable treatment outcomes among patients with TB registered at tertiary referral centers. We attempted to identify the characteristics of patients in different subgroups of poor treatment outcomes to determine the factors that are important for improving each unfavorable TB outcome.
METHODS
Study population
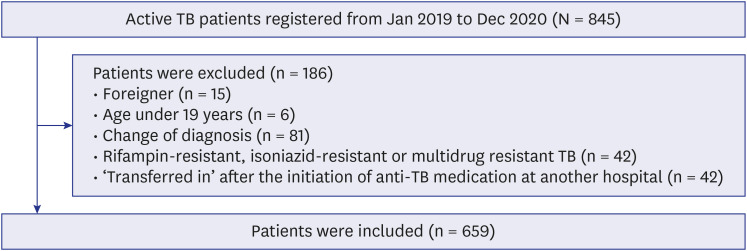
A retrospective cohort of 845 patients diagnosed with active TB between January 2019 and December 2020 at Severance Hospital, a tertiary referral hospital, was eligible for analysis. After excluding 186 individuals (foreigners [n = 15], age < 19 years [n = 6], change of diagnosis [n = 81], rifampin-resistant, isoniazid-resistant, or multidrug-resistant TB [n = 42], and transferred to our center after the initiation of anti-TB medication at another hospital [n = 42]), 659 patients were included in the final analysis (Fig. 1). Using the Andrew Fisher equation with a confidence level of 95% and a standard error of 5%, we calculated the necessary sample size based on the reported 30,304 TB cases as of 2019 in South Korea.8 With an estimated sample size of 380, we determined that it was suitable for the number of patients we gathered.
Data collection and definition
Data on clinical and demographic factors, including age, sex, body mass index (BMI), smoking history, health insurance beneficiary status, previous TB history, type of TB, acid-fast bacilli (AFB) smear, TB polymerase chain reaction (PCR), TB culture results, comorbidities, treatment duration, presence of symptoms at the time of diagnosis, adverse drug reactions (ADRs), and laboratory findings, were collected. Treatment outcomes were defined according to the criteria suggested by the 2021 WHO Treatment Outcome Definitions for TB.11 Treatment success was defined as cure and/or treatment completion. Death was defined as mortality during treatment. NE was defined as no assigned treatment outcomes. In our study, NE group refers to “transferred out to other health institutions.” LTFU was defined as a patient who did not start treatment or whose treatment was interrupted for two consecutive months. TF was defined as a patient whose treatment regimen needed to be terminated or permanently changed to a new regimen or treatment strategy due to no clinical response or anti-TB drug intolerance.
Covariates
The following variables were measured as covariates that might influence the final treatment outcome: sex, age, smoking, BMI, health insurance beneficiaries, distance from the living area to the treatment center, type of TB, previous TB history, sputum AFB smear, culture results, TB PCR, symptoms. Health insurance beneficiaries were classified into two groups, “national health insurance” and “medical aid.” Patients receiving medical aid had an income less than 40% of the standard median income. The distance from the treatment facility was determined based on patients’ residence in the administrative districts. Patients living in Seoul, Gyeonggi or Incheon area were categorized as “Same or Neighboring,” while those living in other areas were classified as “Far-away.” We also collected information on the comorbidities (cardiovascular disease, diabetes mellitus, cerebrovascular disease, chronic liver disease, chronic lung disease, chronic kidney disease [CKD], malignancy, psychologic disease, and transplantation) and ADRs related with TB treatment. For cardiovascular disease, we included patients with coronary artery disease, heart failure, valvular heart disease, or arrhythmia. Chronic liver disease included patients who had chronic hepatitis B or C, alcoholic liver disease, and nonalcoholic liver disease. Chronic lung disease was defined as chronic obstructive pulmonary disease, asthma, bronchiectasis, or interstitial lung disease. Patients with a lower estimated glomerular filtration rate (< 30) or those undergoing dialysis were classified as having CKD or end-stage renal disease (ESRD). Psychologic disease defined as depression, schizophrenia, drug dependency, or dementia. For treatment-related adverse events, we classified as follows: grade 1 was assigned for cases with drug-related side effects, grade 2 for cases where additional medication was required due to drug-related side effects while maintaining anti-TB medication, and grade 3 or severe ADR for cases where treatment was discontinued or hospitalization and other measures were necessary due to drug-related side effects.
Statistical analysis
Categorical variables are presented as numbers and percentages, whereas continuous variables are presented as medians (interquartile range [IQR]). The baseline characteristics of each treatment outcome were analyzed using analysis of variance test for continuous variables and a χ2 test for categorical variables. Cox proportional hazard regression analysis was conducted to evaluate the factors that accounted for unfavorable treatment outcomes (LTFU, NE, death, TF). All covariates with a P value < 0.05 in the unadjusted model were included in the multivariate model. Furthermore, we conducted statistical analysis with age, sex, and BMI as common adjusted variables. We included only the culture results as variables; considering multicollinearity, we excluded the AFB smears and PCR results. Statistical significance was defined as P < 0.05. SPSS Statistics (version 26.0; SPSS Inc., Chicago, IL, USA) and R software, version: x64 4.2.1 (R Foundation, Vienna, Austria) were used for all statistical analysis.
RESULTS
Baseline characteristics of TB patients
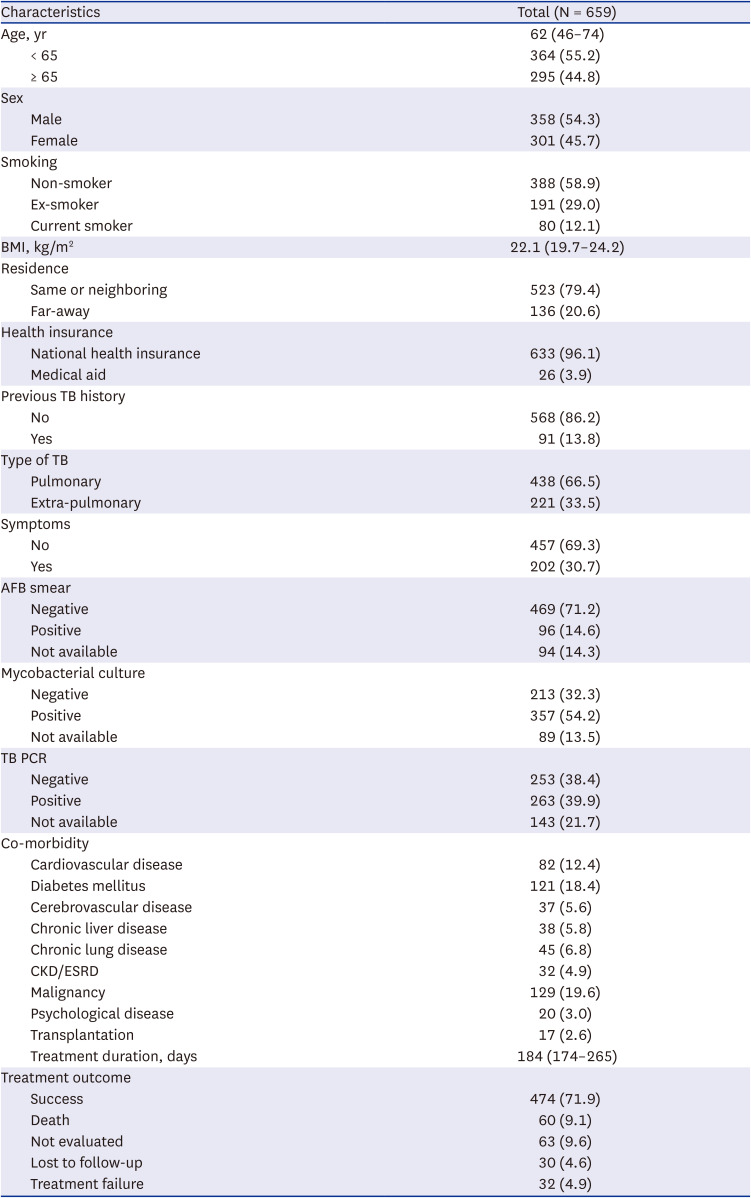
Table 1 shows the baseline characteristics of 659 patients with TB. The median age was 62 (IQR 46–74) years, and 54.3% of the participants were male. Five hundred sixty-eight patients (86.2%) had no history of TB, and pulmonary TB was the major cause in 438 patients (66.5%). Smear positivity of AFB was 14.6%, and mycobacterial culture was positive in 357 patients (54.2%). The most common co-morbidity was malignancy (19.6%). Treatment duration was median 184 (IQR 174–265) days and treatment success rate was 71.9%.
Table 1
Baseline characteristics of the study population
Different characteristics for each treatment outcome
Table 2 shows the differences in the baseline characteristics of patients according to treatment outcomes. Treatment success was achieved in 474 patients (71.9%). The number and proportion of “death,” “NE,” “LTFU,” and “TF” were 60 (9.1%), 63 (9.6%), 30 (4.6%), 32 (4.9%) respectively. Patients in the “death” group were older (median 78 years, P < 0.001) and had relatively lower BMI (median 20.6, P = 0.019) compared with other groups. The NE group had a higher proportion of patients (49.2%) living far from the treatment center. There were no significant differences in TB-related factors, including previous TB history, AFB smear results among the groups. The positive result of mycobacterial culture was relatively low in the LTFU group (26.7%, P < 0.001). The prevalence of co-morbidities varied across the groups. Cardio/cerebrovascular disease, CKD/ESRD, and malignancy were more common in the death group. The proportion of patients who experienced TB-related ADRs was higher in the LTFU (74.1%), and TF (87.5%) groups.
Table 2
Differences in characteristics according to treatment outcomes in patients with TB
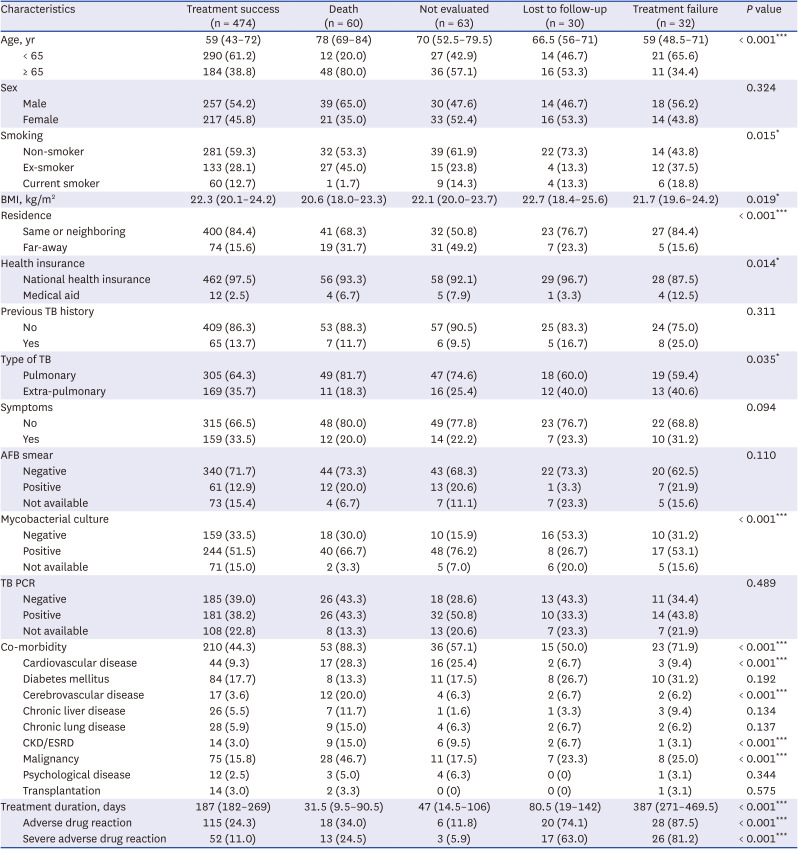
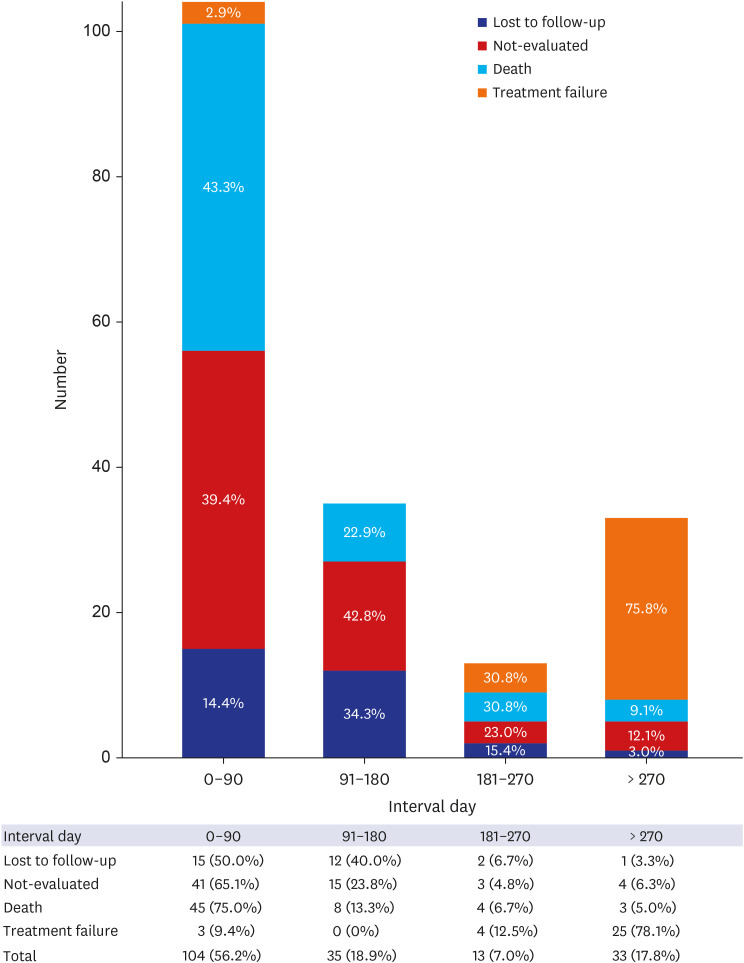
Fig. 2 shows the time interval for unfavorable outcomes after treatment initiation. More than half (56.2%) of the unfavorable outcomes occurred within the first 3 months of treatment (50% LTFU, 65.1% NE, 75% death, and 9.4% TF).
Treatment-related adverse events
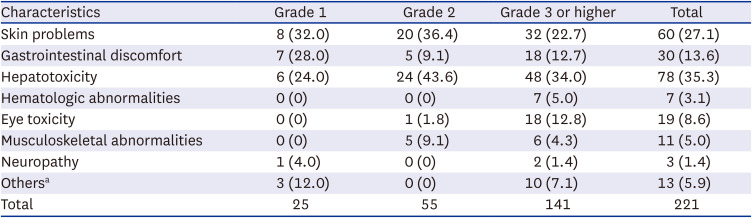
Table 3 shows the classification of ADRs according to the organ system affected and severity. In total, 221 ADRs were reported in 187 patients (28.4%). More than half (63.8%) of the patients were classified as having grade 3 ADR or higher. The most common ADR was hepatotoxicity (35.3%), followed by skin problems (27.1%) and gastrointestinal discomfort (13.6%).
Table 3
Adverse drug reactions during tuberculosis treatment
Different risk factors for unfavorable treatment outcomes
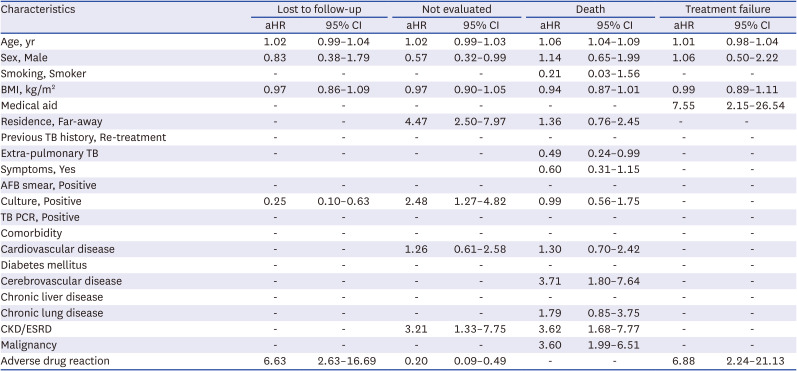
Table 4 shows the multivariate results for the risk factors related to unfavorable outcomes. A culture-confirmed diagnosis of TB was related to a lower risk of LTFU (adjusted hazard ratio [aHR], 0.25; 95% confidence interval [CI], 0.10–0.63), whereas the occurrence of ADRs related to TB treatment significantly increased the risk of LTFU (aHR, 6.63; 95% CI, 2.63–16.69). Patients living far from the hospital (aHR, 4.47; 95% CI, 2.50–7.97), and patients with CKD/ESRD (aHR, 3.21; 95% CI, 1.33–7.75) were at a higher risk of being transferred out to other health institutions and we could not follow-up on the final treatment outcomes. However, patients who experienced ADRs during TB treatment were less likely to transfer out to other hospitals (aHR, 0.20; 95% CI, 0.09–0.49). As expected, higher mortality was associated with older age (aHR, 1.06; 95% CI, 1.04–1.09). Extra-pulmonary TB had a lower mortality rate than pulmonary TB (aHR, 0.49; 95% CI, 0.24–0.99). Patients with comorbidities, especially cerebrovascular disease (aHR, 3.71; 95% CI, 1.80–7.64), CKD/ESRD (aHR, 3.62; 95% CI, 1.68–7.77), and malignancy (aHR, 3.60; 95% CI, 1.99–6.51) were more associated with death. For TF, lower household income (medical aid group, aHR, 7.55; 95% CI, 2.15–26.54), and ADR (aHR, 6.88; 95% CI, 2.24–21.13) were significant risk factors. Univariate and multivariate analysis for each unfavorable outcome are presented in Supplementary Tables 1, 2, 3, 4.
Table 4
Risk factors associated with each unfavorable outcome
DISCUSSION
In this study, we identified different risk factors for each unfavorable outcome, namely, LTFU, NE, death, and TF among patients with TB. Our results show that ADRs and microbiological uncertainty are the risk factors for LTFU. The distance between treatment center and resident area, as well as co-morbid CKD/ESRD, were associated to “transfer out” to other health institutions. Old age and multiple co-morbidities are the risk factors for mortality during TB treatment.
Improving adherence to treatment and enhancing successful treatment outcomes are key pillars of national and global TB policies.5 Therefore, a patient-centered approach based on the needs and values of patients has been emphasized to promote treatment adherence. In South Korea, more than 90% of patients with TB has been cared for in private health institution since 2012.12 Thus, KDCA launched PPM collaboration which deployed TB management-dedicated nurses to private healthcare institutions to improve the quality of TB care. The implementation of the PPM project has contributed to a decrease in LTFU in TB management.1314 Continuous education and counseling of patients regarding their needs and barriers during TB treatment could lead to an improvement in adherence. However, LTFU is still around 5%15 and identifying the risk factors for LTFU and strengthening the TB management system are important tasks in South Korea. In the present study, the most important risk factor for LTFU was the occurrence of ADRs associated with TB treatment. ADRs increase the likelihood of treatment interruption.16171819 In our study, 187 patients (28.4%) experienced ADRs in total. Among the LTFU group, 20 (74.1%) patients experiencing ADRs. When ADRs occur, the treatment duration is prolonged, and in some cases, fatal outcomes can happen,20 and hence, the management of ADRs is crucial for improving treatment adherence and achieving successful treatment.
Individuals with a bacteriological confirmation had a lower likelihood of LTFU. In other words, microbiologic uncertainty increased the risk of LTFU, which is consistent with previous results in South Korea.21 The lower burden of mycobacteria in culture-negative TB and doubts regarding the diagnosis of TB may contribute to treatment interruption in this group.
Another unfavorable outcome of TB treatment is “NE,” which represents “transferred out to other institutions” in our study. The important issue regarding the “transferred out” outcomes is the possible treatment interruption or LTFU during the transition from one health center to another. In a previous study,22 it was found that 50% of “transferred out” patients did not re-register for TB treatment in other health centers and 24% of “transferred out” patients re-registered after more than 60 days. Thus, being “transferred out” increases the risk of treatment interruption and LTFU. In our study, living far from the treating center which is a well-known barrier to providing and taking sustainable health services, was an important risk factor for being “transferred out.” In general, people preferred to receive health services near their homes with familial support. Particularly, patients with ESRD who required regular hemodialysis near their homes showed higher odds of being transferred. South Korea has the advantage of good accessibility to health services, primarily private health services.23 Thus, efforts to build a continuous network across health institutions, to transfer in/out via PPM project with support from the public health centers, are essential to keep continuity of TB treatment and help facilitate prevention of LTFU in this “transferred out” group.
As expected, older age and multiple comorbidities were important risk factors for mortality during TB treatment. The lower treatment success rate due to the high rate of death in elderly TB patients is an important public health concern in low-incidence countries.24 In our study, 44.8% of the total patients were older than 65 years, and among deceased patients, 80% were older than 65 years. Several factors are associated with mortality in elderly patients with TB. The high mortality rate in elderly TB patients may be due to reduced immune function25 and age-related comorbidities, as observed in our study.26 In addition, elderly people with TB often experience challenges in timely diagnosis due to atypical symptoms and difficulties in accessing healthcare services.27 Considering the high burden of elderly TB patients in South Korea, health interventions to care for elderly people should be prioritized. Actively searching for active TB in elderly patients, who are more likely to exhibit unusual manifestations, can facilitate early diagnosis and timely treatment, potentially reducing mortality.28 Strengthening the health system to enhance medical accessibility for the elderly, and providing community/home-based healthcare services with the help of TB-dedicated nurses for patient management could improve treatment outcomes of vulnerable elderly people with multiple co-morbidities.2930
Among the 32 patients classified as TF, 6 patients (18.8%) were categorized as such due to the absence of clinical improvement, while the remaining 26 patients (81.2%) were classified as TF due to regimen change because of ADRs, based on 2021 WHO Treatment Outcome Definitions.11 Although the treatment regimen for these 26 patients was changed, they successfully completed the longer treatment course.
This study was conducted at a referral center that registers approximately 300–400 TB patients yearly. We reviewed individual medical histories and treatment outcomes, including the occurrence of ADRs. However, several limitations of this study should be considered when interpreting the results. First, this was a single-center study; therefore, we could not reflect the heterogeneous spectrum of patients with TB. Second, we excluded foreign-born and drug-resistant patients with TB. Considering the increasing number of foreign-born patients and poor treatment outcomes of drug-resistant TB, these issues should be investigated in future studies. Third, given that this was a retrospective analysis, it is possible that ADRs across the course of treatment, particularly those of grade 1 and grade 2, were underestimated. Fourth, we could not follow the final treatment outcomes of patients who were transferred. Due to protection of personal information, we were unable to access the final treatment outcomes of patients who were transferred. An integrated system for monitoring treatment outcomes is necessary for the comprehensive analysis and management of national TB outcomes.
In conclusion, the treatment outcomes of patients with TB registered at a tertiary referral center were suboptimal, and each unfavorable treatment outcome had different risk factors. To reduce unfavorable outcomes, such as mortality, LTFU, NE, and, TF, a variety of healthcare services—functional across multiple health institutions, private-public sectors, and hospital-community networks—are needed to provide support to high-risk patients based on their needs and values. In the future, studies should include multiple centers to understand the characteristics of a wider population.
 XML Download
XML Download