

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Few years into the coronavirus disease 2019 (COVID-19) pandemic, the COVID-19 vaccines have been widely used to prevent the rapid spread of the disease and severe complications after the infection.12 Pregnant populations were also recommended to receive COVID-19 vaccination given that pregnancy is an independent risk factor for severe COVID-19.345 Moreover, previous studies have shown that pregnant women with COVID-19 have higher risk of severe complications (i.e., intensive care unit admission and death) and the adverse perinatal outcomes (e.g., preterm birth),4678910 although the vertical transmission appeared to occur in minority cases.1112 Accordingly, the US Centers for Disease Control and Prevention recommended COVID-19 vaccination to pregnant populations on 11 August 2021, and Korea Disease Control and Prevention Agency also announced the recommendation in October 2021.313 Similarly, breastfeeding women are recommended to receive COVID-19 vaccination as there are potential benefits including the production of antibodies that can be passed on to the infant through breast milk.14 However, because pregnant and lactating women were largely excluded from the pre-authorization clinical trials of COVID-19 vaccines, potential risk after the COVID-19 vaccination in these populations were of concern.
To date, available evidence on the safety of COVID-19 vaccination during pregnancy and lactation are limited. In preliminary findings, there were no increased risk of adverse events associated with COVID-19 vaccination during pregnancy.15 Following epidemiological studies also showed no significantly increased risk in pregnancy-related outcomes, including spontaneous abortions,1617 miscarriage,18 and preterm birth.1920 However, there is a need to further evaluate the safety of COVID-19 vaccination during pregnancy, as previous studies mainly focused on specific outcomes rather than investigating the overall adverse pregnancy outcomes that can occur during pregnancy or after birth in infants. Likewise, while studies have reported general adverse events after COVID-19 vaccination in lactating women such as swelling and injection site pain,21 additional study is needed to better understand potential lactation-related adverse events or any impact on neonatal health after COVID-19 vaccination.
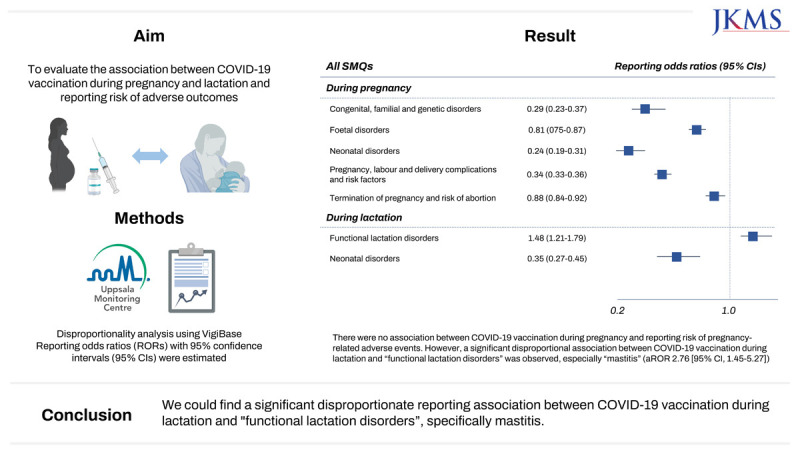
Pharmacovigilance database contains information on adverse drug reactions (ADRs) in real-world setting and have been widely used to detect potential signals associated with drugs.22 Using the global individual case safety reports (ICSRs) database, VigiBase, we aimed to explore the potential associations between the COVID-19 vaccination during pregnancy and lactation and adverse pregnancy-related outcomes.
METHODS
Data source
We performed a pharmacovigilance study using VigiBase, the World Health Organization (WHO)’s global database of ICSRs managed by the Uppsala Monitoring Centre. It contains more than 30 million safety reports of suspected ADRs, submitted by over 150 countries. The database includes information on patient’s demographics, suspected drugs, suspected ADRs coded with Medical Dictionary for Regulatory Activities (MedDRA) terminology, reporter type, and country of origins.23 As the database contains de-identified data, patients’ informed consent was not required.
Data retrieval
Among all deduplicated reports identified from inception to 31 December 2022, we first included all case reports reporting Standardized MedDRA queries (SMQs) of “Pregnancy and neonatal topics”, with COVID-19 vaccines as suspected drug. Among the identified reports, those in women aged 12 to 44 years were selected. When analyzing the safety signals for COVID-19 vaccination during lactation, reports with infants aged below 23 months were additionally included. To retrieve reports associated with COVID-19 vaccination during pregnancy, we used the following preferred terms (PTs) which belong to the SMQs of “Pregnancy and neonatal topics”: “Exposure during pregnancy”, “Foetal exposure during pregnancy” and “Maternal exposure during pregnancy”. Case reports without these PT were excluded to minimize the possibility of including the ADRs not associated with COVID-19 vaccination during pregnancy. In addition, reports with the PT of “Exposure via breast milk” and “Maternal exposure during breastfeeding” were considered as adverse events associated with COVID-19 vaccination during lactation.
Case/non-case design
In this study, we implemented case/non-case design to assess safety signals associated with COVID-19 vaccination during pregnancy and lactation. We identified the cases using the SMQs of “Pregnancy and neonatal topics”, which are validated standard sets of MedDRA terms. The SMQs of “Pregnancy and neonatal topics” are sub-organized by several SMQs: “Congenital, familial and genetic disorders,” “Foetal disorders,” “Neonatal disorders,” “Pregnancy, labour and delivery complications and risk factors (excl. abortions and stillbirth),” “Termination of pregnancy and risk of abortion,” “Lactation- related topics,” and “Normal pregnancy conditions and outcomes.”24
Cases for pregnancy analysis were defined as “Congenital, familial and genetic disorders,” “Neonatal disorders,” “Termination of pregnancy and risk of abortion,” “Pregnancy, labour and delivery complications and risk factors (excl. abortion and stillbirth),” and “Foetal disorders.” For lactation analysis, “Neonatal disorders” and “Functional lactation disorders” were defined as cases. Non-cases were all other reports in the VigiBase.
Statistical analysis
Disproportionality analysis was conducted to evaluate whether adverse events were differentially reported for the COVID-19 vaccine during pregnancy and lactation compared to the full database. Reporting odds ratios (RORs) with 95% confidence intervals (CIs) of adverse outcomes were estimated using logistic regression models, while adjusting for maternal age. We also adjusted for infant age and infant sex when assessing the reporting risk associated with COVID-19 vaccination during lactation. To be identified as a signal, the lower limit of the ROR’s 95% CI had to be higher than 1.00, and also the number of cases should be more than 5 to reduce false positives.25 All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Sensitivity analyses
In sensitivity analyses, we assessed safety signals of COVID-19 vaccines by using the influenza vaccines as comparator group, instead of all other drugs in the database. Although we used full database as comparators in our main analysis to reduce the false positivity,26 evaluating the safety profile of COVID-19 vaccines as compared with other vaccines may provide further relevant evidence. Because previous studies have shown that influenza vaccination during pregnancy or lactation were not associated with adverse outcomes, influenza vaccines were selected as the comparator group.27282930 Additionally, we restricted the ICSRs notified by physicians to examine the robustness of our main findings.
Lastly, as a post-hoc analysis, we further analyzed the “functional lactation disorders” at a PT level, which was identified as a potential signal associated with COVID-19 vaccination during lactation.
RESULTS
Characteristics of reports
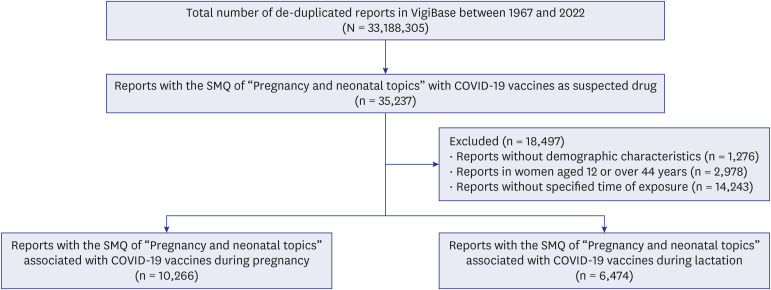
From inception through 31 December 2022, there were 33,188,305 ICSRs reported in the database. After applying the exclusion criteria, 16,740 reports reporting SMQs of “Pregnancy and neonatal topics” with COVID-19 vaccines as suspected drug remained; 10,266 reports associated with COVID-19 vaccine during pregnancy and 6,474 reports associated with COVID-19 vaccine during lactation (Fig. 1). As COVID-19 vaccines were first commercialized on December 11, 2020,1 all the reports associated with COVID-19 vaccines were reported from 2021.
Fig. 1
Flowchart of reports with COVID-19 vaccines during pregnancy and lactation.
SMQ = Standardized Medical Dictionary for Regulatory Activities Query, COVID-19 = coronavirus disease 2019.
Overall, most of the safety reports associated with exposure during pregnancy were reported from women aged 18 to 44 years (n = 10,215 [99.5%]) and were from the Region of the Americas (n = 5,616 [54.7%]) and Europe (n = 4,309 [42.0%]) (Table 1). Except for the reports without notifiers, the reports were mostly notified by consumer or other non-health professionals.
Table 1
Baseline characteristics of “pregnancy and neonatal topics” reports with COVID-19 vaccines
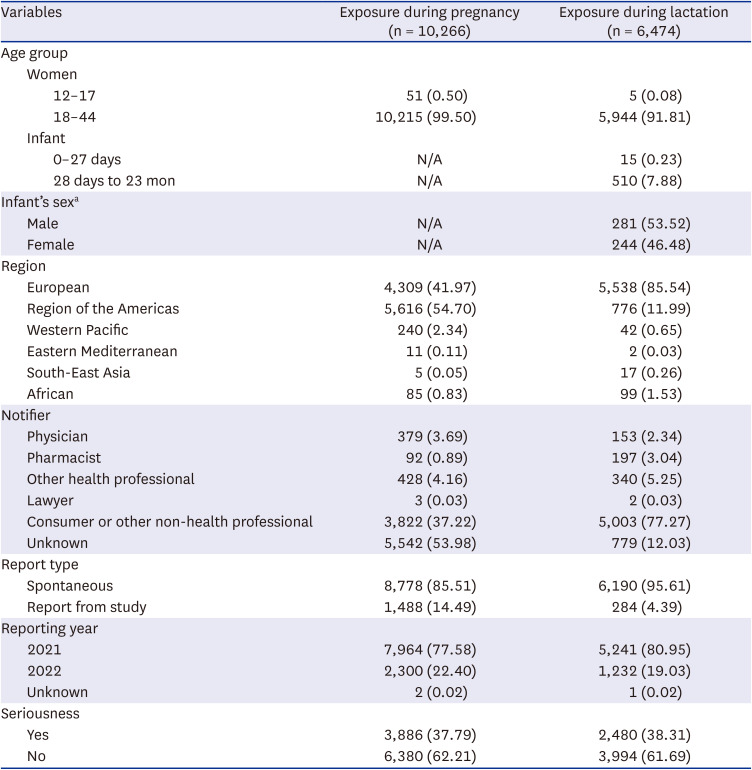
Likewise, majority of the safety reports associated with COVID-19 vaccines during lactation were reported from women aged 18 to 44 years (n = 5,944 [91.81%]). Of 565 reports reported from the infants, 281 (53.5%) were from male infants. The reports were mainly originated from Europe (n = 5,538 [85.5%]) and were notified by consumer or other non-health professionals (n = 5,003 [77.27%]).
Adverse events associated with COVID-19 vaccine during pregnancy
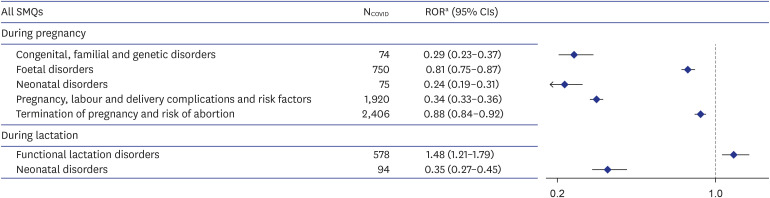
There were no significant disproportional associations between the COVID-19 vaccines during pregnancy and the SMQs of “Pregnancy and neonatal topics”; the adjusted ROR (aROR) was 0.29 (95% CI, 0.23–0.37) for congenital, familial and genetic disorders, 0.81 (0.75–0.87) for foetal disorders, 0.24 (0.19–0.31) for neonatal disorders, 0.34 (0.33–0.36) for pregnancy, labour, and delivery complications and risk factors, and 0.88 (0.84–0.92) for termination of pregnancy and risk of abortion (Fig. 2).
Fig. 2
Disproportionality analysis on the SMQs of “Pregnancy and neonatal topics” associated with COVID-19 vaccines during pregnancy and lactation.
SMQ = Standardized Medical Dictionary for Regulatory Activities Query, NCOVID = number of reports with COVID-19 vaccine as suspected drug, ROR = reporting odds ratio, CI = confidence interval, COVID-19 = coronavirus disease 2019.
aFor pregnancy analysis, maternal age was adjusted and for lactation analysis, maternal age, infant age, and infant sex were adjusted.
Adverse events associated with COVID-19 vaccine during lactation
However, as described in Fig. 2, the “Functional lactation disorders” showed a significant disproportionate reporting for COVID-19 vaccines during lactation (aROR, 1.48 [95% CI, 1.21–1.79]), whereas the SMQ of “neonatal disorders” did not show significant aROR (0.35 [0.27–0.45]).
Functional lactation disorders associated with COVID-19 vaccines
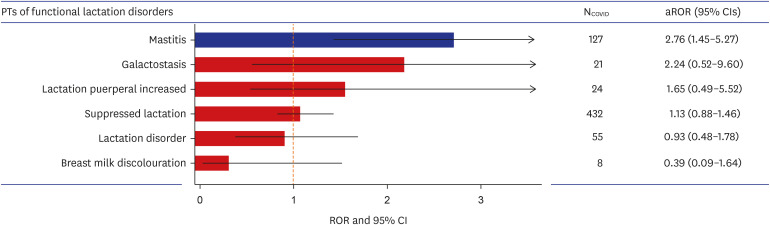
Additional analysis was conducted for the SMQ of “Functional lactation disorders” at a PT level, associated with COVID-19 vaccine during lactation. We identified a significant disproportionality signal for mastitis associated with COVID-19 vaccine during lactation, with aROR (95% CI) of 2.76 (1.45–5.27) (Fig. 3). Other PTs showed no significant reporting risk.
Fig. 3
Disproportionality analysis for reporting “Functional lactation disorders” associated with COVID-19 vaccines during lactation at a PT level.
PT = preferred term, NCOVID = number of reports with COVID-19 vaccine as suspected drug, aROR = adjusted reporting odds ratio, CI = confidence interval, COVID-19 = coronavirus disease 2019.
Sensitivity analyses
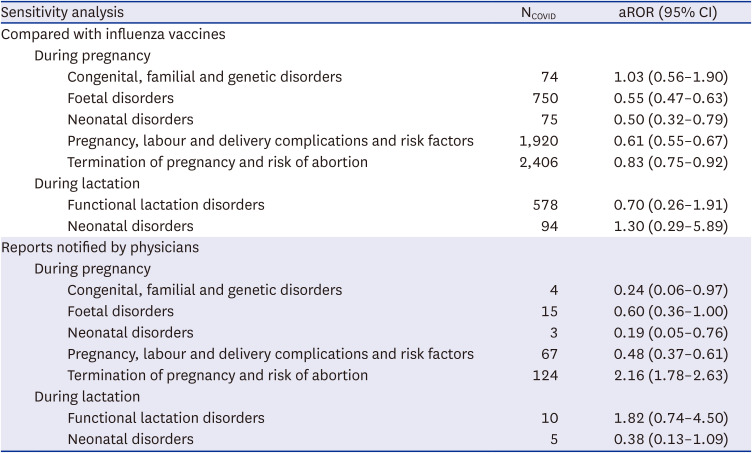
Sensitivity analyses generally showed consistent results with our main analyses (Table 2). When compared with influenza vaccines, there were no disproportional signals associated with COVID-19 vaccines during pregnancy and lactation. Also, similar results were observed in analyses restricting the reports notified by physicians, except for small increased reporting risk observed for “termination of pregnancy and risk of abortion” associated with COVID-19 vaccination during pregnancy.
Table 2
Sensitivity analyses on the risk of reporting SMQs of “Pregnancy and neonatal topics”
DISCUSSION
Previous study has reported that the most common reason for COVID-19 vaccination hesitancy in pregnant women was concern that COVID-19 vaccine might affect the fetus.31 In light of this and the limited available evidence on the safety of COVID-19 vaccine, our study used the global WHO database of ADRs and investigated the potential signals associated with COVID-19 vaccination during pregnancy or lactation. We utilized the SMQs of “pregnancy and neonatal topics”, which are predefined sets of MedDRA terms that are associated with the pregnancy or neonatal-related conditions, to detect any potential signals. Overall, we did not identify any disproportional signal on pregnancy-related adverse events associated with the COVID-19 vaccine during pregnancy; however, there was significant disproportionate reporting of “functional lactation disorders” associated with the COVID-19 vaccine during lactation, with an aROR (95% CI) of 1.48 (1.21–1.79). Further analysis that analyzed “functional lactation disorders” at a PT level, showed higher ROR in mastitis (2.76 [95% CI, 1.45–5.27]).
Our findings are supported by the previous epidemiologic studies and review articles which found no association between COVID-19 vaccination during pregnancy and adverse pregnancy-related outcomes.532333435 Because pregnant women are typically excluded from the randomized clinical trials owing to ethical restrictions, information on the vaccines safety during pregnancy mostly relies on the observational studies.32 Earlier meta-analysis on the perinatal outcomes of COVID-19 vaccination in pregnancy found no evidence of a higher risk of adverse outcomes (e.g., miscarriage, postpartum haemorrhage, low birth weight) associated with COVID-19 mRNA vaccination in pregnancy.33 Similar results were found by subsequent cohort study using the pregnancy registry of Sweden and Norway.34 This study observed no significantly increased risk of adverse pregnancy outcomes including preterm birth, stillbirth, and low Apgar score among individuals vaccinated against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) during pregnancy compared with those without SARS-CoV-2 vaccination during pregnancy. Another population-based cohort study in Canada reported that COVID-19 vaccination during pregnancy, primarily mRNA vaccines administered in the second and third trimester, was not associated with an increased risk of adverse peripartum outcomes.35 In our study, we performed a disproportionality analysis using the largest pharmacovigilance database and did not find any significant signals associated with COVID-19 vaccination during pregnancy. According to the KCDC reports, the most common adverse events reported from the pregnant women was headache (n = 10) followed by stomachache (n = 10) and muscleache (n = 8), which is relatively mild.36 Considering these results together in alignment with the current recommendation, COVID-19 vaccination during pregnancy should be considered when the expected benefits are considered to outweigh the potential risks.37383940
However, we found an increased reporting risk of “functional lactation disorder”, specifically mastitis, associated with COVID-19 vaccination in lactating women. To date, limited number of studies have investigated the safety of COVID-19 vaccination during lactation. An online prospective cohort study in U.S reported that COVID-19 vaccines were well-tolerated among the lactating women.41 Another study based on self-reported online questionnaire found no severe adverse events for mothers or infants after COVID-19 vaccination during lactation.42 In the previous studies, the most frequently reported adverse events after COVID-19 vaccination during lactation were injection site pain, fatigue, and headache, which are relatively mild and similar to those observed in the general population. On the other hand, lactation related adverse events such as mastitis and suppressed lactations were not commonly reported. One study of lactating healthcare workers in Singapore reported that three of 88 (3.4%) participants had mastitis after two doses of BNT162b2 (Pfizer/BioNTech) vaccination,43 whereas in another cross-sectional survey, 0.2% of breastfeeding mothers reported a mastitis after COVID-19 vaccination.42 Given that the incidence of mastitis in the general breastfeeding population ranges from 2.5% to 20%, further studies should be conducted to confirm whether COVID-19 vaccination during lactation is associated with mastitis. Meanwhile, according to one case report of post COVID-19 vaccine mastitis, the type of mastitis was self-limited and the symptom spontaneously disappeared in 6 days.44 Therefore, while awaiting for additional studies to confirm the safety of COVID-19 vaccination during lactation, COVID-19 vaccine should be considered in lactating women based on the recommendation of the CDC and WHO.4546
To the best of our knowledge, this is the first study using the world’s largest pharmacovigilance database to examine the pregnancy and lactation related adverse events in association with COVID-19 vaccination as providing a quantitative measure of the ROR in comparison to all other drugs. Although several well-conducted epidemiological studies16172035 have addressed the safety of COVID-19 vaccination during pregnancy, limited evidence exists regarding the safety of COVID-19 vaccination during lactation.4748 Moreover, disproportionality analysis, a validated method used in drug safety studies, would still be informative to detect any potential signals associated with COVID-19 vaccination during pregnancy that may not have been the outcomes of interest in previous cohort studies.
This study has several limitations which are mostly inherent to studies using a pharmacovigilance database. First, given the spontaneous nature of ADR reporting in VigiBase, underreporting is unavoidable. However, the effect of underreporting would be low to change the results of the disproportionality analysis.49 Second, information on some variables may be incomplete. In our analysis, we excluded the reports with missing data on the basic demographics such as age and sex. Third, information on the detailed timing of exposure during pregnancy (e.g., trimester) and the dose of vaccines were unavailable in the VigiBase. Future studies are needed to assess the safety according to the timing of exposure and the dose effect. Lastly, although we used the global pharmacovigilance database, majority of the reports were originated from Europe and the region of America; thus, the results may not be generalizable to other regions. This may be due to the different policies across the countries regarding the COVID-19 vaccination during pregnancy or lactation. Therefore, additional analysis including the reports from other countries and regions would be beneficial.
This large pharmacovigilance study suggests that COVID-19 vaccination during lactation increased the risk of reporting functional lactation disorders, specifically mastitis, whereas no significant risk of reporting adverse pregnancy outcomes was observed after COVID-19 vaccination during pregnancy. However, considering that COVID-19 vaccine is a newly developed vaccine, continuous surveillance is warranted, especially on the long-term safety, to confirm the safety of COVID-19 vaccine during pregnancy and lactation.
 XML Download
XML Download