

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In order to diagnose lung cancer, we relied on computer-tomography (CT) images. When suspicious lesions are observed on CT, lung cancer is diagnosed through biopsy. According to a previous study, the false positive rate of low dose CT for lung nodule was 94%.1 Although low dose CT is used for lung cancer screening, CT has limitations because the rate of false positive is high. Therefore, biopsy is necessary for diagnosis of lung cancer. Compared with other procedures, bronchoscopy has lower risk for complications.2 However, the sensitivity of peripheral lesion through bronchoscopy including washing cytology is low.3 A new test with higher sensitivity through bronchoscopy is needed.
DNA methylation is an epigenetic mechanism that inactivates cancer suppressor genes and cancer related genes. DNA methylation has been studied as a cancer diagnostic biomarker because it was frequently found in cancer development.4 Recently, DNA methylation is used as a diagnostic tool in various cancers.56 In lung cancer, DNA methylation is used as a marker for diagnosis, treatment, and prediction of prognosis.789 DNA methylation in tissue or body fluid is used recently for diagnosis of lung cancer.9 Many studies have performed diagnosis of lung cancer through DNA methylation in bronchoalveolar lavage fluid (BALF).10
It is known that protocadherin affects tissue development and growth.11 Genes that code for protocadherin can affect the development of various cancers.111213 Hypermethylation of protocadherin gamma subfamily A12 (PCDHGA12) affects various cancers including lung cancer.14 We have found that DNA methylation of PCDHGA12 in bronchial washing cytology has a diagnostic value for lung cancer in a previous study.15 However, its specificity was low although its sensitivity was high.15 Therefore, further study is needed to improve its low specificity.
We used a DNA methylation gene set to make up for the limitation of our previous study and decided to use cysteine dioxygenase type 1 (CDO1). CDO1 is known to affect protein function and antioxidant defense mechanism.16
CDO1 promotor methylation is related to progression and malignancy of various tumors.161718
CDO1 methylation can be used for diagnosis of cancers including lung cancer.192021
We previously reported a highly sensitive and accurate two-step Linear Target Enrichment (LTE)-quantitative methylation specific real-time polymerase chain reaction (PCR) (qMSP) assay (LTE-qMSP) to detect PCDHGA12 methylation using bronchial washing cytology.15 However, this method had limitations, such as the risk of cross-contamination due to the two-step PCR procedure requiring multiple pipetting steps and open-up tubes. In this study, we applied the 3-plex one-step LTE-qMSP assay that uses a single closed-tube reaction to simultaneously detect PCDHGA12 and CDO1 methylation targets DNA. Both PCDHGA12 methylation and CDO1 methylation obtained through bronchial washing cytology were evaluated as a diagnostic tool for lung cancer. Additionally, we analyzed relationships of the combination of PCDHGA12 and CDO1 methylation with clinicopathological parameters including gender, age, cancer location, histology, and staging of lung cancer.
METHODS
Study design
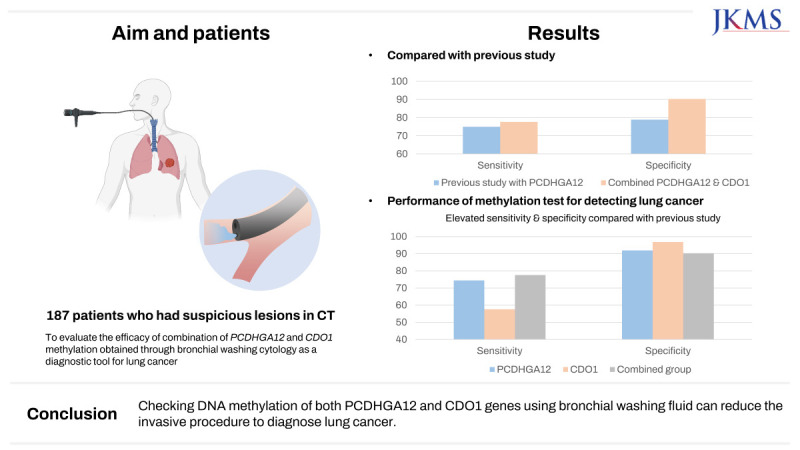
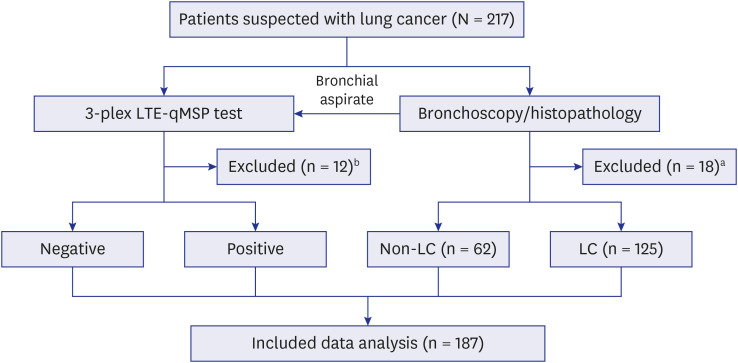
A prospective study was designed to evaluate clinical performance of PCDHGA12 and CDO1 genes for detecting lung cancer using bronchial washing samples. Patients (n = 187) suspected with lung cancer scheduled for bronchoscopy at Konyang University Hospital (Daejeon, Korea) between May 2020 and November 2022 were enrolled. The indications for bronchoscopy of CT images suspected of lung cancer are shown in Table 1. Results of bronchoscopy or histopathology examination were not informed to the personnel involved in the laboratory work. Data analysis of LTE-qMSP results were independently performed to compare bronchoscopy findings and pathology outcomes as reference standards. The outline of this study is illustrated in Fig. 1. Among 217 patients, 12 patients were excluded due to metastatic cancer and 18 patients were excluded due to insufficient samples.
Table 1
Indications for bronchoscopy of CT images suspected of lung cancer
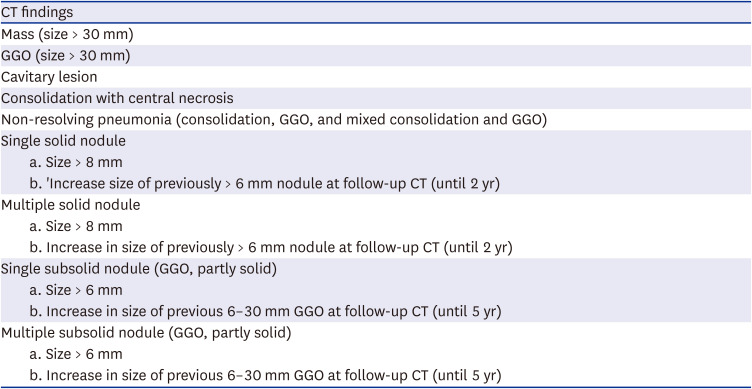
Fig. 1
Flowchart of the combined analysis of protocadherin gamma subfamily A12 and cysteine dioxygenase type 1 DNA methylation for lung cancer.
LTE-qMSP = Linear Target Enrichment-quantitative methylation specific real-time polymerase chain reaction, LC = lung cancer.
aExcluded due to insufficient specimen quantity; bexcluded due to unclear diagnosis or metastatic cancer.
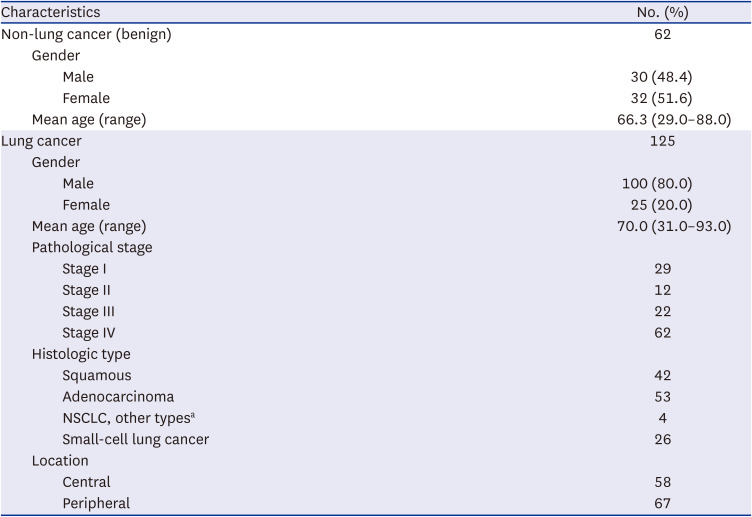
Clinicopathological and demographical characteristics of patients enrolled in this study are shown in Table 2.
Table 2
Clinical and demographic characteristics of the patients test in this study
Bronchial washing samples, DNA isolation, and bisulfite treatment
Fresh bronchial washing samples (10 mL each) were collected into preservative buffer (Genomictree, Inc., Daejeon, Korea) during bronchoscopy. Samples were kept at −20°C until DNA extraction.
Genomic DNA was isolated using a solid phase magnetic bead-based GT NUCLEIC ACID PREP Kit (Genomictree, Inc.) according to the manufacturer’s instructions. The 20 ng of the genomic DNA was then chemically modified with sodium bisulfite using an EZ DNA Methylation Gold kit (Zymo Research, Irvine, CA, USA) according to the manufacturer’s instructions. Bisulfite-converted DNA was purified and eluted with 18 µL of distilled water using a Zymo-Spin IC column (Zymo Research). Eluted DNA was immediately subjected to methylation analysis.15
Measurement of methylation for target genes in bronchial washing samples by 3-plex LTE-qMSP test
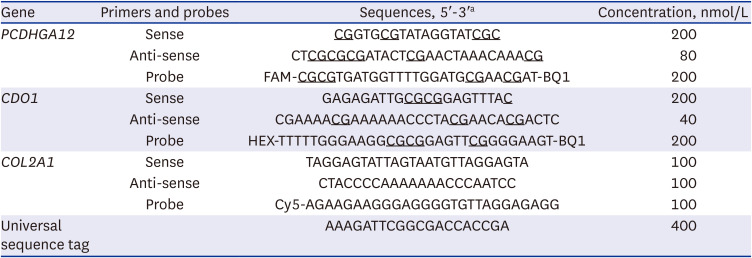
We developed a 3-plex LTE-qMSP test for measuring PCDHGA12 and CDO1 methylation targets and control gene in a single-tube. This test was performed by trained personnel who were unaware of bronchoscopy or histopathology results. A total of 20 ng of genomic DNA was used as an input. A 25 µL reaction mixture contained 5 µL of bisulfite-converted DNA, PCDHGA12 and CDO1 methylation-specific forward primer, PCDHGA12 and CDO1 methylation-specific reverse primer linked to a 5’ universal tag sequence, PCDHGA12 probe (5’-FAM), CDO1 probe (5’-HEX), COL2A1-specific forward and reverse primers, COL2A1 probe (5’-Cy5), universal tag sequence, and 5 µL of 5 x Fast qPCR PreMIX TaqMan Probe (Enzynomics, Inc., Daejeon, Korea). Real-time PCR was performed on an AB7500 FAST Real-Time PCR system (Thermo Fisher Scientific, Waltham, MA, USA). Thermal cycling conditions were as follows: 95°C for 5 minutes; 15 cycles of 95°C for 15 seconds and 70°C for 45 seconds; followed by 35 cycles of 95°C for 15 seconds and 60°C for 45 seconds. Heating and cooling rates were ≥ 4°C per second and ≥ 3.5°C per second, respectively. Primers and probes used for the 3-plex LTE-qMSP test are listed in Table 3.
Table 3
Primer and probe sequences used in the 3-plex Linear Target Enrichment-quantitative methylation specific real-time polymerase chain reaction assay
We performed the 3-plex LTE-qMSP test once for each sample. The relative level of methylated gene in each sample was calculated as 35-△CT [CT of amplified target gene − CT of COL2A1 (human reference gene)].22 Higher values of 35-△CT indicated higher levels of methylation. If the CT of target gene was undetectable, the value was set to 20, the value closest to the lowest 35-△CT for all test results.
Statistical analysis
We calculated receiver operating characteristic (ROC), area under ROC (AUC), and 95% confidence interval (CI) to determine the accuracy, sensitivity, and specificity of diagnosis using the MedCalc software, version 9.3.2.0 (MedCalc Software Ltd., Basel, Belgium). Statistical significance was considered when P value was less than 0.05. To calculate sensitivity and specificity, we categorized test results in a dichotomous manner: methylation-positive as ‘1’ and methylation-negative as ‘0.’ To describe demographic and other clinical characteristics, we used frequency and percentile (%). We also computed negative and positive predictive values.
RESULTS
Clinical and demographic characteristics
A total of 187 patients were enrolled in this study, including 62 patients who were diagnosed with a benign disease and 125 patients who were diagnosed with lung cancer. Benign diseases were confirmed by histological examination through biopsy or improvement of CT lesion after 6 months follow-up. The mean age of patients with a benign disease was 66.3 years and the mean age of patients with lung cancer was 70.0 years. Among 125 lung cancer patients, there were 29 with stage I, 12 with stage II, 22 with stage III, and 62 with stage IV. In lung cancer patients, adenocarcinoma was the most common with 53 cases. Four patients were confirmed to have other types of NSCLC, including carcinoma, mucoepidermoid, neuroendocrine, and pleomorphic carcinoma. There were more peripheral cases than central cases (Table 2).
Diagnostic performance of 3-plex LTE-qMSP test in detecting lung cancer using bronchial washing samples
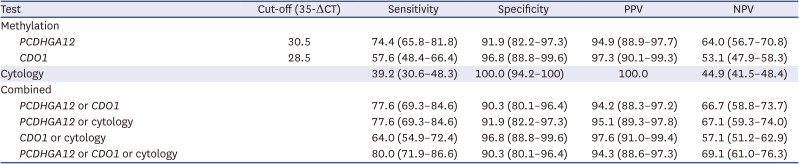
The 3-plex LTE-qMSP test was performed using DNAs from 187 patients composed of 125 lung cancer patients at various stages (I to IV) and 62 non-lung cancer patients. Results revealed that significantly higher levels of PCDHGA12 and CDO1 methylation were present in DNAs from lung cancer patients than in DNAs from non-lung cancer patients (P < 0.001, Kruskal-Wallis test) (Fig. 2). Optimal cutoff values for PCDHGA12 and CDO1 were determined to be 30.5 and 28.5 of 35-△CT for detecting lung cancer, respectively (Fig. 3). For PCDHGA12, its sensitivity and specificity were 74.4% (93/125, 95% CI, 65.8–81.8%) and 91.9% (57/62, 95% CI, 82.2–97.3%), respectively, with an AUC of 0.832 (95% CI, 0.770–0.882, P < 0.001). For CDO1, its sensitivity and specificity were 57.6% (72/125, 95% CI, 48.4–66.4%) and 96.8% (60/62, 95% CI, 88.8–99.6%), respectively, with an AUC of 0.772 (95% CI, 0.705–0.830, P < 0.001). The combination of both genes revealed a sensitivity of 77.6% (97/125 95% CI, 69.3–84.6%) and a specificity of 90.3% (56/62, 95% CI, 80.1–96.4%), with an AUC of 0.840 (95% CI, 0.779–0.889) (Table 4). Cytology achieved a sensitivity of 39.2% (49/125 95% CI, 30.6–48.3%) and a specificity of 100% (62/62, 95% CI, 94.2–100%), with an AUC of 0.696 (95% CI, 0.625–0.761) (Table 4). Combining the two methylation genes and cytology for detecting lung cancer showed an overall sensitivity of 80.8% (101/125, 95% CI, 72.8–87.3%) and a specificity of 90.3% (56/62, 95% CI, 80.1–96.4%), with an AUC of 0.856 (95% CI, 0.797–0.903) (Table 4).
Fig. 2
The DNA methylation level of PCDHGA12 gene (A) and CDO1 (B) in lung cancer patients and non-LC patients.
PCDHGA12 = protocadherin gamma subfamily A12, CDO1 = cysteine dioxygenase type 1, LC = lung cancer.
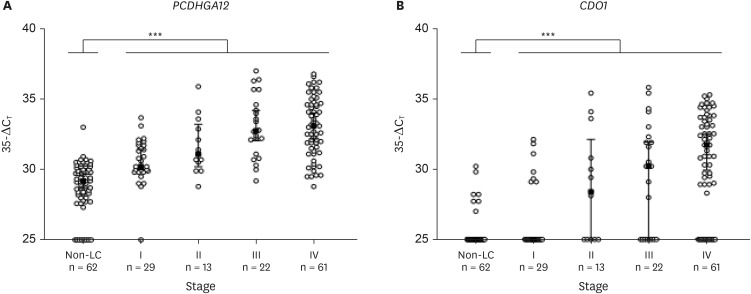
Fig. 3
Receiver operating characteristic curve for PCDHGA12 gene (A) and CDO1 (B) for diagnosing lung cancer in bronchial washing fluids.
PCDHGA12 = protocadherin gamma subfamily A12, CDO1 = cysteine dioxygenase type 1, AUC = area under receiver operating characteristic.
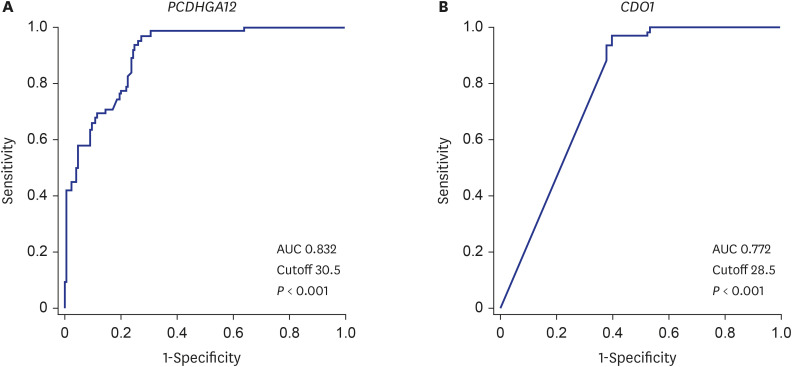
Table 4
Clinical performance of the methylation test and cytology for detecting lung cancer
Subgroup analysis of methylation test and cytology for lung cancer
Results of subgroup analysis for lung cancer patients are shown in Table 5. Compared with PCDHGA12 methylation test, combined test for methylation of both genes showed a higher sensitivity in males (81.0%), those with age ≥ 65 years (81.3%), those with a central location (94.7%), those with SCLC (90.9%), and those with stages III–IV (88.0%). Combining methylation of both genes and cytology had a significant diagnostic value for central lung cancer (sensitivity 94.7%, P < 0.001) and stage III–IV lung cancer (sensitivity 91.6%, P < 0.001). In all subgroup analyses, the sensitivity was higher when combining methylation tests for both genes than PCDHGA12 or CDO1 methylation test alone and cytology alone. Table 6 shows results according to the location of lung suspicious lesion. There was no significant difference in DNA methylation according to the location of suspicious lesion. In this study, there were 10 patients who underwent surgery without biopsy for histological confirmation, of which 8 were diagnosed with cancer and the other 2 had a non-cancerous disease.
Table 5
The relationship between clinicopathological parameters, methylation and cytology in bronchial aspirate samples from 125 lung cancer patients
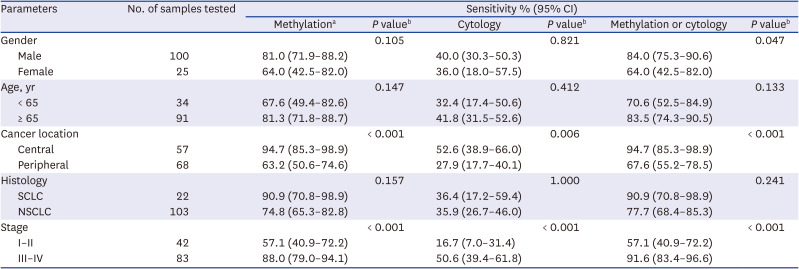
Table 6
The relationship between mass location, methylation and cytology in bronchial aspirate samples from 125 lung cancer patients

DISCUSSION
In our previous study, PCDHGA12 methylation for diagnosing lung cancer had a sensitivity of 75.0%, a specificity of 78.9%, a positive predictive value of 84.9%, and a negative predictive value of 66.7%.15 Compared with our previous study, the sensitivity and specificity were increased by combining methylation of both genes in the present study. The positive predictive value of combining methylation of both PCDHGA12 and CDO1 was also superior to that of the previous PCDHGA12 methylation test, although the negative predictive value of combining methylation of both PCDHGA12 and CDO1 was not inferior to that of the PCDHGA12 methylation test in the previous study. Additionally, when methylation of both genes was combined with cytology, sensitivity, specificity, positive predictive value, and negative predictive value all showed better results. According to previous studies on DNA methylation and lung cancer diagnosis, sensitivity was increased by adding different types of methylation markers compared to lung cancer diagnosis through a single DNA methylation marker.102324 In the present study, the sensitivity was increased by combining methylation of PCDHGA12 and CDO1 compared with our previous study.15
In this study, we improved the specificity of the methylation test as compared to our previous study. In the previous study, we used a two-step LTE-qMSP method to measure methylation in bronchial washing samples. However, this method involves open tubes and multiple pipetting steps, which increases the risk of cross-contamination and prolonged assay time. To overcome these limitations, we employed a one-step LTE-qMSP assay using a single closed-tube reaction to simultaneously detect multiple methylated targets of DNA.25 This method has several advantages such as low false-positive and negative rates and minimal risk of PCR contamination.
Lung cancer is diagnosed through low dose CT and biopsy. As mentioned earlier, low dose CT has high false positive rate and biopsy has many complications.1 Biopsy through bronchoscopy is difficult to find the exact bronchus that has lesion.26 Recently, many studies are being conducted to diagnose lung cancer with non-invasive tests such as liquid biopsy to minimize complication through invasive test including bronchoscopy biopsy and surgical biopsy.2728 A liquid biopsy is a test for confirming substances present in blood or bodily secretion. Through liquid biopsy, lung cancer can be diagnosed by confirming circulating tumor cells, circulating tumor DNA, exosome, and microRNA in blood or bodily fluids including bronchial washing cytology.27 However, bronchial washing cytology has limitation in screening or diagnosis for lung cancer due to its low sensitivity.29 Therefore, finding a new tumor marker that can suggest lung cancer with a high sensitivity is needed to reduce invasive tests and supplement the false positive rate of a low-dose CT.
Previous studies on bronchoscopy have used BALF.103031 BALF analysis is invasive. It can induce several complications to patients including respiratory failure, bronchospasm.32 To diagnose lung cancer, percutaneous transthoracic needle aspiration biopsy can also induce complications including pneumothorax and air embolism.3334 In this study, we used simple bronchial washing fluid. It is less invasive than other procedures with complications. If data on DNA methylation tests through bronchial washing fluid are accumulated, invasive tests such as BALF analysis and percutaneous transthoracic needle aspiration biopsy for lung cancer diagnosis can be reduced. Through reducing the invasive tests, there are some advantages including lesser costs, shorter hospital days and lesser complications.35
Recent studies have tried to diagnose lung cancer through DNA methylation.789 In our previous study, we found that methylation of PCDHGA12 had a diagnostic value of lung cancer.15 Compared with our previous study, the sensitivity was increased by combining methylation of CDO1 and the specificity was increased by changing technological method. According to this study, it was found that diagnosis through bronchial washing cytology and both gene methylation can be helpful in increasing the diagnosis rate of lung cancer.
This study has several limitations. The small sample size was the first limitation. A total of 187 patients were enrolled. Statistical limitations could not be ruled out due to the small sample size. In subgroup analysis, some subgroups including male, central location lung cancer, and stage III–IV lung cancer has a significant diagnostic sensitivity. However, other groups dividing by age or histology did not show any significant difference in sensitivity. Further study is needed to overcome the limitation of subgroup analysis in this study. To increase the diagnostic value of lung cancer through DNA methylation, it is important to find optimal combination of DNA methylation. This study did not combine with methylation of other DNAs known to be associated with lung cancer including SOX17, TAC1, HOXA7, and RASSF1A.10363738 Lastly, in this study, a statistically significant increase in sensitivity was shown as the stage of the patients in the subgroup progressed, with 57.1% in stages I and II compared to 88% in stage III and IV of lung cancer. The sensitivity of this study increases as the stage progresses, however patients with advanced lung cancer require biopsy for chemotherapy rather than surgery. Hence, the DNA methylation method will be more beneficial for screening rather than having a significant impact on diagnosis and treatment.
In conclusion, the sensitivity for lung cancer diagnosis was increased after combining results of both PCDHGA12 and CDO1 methylation tests. Therefore, checking DNA methylation of both genes using bronchial washing fluid can reduce invasive procedure for diagnosing lung cancer.
 XML Download
XML Download