

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has caused tremendous turmoil, with over 2 million deaths and hundreds of millions of individuals isolated worldwide.1 However, its impact on children and adolescents has been relatively minimal in terms of morbidity and mortality rates.2 Similar to the events observed during the outbreak of severe acute respiratory syndrome in 2003, quarantine measures during the COVID-19 pandemic have had adverse mental repercussions, such as increased incidence of depression and posttraumatic stress disorder.3 A survey of over 50,000 individuals in the United Kingdom revealed that the percentage of individuals suffering from mental stress rose from 19% in 2018 to 27% in April 2020, 1 month after the COVID-19 lockdown was enforced.4 The quarantine measures imposed during the COVID-19 pandemic posed a significant challenge to the mental health of children and adolescents as well.2
Adolescence is a vulnerable period in which individuals undergo significant transitions.56 Mental health issues are more common than physical issues during this period and can impact individuals’ mental health status into adulthood.7 During adolescence, individuals establish the direction of their behaviors and develop self-concept and self-worth based on their experiences of peer acceptance and rejection, highlighting the importance of peer interactions for mental health.8 The impact of the COVID-19 pandemic and subsequent lockdown measures on the mental health of young people has raised concerns. Children and adolescents were unable to attend school during quarantine, which potentially led to a decrease in social contact, loneliness, and increased reliance on the internet and social media. Some of them also experienced unstable home environments and exposure to domestic violence.259
The COVID-19 pandemic significantly affected the global economy as well, including an increase in the worldwide unemployment rate.10 Approximately 30 million people in the United States and 400 million people worldwide have lost their jobs in the ongoing economic recession.11 The children and adolescents who observed their parents experiencing anxiety regarding potential unemployment and helplessness related to physical distancing may have developed stress regarding their future prospects.3 The deteriorating economic conditions may also have triggered conflict within families, taking a toll on the mental health of children and adolescents through various pathways, including child abuse.7
Several studies have examined the mental health of children and adolescents during the COVID-19 pandemic, their findings are conflicting. Some studies indicated that families spending more time together during the COVID-19 crisis may have strengthened the sense of community and social support in some households, positively influencing the mental health of children.12 However, others revealed an increased adverse childhood experiences13 and risk of mental disorders, such as depression, anxiety, posttraumatic stress disorder, and addiction, among children and adolescents.5 It is clear that negative childhood events linked to poor mental health outcomes and an increased risk of suicide attempt.13 As the COVID-19 pandemic prolongs, there are also numerous studies indicating that suicide rates tend to increase in general population.14 Although the impact of the COVID-19 pandemic on the risk of suicide among vulnerable populations is of utmost importance, research on suicide risk in children and adolescents is lacking1415 and needs to include periods before, during, and after COVID-19. Additionally, studies that have addressed the suicide attempt risks among adolescents depending on financial stress or loneliness that are closely associated with COVID-19 pandemic are relatively rare. Therefore, this study examined the trends in the suicidal risk population before and after the COVID-19 pandemic and investigated the impact of COVID-19-related social isolation and financial stress on suicide attempts among adolescents.
METHODS
Data source and participants
We used raw data from the Korean Youth Risk Behavior Web-Based Survey (KYRBS),16 which is planned by the Korea Centers for Disease Control and Prevention (KCDC) of the Ministry of Health and Welfare and conducted by the Ministry of Education. The KYRBS aims to assess the health behaviors of Korean youth and generate health indicators for youth health promotion projects that enable international comparisons. Sixteen items, including smoking, alcohol consumption, diet, mental health, personal hygiene, and sexual behavior, are assessed in the KYRBS. Since 2005, the survey has been conducted every year among students from grades 7–12 in 800 sampled schools nationwide using a standardized, anonymous, self-administered online questionnaire in computer labs.16
In this study, KYRBS datasets16 from years 2020 (N = 54,948, response rate = 94.9%), 2021 (N = 54,848, response rate = 92.9%) and 2022 (N = 51,850, response rate = 92.2%) were analyzed.
Measures
The outcome variable used in this study was suicide attempt, which was measured by the question, “Have you attempted suicide in the past 12 months?” Respondents who answered “yes” to this question were categorized as having made a suicide attempt. The main explanatory variable was the experience of worsening household finances due to the COVID-19 pandemic and loneliness. The experience of financial stress was defined as responding with “strongly agree” to the question, “Do you think that the financial condition of your family has worsened due to the COVID-19 pandemic?”, among the response options: “strongly agree,” “somewhat agree,” “somewhat disagree,” and “strongly disagree.” Additionally, to assess loneliness, responding “sometimes,” “often,” or “always” among the responses (“never,” “almost never,” “sometimes,” “often,” and “always”) to the question, “How often have you felt lonely in the past 12 months” was defined as feeling loneliness. Demographic factors, such as age, sex, and city type were also considered. Age was treated as a continuous variable. The reference categories for sex and city type were defined as “male” and “countryside,” respectively. Furthermore, potential risk factors of suicide attempt identified in previous studies17 were included as control variables. Some binary variables, including experience of suicidal ideation, having a suicide plan, experience of smoking, alcohol, and drug intake, feeling sadness or hopelessness, physical activity, and experiences of asthma, allergic rhinitis, and atopic dermatitis, were considered. All of these factors are categorized by “yes” and “no.” As for other factors, grade level was ranged from 12th grade (G6) to 7th grade (G1). Academic achievement and family socioeconomic status were divided into 5 categories: “high,” “middle high,” “middle,” “low middle,” and “low.” Based on the body mass index (BMI), the participants were classified as underweight (< 18.5), normal (18.5–22.9), overweight (23–24.9), and obese (≥ 25). Moreover, all the following parameters were recorded with 5 response options: stress (very low, low, middle, high, and very high), sleep (very high, high, middle, low, and very low), self-rated health (very good, good, normal, poor, and very poor), and the perceived body image (normal, very thin, thin, fat, and very fat). Questionnaires with missing responses to any 1 of the items were excluded from the analyses.
Statistical analyses
We conducted a frequency analysis to assess data on demographic factors including age, sex, and city type; outcome variables, suicide attempt; and other variables, such as financial stress and feeling of loneliness. Univariate logistic regression was performed to assess the association of the variables with suicide attempts. Subsequently, a multivariate logistic regression analysis was conducted to examine the influence of financial stress and feeling of loneliness on suicide attempts, while considering the effects of other variables. Confidence intervals (CIs) were set at 95%, and statistical significance was set at P < 0.05 in both the univariate and multivariate logistic regression analyses. All statistical analyses were performed using the Statistical Package for the Social Sciences for Windows, version 21.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The raw data was approved by the KCDC Institutional Review Board (certification number: 117058) and obtained in accordance with the KCDC regulations for the management and disclosure of raw data. Due to the study design, the KCDC Institutional Review Board waived the requirement to obtain informed consent.
RESULTS
Table 1 shows the general distribution of the study variables. As shown in Table 1, the sex ratio of the participants was similar, with 51.7% male participants in 2020, 52.0% in 2021 and 51.0% in 2022. A total of 3,072 (5.7%) adolescents in 2020 and 3,026 (5.7%) in 2021 reported a family financial stress due to the COVID-19 pandemic, while in 2022 the survey did not include questionnaires pertaining to family financial stress due to the COVID-19 pandemic, we were unable to examine this aspect. The 25,949 (48.5%) adolescents in 2020, 27,709 (51.8%) in 2021 and 27,440 (54.4%) in 2022 experienced loneliness in the prior 12 months.
Table 1
Baseline characteristics of demographic and psychological variables in the 2020–2022 Korean Youth Risk Behavior Web-Based Survey data
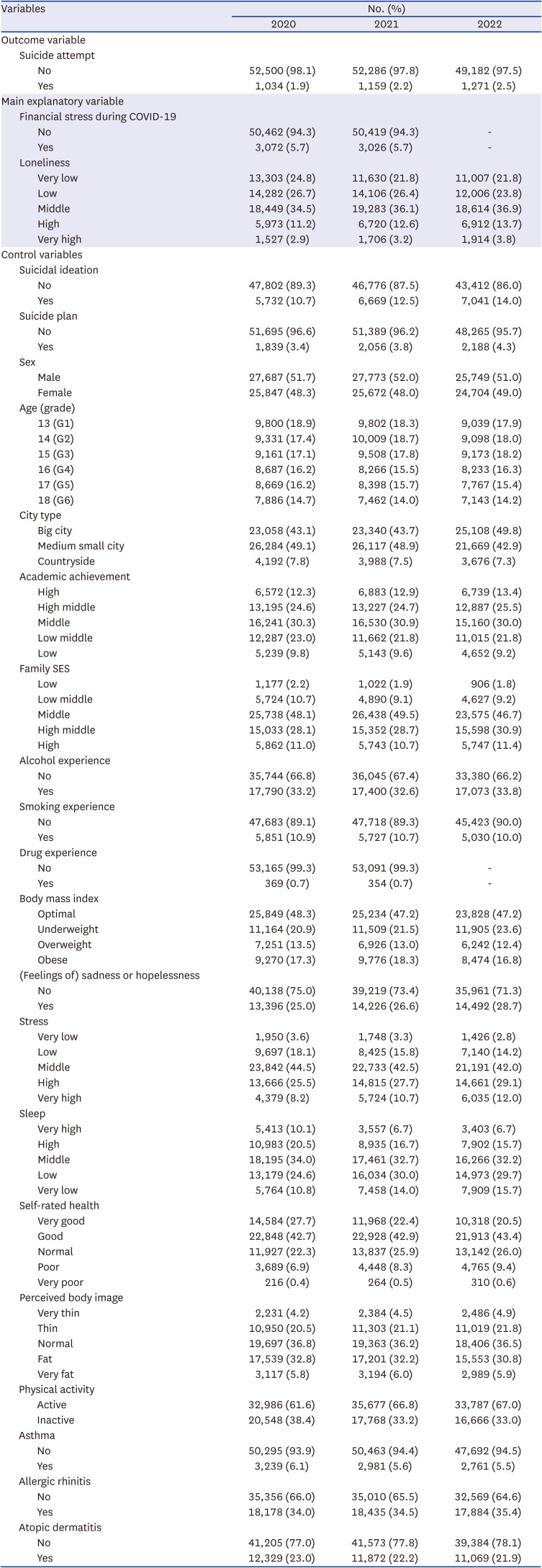
Approximately one-third of the adolescents (33.2% in 2020, 32.6% in 2021 and 33.8% in 2022) reported drinking alcohol, and approximately 10% reported trying cigarettes or e-cigarettes (10.9% in 2020, 10.7% in 2021 and 10.0% in 2021). Similarly, in both 2020 and 2021, 0.7% adolescents reported using drugs habitually other than for therapeutic purposes. However, due to limited access to the data for habitual use of drugs in 2022, we were unable to perform an analysis. Less than half of the adolescents (48.2% in 2020, 47.2% in 2021 and 47.2% in 2022) maintained a healthy BMI, while approximately 36% of them felt that they had an average body shape (36.8% in 2020, 36.2% in 2021 and 36.5% in 2021, respectively).
One-fourth of adolescents reported feeling sad or hopeless to the extent that their daily lives were disrupted for 2 consecutive weeks within the past 12 months (25% and 26.6% in 2020 and 2021, respectively), which increased to 28.7% in 2022. The rates of experiencing significant stress in their daily lives also showed a steady increase, reaching 33.7% in 2020, 38.4% in 2021, and 41.0% in 2022. However, the rates of feeling sufficiently rested during sleep demonstrated a consistent decrease, dropping to 30.6% in 2020, 27.4% in 2021, and 22.4% in 2022. Lastly, the rates of participants reporting feeling unhealthy were 7.3%, 8.8%, and 10.0% in 2020, 2021, and 2022, respectively, while in those same years, 38.4%, 33.2%, and 33.0% of the participants did not engage in physical activity that increases the heart rate above normal levels or causes shortness of breath for at least 60 minutes a day on at least 1 day within the past 7 days.
Suicide attempt
As shown in Table 1, when comparing the years 2020, 2021, and 2022, the rates of suicidal ideation were 10.7%, 12.5% and 14.0% respectively, which means there was an increase of 1.8% in 2021 and an additional 1.5% increase in 2022.
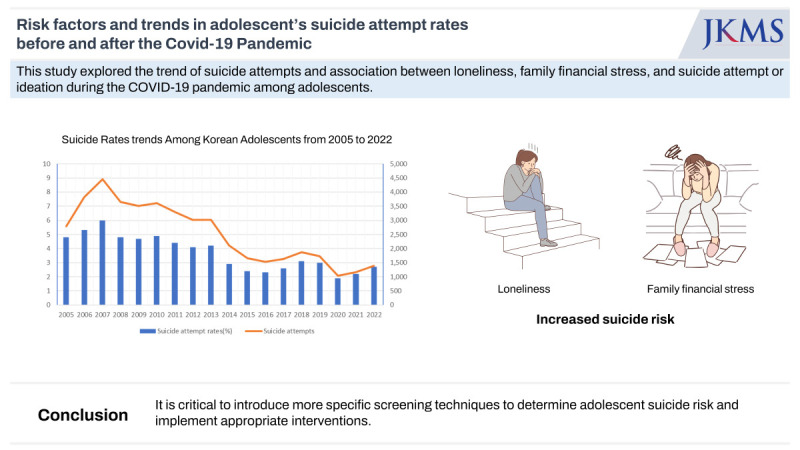
The annual suicide attempt rates and the number of suicide attempts among adolescents were depicted in Fig. 1. The rates showed an increasing trend from 2005 to 2007, reaching a peak of 5.8% in 2007. In 2005, the rate was 4.6% (2,622 out of 56,511), while in 2006 it was 5.2% (3,602 out of 69,497), and in 2007 it was 5.8% (4,148 out of 72,133). Subsequently, there was a slight decline in the rates from 2008 to 2011, ranging from 4.2% to 4.7%. In 2008, the rate was 4.7% (3,388 out of 72,703), in 2009 it was 4.5% (3,243 out of 72,399), in 2010 it was 4.7% (3,331 out of 70,809), and in 2011 it was 4.2% (3,055 out of 73,474). Following this, there was a further decrease in the rates from 2012 to 2016, reaching a low of 2.1% in 2016. In 2012, the rate was 3.9% (2,785 out of 72,229), in 2013 it was 3.9% (2,769 out of 70,354), in 2014 it was 2.7% (1,892 out of 69,959), in 2015 it was 2.2% (1,467 out of 66,068), and in 2016 it was 2.1% (1,369 out of 63,741). However, there was a slight increase in rates from 2016 to 2019, ranging from 2.1% to 2.9%, followed by a decline in 2019 and 2020. In 2017, the rate was 2.4% (1,445 out of 60,392), in 2018 it was 2.9% (1,697 out of 58,336), in 2019 it was 2.8% (1,545 out of 55,748), and in 2020 it was 1.9% (1,034 out of 53,534). In recent years, there has been a slight increase in rates, with 2.2% (1,159 out of 53,445) in 2021 and 2.5% (1,271 out of 50,455) in 2022. This indicates that the rates of suicide attempt increased by approximately 15.8% from 2020 to 2021 and by approximately 31.6% from 2020 to 2022.
Fig. 1
Suicide attempt rates trends among Korean adolescents from 2005 to 2022. This figure shows the annual suicide attempt rates among adolescents as well as the number of suicide attempts year-wise. The graph provides an overview of the trends and patterns in suicide attempt rates within adolescents over a specific period. The x-axis represents the years, while the y-axis represents the suicide attempt rates (left) and number of suicide attempts (right). The graph aims to highlight notable changes, fluctuations, or patterns in suicide attempt rates among adolescents over time.
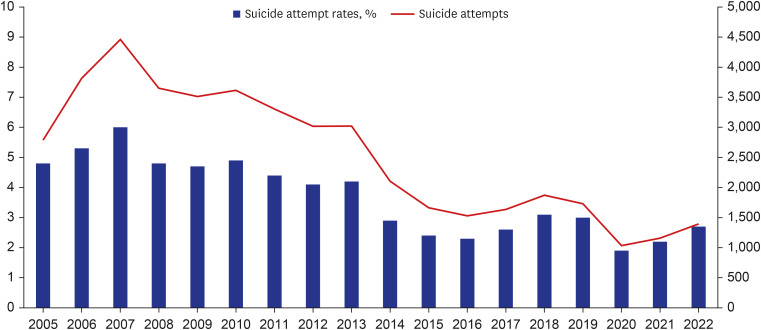
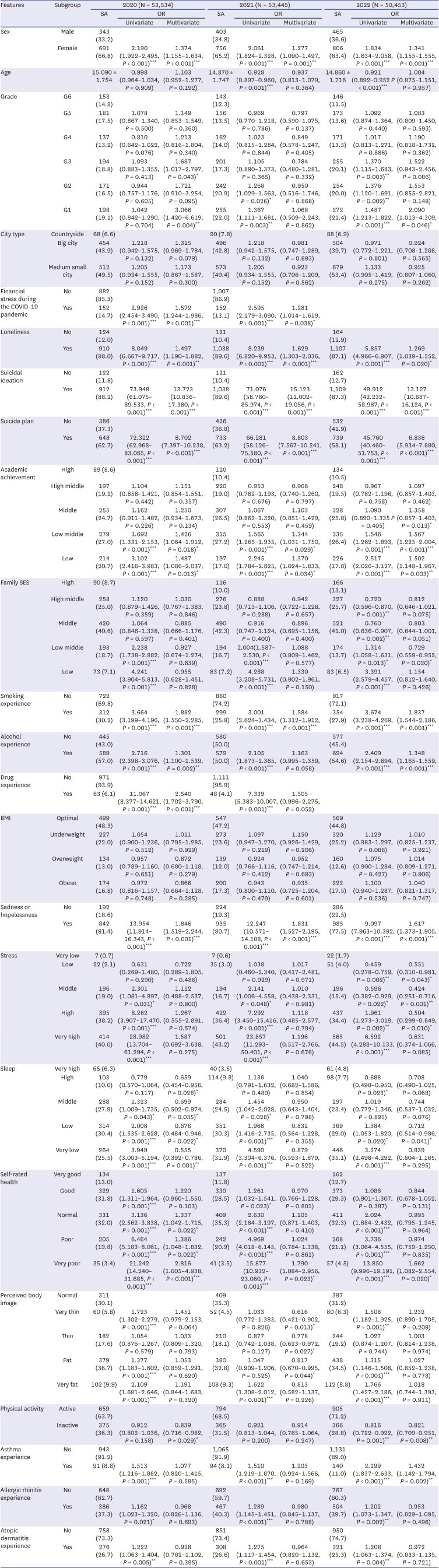
Table 2 shows the multivariate associations between the variables and suicide attempts. Data from 2020 and 2022 were analyzed separately. In the multivariate logistic regression model that controlled for other factors, the risk of suicide attempt was 1.6 times higher in 2020 and 1.3 times higher in 2021 among adolescents who reported a family financial stress due to the COVID-19 pandemic than among those who did not (in 2020: 95% CI, 1.256–1.882, P < 0.001; in 2021: 95% CI, 1.033–1.543, P = 0.023). The risk of suicide attempt was 1.5 times higher in 2020, 1.6 times higher in 2021 and 1.3 times higher in 2022 among adolescents who had felt lonely in the past 12 months than among those who did not (in 2020: 95% CI, 1.786–2.705, P < 0.001; in 2021: 95% CI, 2.159–3.260, P < 0.001; in 2022: 95% CI, 1.039–1.552, P = 0.020).
Table 2
Logistic regression analysis results for assessing the risk of suicide attempt
DISCUSSION
This study investigated the predictors of suicide risk among adolescents with a focus on financial stress and social isolation due to the quarantine measures during the COVID-19 pandemic. Overall, the results indicated that the rates of suicidal behavior including suicidal ideation, suicide plan and suicide attempt were gradually increased through 2020 to 2022. Furthermore, adolescents who experienced family financial stress and feelings of loneliness were at a higher risk of suicide attempt both in 2020 (shortly after the pandemic began) and in 2021 (1 year into the pandemic). Although the risk of suicide attempt among adolescents experiencing financial difficulties showed a slightly decreasing trend from 2020 to 2021, an increasing trend was identified in adolescents who experienced loneliness.
Social isolation, anxiety about infection, and economic hardship due to COVID-19 exacerbated stress-related disorders and suicidality in vulnerable populations.18 However, some studies have shown contradictory results in the early stages of the pandemic. One study found that suicide behavior decreased by approximately 50% during the COVID-19 lockdown, presumably due to reduced help-seeking and hospitalization rates during the lockdown.19 Another study reported a decrease in suicide rates during the first wave of the COVID-19 pandemic (February to June 2020) but a rapid increase in suicide rates, especially among women, children, and adolescents, during the second wave (July to October 2020) and once schools began reopening.2021 Previous study in US has reported an increase in suicide-related visits, particularly regarding suicidal ideation, among youth, aged 15–20, when compared to pre-pandemic periods.22 In this study, the rate of suicide attempt was at its lowest during the 2020 survey when school closure was still in effect. However, since 2020, suicide attempts have been consistently increasing every year. This trend is thought to be strongly linked to the increase in suicide deaths among youth that has been observed in South Korea23 and other countries.1424 Our findings can be explained by the hypothesis that the accumulation of stress resulting from the prolonged pandemic and continued limited access to mental health services and support may increase suicide attempts during the late pandemic. Numerous studies highlight the profound psychological effects of the pandemic, noting increased distress, depression, and anxiety in children and adolescents.2526 Long-term pandemic effects, such as social isolation, economic strain, and general uncertainty, might accumulate, particularly affecting vulnerable groups, leading to more suicide attempts.1827 Furthermore, the limited availability of mental health services and face-to-face care could also prevent timely and sufficient mental health support.2829
Even before the COVID-19 pandemic, financial burden—along with parents’ mental health, parenting quality, and family conflict—has been reported as a family-related factor influencing the mental health of adolescents.3031 A recent study showed that financial problems were associated with depressive symptoms in adolescents from families with a reduced income due to the COVID-19 pandemic as well as those experiencing subjective financial pressure.32 These findings are in line with our observation that adolescents who experienced a family financial stress during the COVID-19 pandemic were at an increased risk of suicide attempt.
Social isolation is a major cause of loneliness,33 and the physical isolation measures implemented during the COVID-19 pandemic have been linked to the perception of loneliness.34 Increased loneliness due to physical and social isolation can elevate the risk of depression, anxiety, suicidal ideation, and self-harm among children and adolescents.35 In addition, as shown in Table 1, the higher percentage of adolescents reporting loneliness in 2021 than in 2020 appears to be the result of prolonged social isolation due to quarantine measures and restrictions on social gatherings during the pandemic. Although we did not find reports on how the duration of perceived loneliness influences suicide risk, we speculate that a prolonged feeling of loneliness could significantly impact suicide risk.
To compare changes in risk factors for suicide attempts among adolescents before and after COVID-19, we used 2011–2018 KYRBS data from previous studies.17 Risk factors that tended to decrease in association with suicide attempts were grade (G1, G2) and academic achievement, which may be related to reduced school adjustment and exam stress due to nationwide school closures and shortened school days during 2020–2021. Interestingly, the risk of both factors for suicide attempts increased as school resumed in 2022. On the other hand, the association between smoking and drug exposure, and suicide attempts was clearly increased in 2020 compared to the pre-COVID-19 period, which may be related to difficulties in getting adequate attention and control for healthy growth at home or in the community during school closures. There was also a trend toward increased risk of hopelessness for suicide attempts, likely due to limited screening process in schools and mental health services during 2020–2021 and a lack of timely therapeutic linkages.2936 As suicidal ideation and suicide attempt rates have been increasing year over year since 2020, post-COVID-19 public health policy and interventions need to take into account the changes in risk of the above-mentioned factors associated with suicide attempts among youth.
There are limitations in this study. One pertains to the reliance on retrospective self-report surveys because they may be susceptible to recall bias or underreporting. Another limitation is the absence of data for comparing the feeling of loneliness before the COVID-19 pandemic as this variable was introduced for the first time in 2020. Similarly, the lack of data on financial stress during COVID-19 pandemic and drug exposure in 2022 also hinders our ability to confirm sustained trend in these variables. In addition, while this study addressed risk factors associated with the COVID era, it did not account for other confounding factors, including adverse childhood experiences, personality, and protective factors.61337
In conclusion, the changes brought upon by the COVID-19 pandemic certainly impacted the mental health of adolescents, particularly in relation to suicide risk. The study provides insights into the impact of these factors on adolescent mental health because the results demonstrated an elevated risk of suicide attempt among adolescents who experienced financial stress and reported feelings of loneliness during the pandemic. Although financial aid may have weakened the association between family financial stress and suicide risk, adolescents experiencing loneliness showed elevated risks of suicide attempt, indicating that the interventions for social isolation and loneliness were inadequate. As the COVID-19 pandemic comes to an end, it is critical to introduce more specific screening techniques to determine adolescent suicide risk and implement appropriate interventions.
 XML Download
XML Download