

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to the Korean national health and nutrition examination survey, an average of 8.1% of Korean children and adolescents under the age of 20 responded that they had experienced non-fatal injuries.1 The mortality rate due to external cause is 21.2 for 0-year-olds, 2.7 for 1–9 year-olds, and 10.1 for 10–19-year-olds per 100,000 population in 2021.2 Korea’s preventable trauma death rate is decreasing from 35.2% in 2012 to 15.7% in 2019, but is still at a high level.345 Korea’s trauma system is currently in the stage of construction, starting with the designation of regional trauma centers in 2012. The introduction of a regional trauma center reduced the mortality rate,678 but the transfer rate between hospitals increased.7 Regional trauma centers remain in operation, but there is no transport protocol for trauma patients in prehospital and hospital stage.
Various studies have reported on the effect of inter-hospital transfer on the prognosis of pediatric trauma patients. Locke et al.9 demonstrated no difference in the mortality or complication rate between a direct visit group and inter-hospital transfer group in Canada, and Odetola et al.10 reported a lower mortality rate in a direct visit group in US mountain states. Although the trauma system is developing, there is no dedicated pediatric trauma center in Korea, and there is insufficient research on the impact of inter-hospital transfer on the prognosis of pediatric patients. Therefore, we investigated the association of hospital transfer on the prognosis and prognostic factors by comparing direct visit and transfer groups of Korean pediatric injury patients.
METHODS
Study design and setting
This was a retrospective observational study that analyzed data from the Emergency Department-based Injury in Depth Surveillance (EDIIS) (2020), Korea Center for Disease Control and Prevention, in which 22 regional and local emergency centers in Korea are participating as of 2022. The EDIIS is an emergency room-based prospective data collection system managed by Korea Center for Disease Control and Prevention, which has been encouraging voluntary participation in hospitals nationwide since 2016.
Participants
The subjects were patients aged < 18 years who visited the emergency room with injuries including motor vehicle collision, falls, slip down, collision with objects and etc., poisoning, chemical contact, hanging, asphyxia, drowning, others from January 2013 to December 2017. Patients discharged from the emergency room, those who visited the hospital > 48 hours after trauma, those whose injury time was not recorded, those whose disposition was not known, those who were referred from outpatient department, those whose routes of visit is not recorded, and those who were transferred to another hospital were excluded.
Variables
The variables included in the analysis were age, gender, time of injury, time of emergency room visit, intentionality of injury, mechanism of injury, excess mortality ratio-adjusted injury severity score (EMR-ISS), head trauma (main diagnosis in International Classification of Diseases, 10th Edition code), presence of surgery during hospitalization, whether or not the patient died, date and time of death, and length of hospitalization. The EMR-ISS is an injury severity scale adapted from the International Statistical Classification of Diseases and Related Health Problems 10th Revision, Clinical Modification.11 The EMR-ISS was calculated as the sum of the squares of the three highest EMR grades among all injury codes11: EMR-ISS = (First Highest EMR Grade)2 + (Second Highest EMR Grade)2 + (Third Highest EMR Grade)2. Each EMR is assigned as one of five grades of severity by quintiles, which we termed minimal, mild, moderate, severe, and critical. All injury episodes were classified into three groups: mild (1 ≤ EMR-ISS ≤ 8), moderate (9 ≤ EMR-ISS ≤ 24), severe (25 ≤ EMR-ISS) in the study. Mortality was classified as death within 4 hours after injury, death within 30 days after injury and overall death. The visit time to the emergency room was classified as regular hours (8 am to 5:59 pm) or non-regular hours.
Outcomes
The primary outcome measure was 30-day mortality and the secondary outcome was 72 hour mortality after injury.
Statistics analysis
SPSS software (version 27.0; SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The χ2 test and Fisher’s exact test were used to analyze categorical variables, and median and interquartile range values were calculated for continuous variables. The Mann-Whitney U test was also performed. To compare the survival rates of the direct admission group and the inter-hospital transfer group, survival analysis was performed excluding patients who died within 4 hours after injury among all deaths. A Kaplan-Meier survival curve was used to compare survival between the direct visit and inter-hospital transfer groups, and Cox proportional regression was performed for the risk factor analysis. In the survival analysis, the time period analyzed was that between injury and hospital discharge. P values < 0.05 were considered significant.
RESULTS
Among the 444,817 injured patients aged < 18 years who visited the hospital during the study period, 18,518 were included in the analysis (Fig. 1). In total, there were 15,831 patients (85.5%) in the direct hospital visit group and 2,687 (14.5%) in the inter-hospital group. The median age was 8 years in the direct visit group and 10 years in the inter-hospital group. The 0–4-year-old subgroup was the largest in the direct visit group, while the relative proportions of 5–9- and 15–17-year-olds were larger in the transfer group. The mechanism of injury was different between the direct visit and transfer groups. In the direct visit group, falls and slips (41.5%) were the most common causes of injury, whereas traffic accidents (48.1%) were the most common cause in the transfer group. Intentional injury accounted for 4.9% of all injuries, and no difference was observed in the rate of intentional injury between the two groups. Both groups had a higher proportion of boys than girls. The EMR-ISS was significantly higher in the inter-hospital group than the direct visit group (25 vs. 16, P < 0.001), and the proportion of head trauma cases was higher in the transfer group (35.6%) than direct visit group (26.2%; P < 0.001). A total of 422 deaths (2.3%) were recorded during the study period, of which 258 (1.4%) occurred in the emergency room and 203 children died within 4 hours after injury. Operation was performed in 35.9% of all patients, and the median hospital stay was 5 days. Overall mortality, emergency department (ED) mortality, 72-hour mortality, and 30-day mortality rates were significantly higher in the transfer than direct visit group. The mortality rate within 4 hours after injury was 1.1% in both the direct visit group and the inter-hospital transfer group, with no significant difference. The length of hospital stay in the hospital was also significantly higher in the transfer group (P < 0.001) (Table 1).
Fig. 1
Study participants.
EDIIS = Emergency Department-based Injury in Depth Surveillance, ED = emergency department.
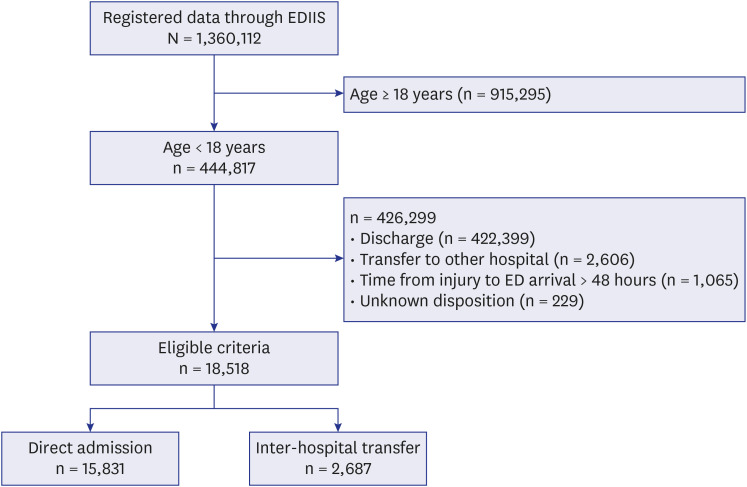
Table 1
Univariable analysis of direct visit group and inter-hospital transfer group
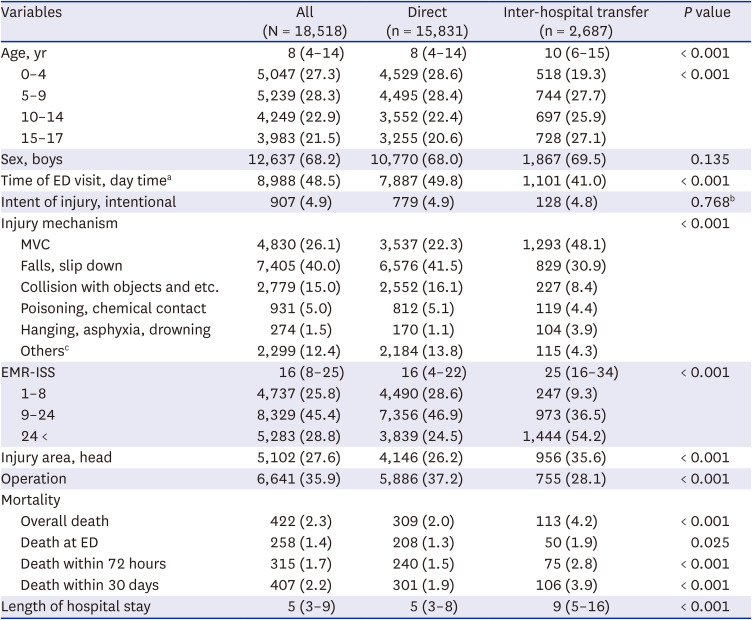
Values are presented as median (interquartile range) or number (%).
MVC = motor vehicle collision, EMR-ISS = excess mortality ratio-adjusted injury severity score, ED = emergency department
aDay time was defined as from 08:00 to 17:59.
bFisher’s exact test.
cPenetrating, machine related, thermal injury, overexertion, unspecified and unknown.
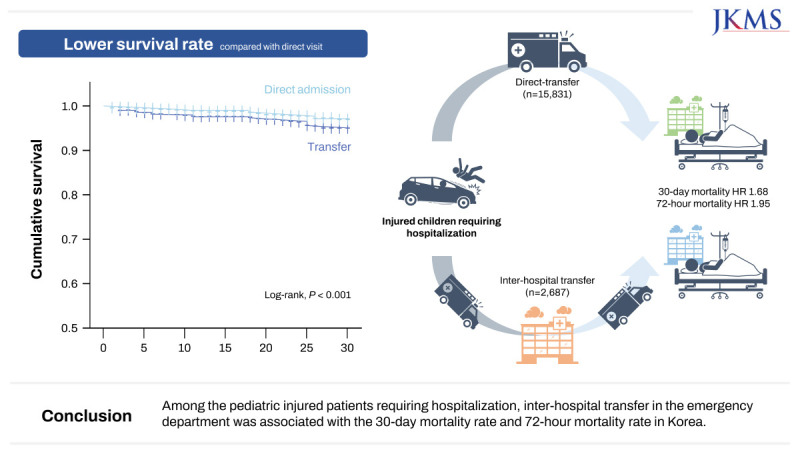
The Kaplan-Meier survival curve revealed that the 30-days survival rate of the transfer group was significantly lower than that of the direct visit group (log-rank, P < 0.001) (Fig. 2). Cox proportional hazards regression analysis was performed to analyze the factors affecting the prognosis of the direct visit and transfer groups (Table 2). Adjusting age, sex, severity (EMR-ISS), time of ED visit, head injury, inter-hospital transfer was associated with 30-day mortality and 72-hour mortality (hazard ratio [HR], 1.681; 95% confidence interval [CI], 1.232–2.294 and HR, 1.951; 95% CI, 1.299–2.930).
Fig. 2
As a result of Kaplan-Meier survival curve analysis, the 30-day survival rate of the interhospital transfer group was significantly lower than that of the direct hospitalization group (log-rank test, P < 0.001).
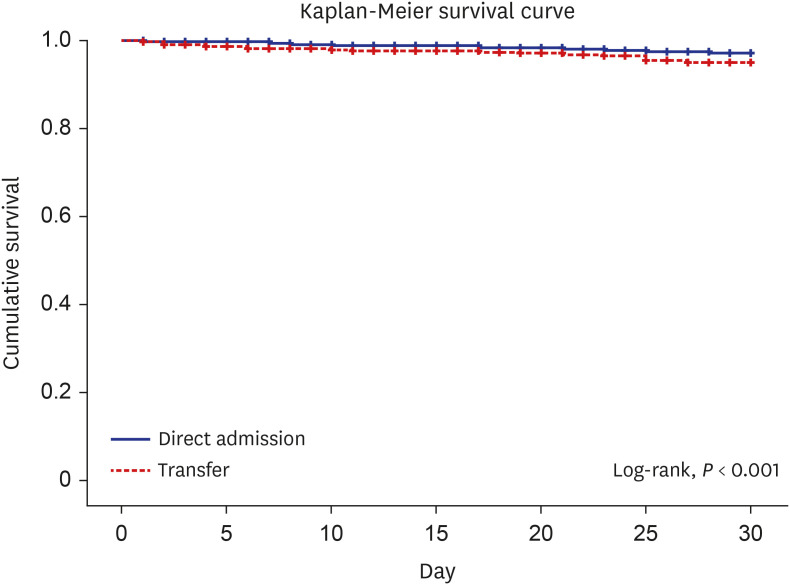
Table 2
Cox proportional hazard regression for mortality at 72-hours and 30-days excluding death within 4 hours after injury

DISCUSSION
As a result of analyzing the association between the prognosis of injured patients and inter-hospital transfer for pediatric patients requiring hospitalization, the 30-day mortality and 72-hour mortality rate were higher in the inter-hospital transfer group compared to the direct visit group. With similar results to this study, a meta-analysis published in 2022 found that the mortality rate was higher in the transfer than direct visit groups of 17 studies from nine low- and middle-income countries (odds ratio, 1.55; 95% CI, 1.12–2.15; P = 0.009).12 In a study conducted in a pediatric Level 1 trauma center located in a US mountain state, the mortality rate was lower in the direct visit than transfer (from 22 nearby hospitals) group (0.4% vs. 3.6%).10 The mortality rate was three times higher in the transfer than direct visit group after adjusting for severity. Contrary to our findings, a study found that no significant difference in mortality or complications between transferred and direct patients after adjusting for injury severity at the Children’s Hospital of Ontario Tertiary University, although the treatment period was longer in transfer group.9 In a systematic review published in 2011, differences in mortality between trauma transfer and direct visit groups were difficult to confirm.13 However, there were limitations in that study, as only two included pediatric subjects. One of those studies showed that that air transport was more advantageous after the patient had been stabilized in the hospital.1415 Based on the research results to date, it is difficult to determine the effect of inter-hospital transfer on general pediatric trauma patients. Thus, even in a country with a well-established trauma treatment system, the effect of transfer among hospitals depends on regional characteristics.5
In this study, mortality rates were compared excluding patients who died within 4 hours after injury. This is because the cause of early death after initial injury is due to a serious injury mechanism,16 so it was not thought to be an appropriate target for examining the impact of inter-hospital transfer. Even after adjusting for gender, age, severity, time of visit, and presence of head injury, the 72-hour mortality rate was 1.9 times higher and the 30-day mortality rate was 1.6 times higher in the inter-hospital transfer group. In other words, the results can be seen as suggesting a correlation between inter-hospital transfer and death within the current Korean trauma system, and the correlation is particularly high with death within 72 hours after injury.
In this study, inter-hospital transfer patients accounted for 14.5% of the injured patients, and the rate was similar (13.2% to 15.7%) over 5 years. In particular, there were many traffic accident patients, high EMR-ISS, and many head injury patients. Considering that all participant hospitals are university hospitals, there are many places that do not provide appropriate treatment for children’s injuries, and that appropriate hospitals that can provide treatment are not properly selected at the accident site. Several studies have already shown that patients triaged directly to trauma centers have improved outcomes compared to patients initially transferred to non-trauma hospitals.1718 The American College of Surgeons Committee on Trauma (ACSCOT) has recommended under-triage rate of < 5% and the Dutch Healthcare Institute dictates an under-triage of less than 10% in trauma system.1920 Therefore, Korea needs an on-site triage protocol that can reduce unnecessary transfers between hospitals by selecting an appropriate hospital on site.
Several studies have reported hypotension, respiratory problems, equipment-related problems, cardiac arrest, and infections as adverse events associated with inter-hospital transfers.2122 Efforts are being made to resolve these problems, including the deployment of professional transfer teams. Previous studies have reported that transport by specialized teams reduces mortality.2324 Therefore, pediatric transfer teams (PTTs) are being introduced in developed countries. Calhoun et al.24 reported that Pediatric trauma patients transferred through PTT were younger, had higher Injury Severity Score (ISS), lower Glasgow Coma Scale (GCS), and longer transfer time, but there was no significant difference in length of stay during transfer and incidence of adverse events during transfer compared to the group not transferred through PTT.24 Considering the higher mortality rate in the interhospital transfer group compared to the direct transfer group in the results of the study, it is necessary to investigate the reason for the high mortality rate in the transfer group. It is also necessary to consider organizing and operating a pediatric transfer team in order to minimize adverse effects during transport.
This study had several limitations. First, it is difficult to generalize the results, as we did not include pediatric injury patients from all emergency rooms in Korea. Nevertheless, the data were obtained from 22 university hospitals and study population had a median EMR-ISS score of 16, and more than 75% of them had a median EMR-ISS score of 9 or higher. Also, there were 422 deaths of patients aged < 18 years in this study, accounting for > 10% of all deaths caused by external causes among Korean children and adolescents during the study period.25 Therefore, the results of this study may be representative to some extent, including a significant number of patients with moderate to severe injuries in Korea. Second, the EMR-ISS used as a severity index in this study is a diagnosis-based severity tool that reflects the anatomical injury area, and has the limitation of not reflecting physiological indicators such as vital signs or consciousness that are important in assessing severity. In this study data, there were many missing values for vital signs and GCS, so they could not be reflected in the analysis. Therefore, it seems necessary to correct the severity using various indicators such as more appropriate tools that reflect the severity or physiological indicators such as Revised Trauma Score and GCS. Third, Since this study is an observational study, there are unmeasured confounders. In particular, information related to the transfer is omitted: level of the referring hospital, time of arrival at the hospital, transfer process (use of ambulance, boarding of medical personnel, time required for transfer), etc. In addition, the level of urbanization of the area where the injury occurred and the socioeconomic status of the patient were not included. Fourth, In addition to mortality, disability (Glasgow Outcome Scale) and occurrence of complications are important outcome variables in injured patients, but these were not measured. However, the length of hospitalization was investigated, and it was confirmed that the hospitalization period was longer in the transfer group compared to the direct visit group.
Among the pediatric injured patients requiring hospitalization, inter-hospital transfer in the emergency department was associated with the 30-day mortality rate and 72-hour mortality rate in Korea.
 XML Download
XML Download