

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has been ongoing since December 2019, with substantial data on persistent symptoms of COVID-19 having been accumulated.123456 The World Health Organization (WHO) defined persistent COVID symptoms that last for more than 12 weeks as a post-COVID-19 condition,17 while the Centers for Disease Control and Prevention defined a post-COVID-19 condition as COVID symptoms persisting for more than one month.8 Recently, after the omicron wave, COVID-19 symptoms have been less severe compared to those of the Delta or earlier variants; most patients had mild symptoms and were treated mainly as outpatients rather than needing to be hospitalized.91011 However, although COVID-19 symptoms have decreased in severity, they can persist for a long time. Therefore, determining the prognostic factors for development of post-COVID-19 condition in outpatients with mild symptoms is becoming increasingly important.
Thus far, several studies have investigated prognostic factors associated with either the post-COVID-19 condition or symptom duration in patients with mild symptoms who visited the outpatient department (OPD). The identified risk factors for persistent symptoms in outpatients with COVID-19 include being female, having obesity, having a psychiatric condition, having multiple comorbidities, and having received previous vaccination against COVID-19.12131415 However, these studies have only focused on demographic risk factors; variables such as biomarkers, chest image, and pulmonary function tests (PFTs) were not included. Therefore, this study aims to investigate various prognostic factors for symptom duration including laboratory data, chest X-rays, and PFT, among patients with persistent COVID-19 symptoms who visited the OPD after their mandatory isolation period of 7 days.
METHODS
Study design and population
This study is a single-center retrospective cohort study, with data analyzed from non-hospitalized patients with mild COVID-19 who visited the ‘post-COVID-19 outpatient clinic’ at Ewha Womans University Mokdong Hospital (a tertiary hospital in South Korea) after the obligatory one-week isolation period between April and December 2022. Patients who visited the post-COVID-19 clinic for reasons unrelated to COVID-19, including issuing certificates and routine follow-ups for underlying disease, were excluded. Patients without a recorded date of COVID-19 diagnosis were also excluded. COVID-19 diagnosis was confirmed by a polymerase chain reaction test or a rapid COVID-19 antigen test. All patients received conservative treatment for symptoms and underwent follow-up visits every few days to two weeks until their symptoms resolved. We defined the post-COVID-19 condition as the persistence of one or more symptoms for more than 12 weeks, according to the WHO definition.17
Data collection
Clinical and demographic data of the patients were collected retrospectively from their medical records. The date of COVID-19 diagnosis and symptom resolution were collected, with symptom duration defined as the time between the date of diagnosis and symptom resolution. Regarding the symptoms, we collected information from the medical records provided by physicians, as well as from the symptom checklist that patients filled out prior to the consultation, which included cough, sputum, and dyspnea (Supplementary Table 1). Laboratory tests and PFT results that were performed at the time of the first outpatient visit after the diagnosis of COVID-19 were collected. Spirometry and diffusing capacity were measured following European Respiratory Society/American Thoracic Society recommendations,1617 and the results were presented as a percentage of the normal predicted value. The laboratory tests included a complete blood count, blood chemistry, C-reactive protein, D-dimer, and 25(OH)D3 tests. The 25(OH)D3 level was measured by an electrochemiluminescence immunoassay (Liaison® 25(OH)D3 Total, DiaSorin, Saluggia, Italy), and a 25(OH)D3 level < 20 ng/mL was defined as a vitamin D deficiency according to the WHO definition.18 Chest X-rays and/or chest computed tomography (CT) scans performed at the time of the first visit in all patients were analyzed. If any abnormalities were detected on the chest X-ray, a chest CT scan was performed to further investigate the lesions. Consolidation or ground-glass opacities were considered as abnormal findings that could suggest COVID-19-induced pneumonia.
Statistical analysis
Continuous variables were presented as mean ± standard deviation and a t test was conducted for comparison of the variables. The χ2 test was used to compare categorical variables, with values denoted as numbers (%). The Kaplan-Meier curve and log-rank test were used to compare the duration of COVID-19 symptoms. Logistic regression analysis was used to investigate risk factors regarding the post-COVID-19 condition. The cut-off for the continuous variable used in the logistic regression analysis for prognostic factors was determined using the receiver operating characteristic curve. The prognostic factors for longer symptom duration were obtained using the time-to-event analysis (Cox regression analysis) and the event was defined as the resolution of symptoms. If patients were lost to follow-up, it was censored on the date of the last visit. The variables with hazard ratio > 1 refer to favorable factors for resolution of symptoms. Variables with a P value of < 0.1 in the unadjusted analysis were selected and adjusted by age, sex, respiratory comorbidities, and vaccination status for the multivariable analysis. A P value of < 0.05 denoted statistical significance. Statistical analyses were performed using IBM SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Ewha Womans University Mokdong Hospital (IRB No. 2022-09-010) and conducted in accordance with the ethical standards of the Declaration of Helsinki. The requirement for written informed consent was waived owing to the retrospective nature of this study.
RESULTS
Baseline characteristics
From April to December 2022, 325 patients visited the post-COVID-19 outpatient clinic, with data from 257 patients retrospectively analyzed, excluding the 68 patients who visited the clinic for reasons unrelated to COVID-19 (Fig. 1). The median symptom duration was 57 days (interquartile range [IQR], 35–96 days), and the median duration from the initial COVID-19 diagnosis to the first visit was 31 days (IQR, 17–61 days). The mean age of patients was 55.7 years, and the proportion of males was 42.8% (Table 1). Smokers accounted for 31.5%, and 24.1% of patients had obstructive lung disease including asthma, chronic obstructive pulmonary disease, and bronchiectasis. The proportion of patients who had never been vaccinated for COVID-19 was 8.9%, and the proportion of those vaccinated more than three times was 59.1%. A total of 21 patients (8.6%) received antiviral agents in the acute phase before their first visit, with all receiving nirmatrelvir/ritonavir. In 21 patients (8.6%), abnormal findings suggesting COVID-induced pneumonia were observed on their chest CT scans. The proportion of symptoms at the time of their first visit is shown in Supplementary Table 1. The patients with cough and sputum accounted for the largest proportion with 63.4% and 52.9%, respectively, followed by those with dyspnea, fatigue, and rhinorrhea.
Fig. 1
Flowchart of the study population.
OPD = outpatient department, COVID-19 = coronavirus disease 2019.
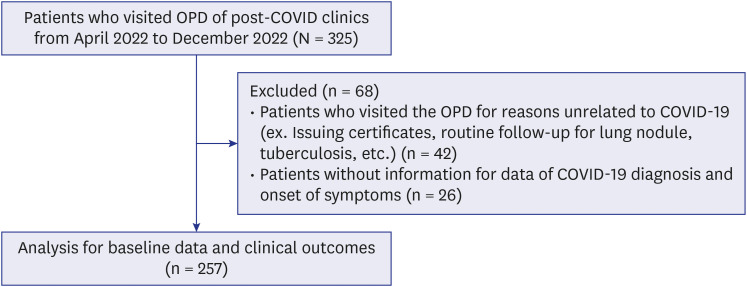
Table 1
Baseline characteristics of the study population at the time of their first visit to the outpatient department
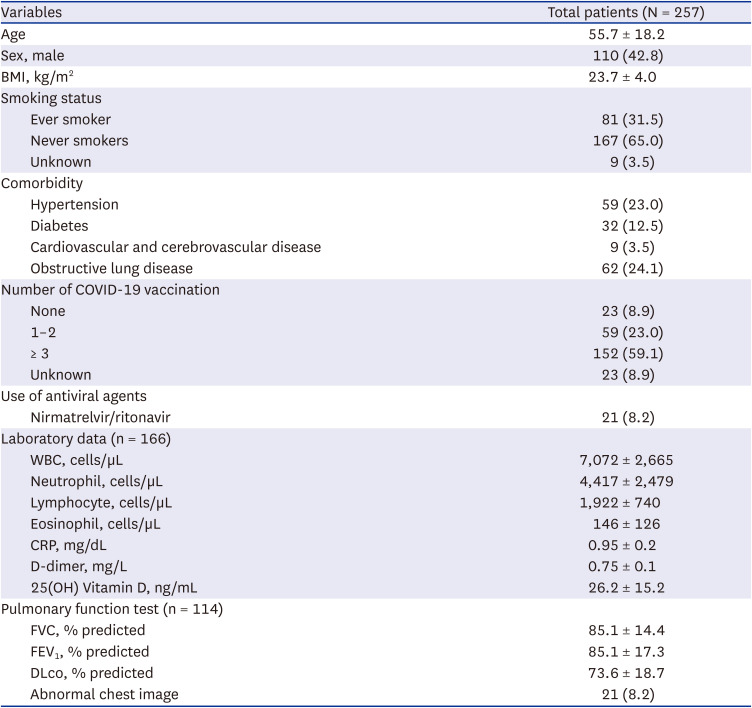
Data are presented as mean ± standard deviation or number (%).
BMI = body mass index, COVID-19 = coronavirus disease 2019, WBC = white blood cells, CRP = C-reactive protein, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, DLco = diffusing capacity of the lung for carbon monoxide.
Prognostic factors for the development of post-COVID-19 condition (> 12 weeks) and symptom duration
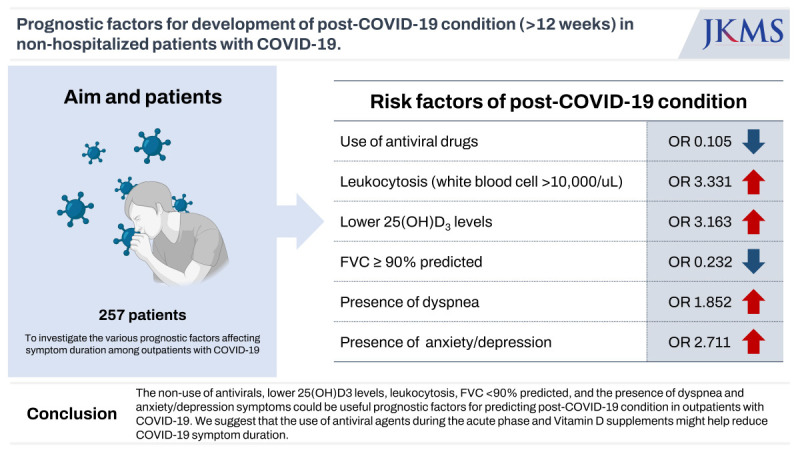
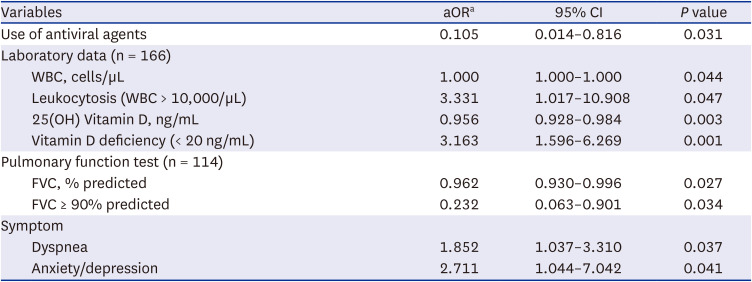
Among patients visiting the post-COVID-19 clinic, 77 patients (30.0%) met the criteria for post-COVID-19 condition, with symptoms persisting for more than 12 weeks. Not using nirmatrelvir/ritonavir during the acute phase, higher white blood cell (WBC) count, leukocytosis (WBC > 10,000/µL), lower 25(OH)D3 levels, lower forced vital capacity (FVC), FVC < 90% predicted, and having dyspnea and anxiety/depression were shown to be independent poor prognostic factors for post-COVID-19 condition in multivariable logistic analysis adjusted by age, sex, respiratory comorbidities, and vaccination status (Table 2 and Supplementary Table 2).
Table 2
Multivariable logistic regression analysis for development of post-COVID-19 condition (> 12 weeks) in non-hospitalized patients with COVID-19
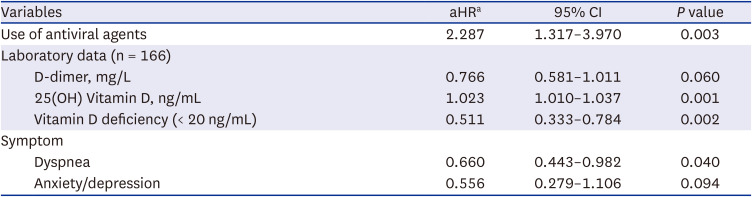
In multivariable Cox regression analysis adjusted by age, sex, respiratory comorbidities, and vaccination status, the poor prognostic factors for longer symptom duration included not using nirmatrelvir/ritonavir during the acute phase, lower 25(OH)D3 levels, and having dyspnea (Table 3 and Supplementary Table 3).
Table 3
Multivariable Cox regression analysis for symptom resolution in non-hospitalized patients with COVID-19
Clinical outcomes according to vitamin D deficiency and use of antiviral agents
We also analyzed the clinical outcomes regarding vitamin D deficiency and use of antivirals. Of the 166 patients whose 25(OH)D3 levels were collected, 67 (40.4%) had a vitamin D deficiency. When comparing the demographic characteristics between the two groups, the group with vitamin D deficiency at the first visit had higher proportion of patients with obstructive lung disease and unvaccinated patients than the group with no vitamin D deficiency (Supplementary Table 4). The baseline characteristics of the two groups based on the use of antiviral agents during the acute phase are presented in Supplementary Table 5. Those who received antiviral agents were older.
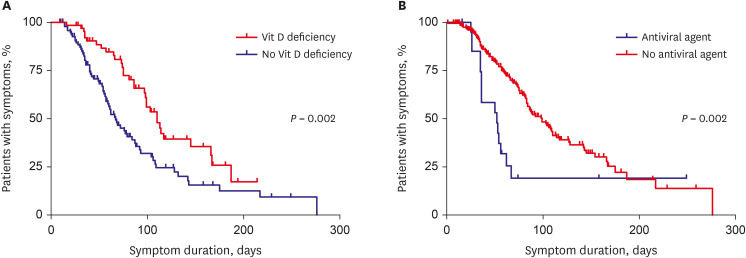
There were no significant differences in hospitalization rates or abnormal chest images at the first visit between the two groups based on vitamin D deficiency and use of antivirals. However, patients with vitamin D deficiency and no use of antivirals were significantly more likely to experience symptoms lasting more than 12 weeks (P = 0.001 and P = 0.033, respectively) (Tables 4 and 5). Additionally, the Kaplan-Meier curves demonstrated that patients with vitamin D deficiency (median, 110 vs. 67 days; P = 0.002) and those who did not receive antivirals (median, 99 vs. 52 days; P = 0.002) had longer symptom durations compared to those without these factors (Fig. 2).
Table 4
Clinical outcomes of patients with COVID-19 according to Vit D deficiency at the time of their first visit to OPD (N = 166)

Table 5
Clinical outcomes of patients with COVID-19 according to use of antiviral agent at acute phase of COVID-19

DISCUSSION
In this study, we found various prognostic factors including biomarkers and PFT for predicting symptom duration in patients with COVID-19 who visited the OPD after the isolation period. Not using antivirals during the acute phase, higher WBC count, leukocytosis (WBC > 10,000/µL), lower 25(OH)D3 levels, lower FVC, FVC < 90% of predicted value, and having dyspnea and anxiety/depression were associated with the development of post-COVID-19 conditions (symptoms > 12 weeks). Particularly, vitamin D deficiency and not using antivirals during the acute phase were independent poor prognostic factors for both post-COVID-19 condition and longer symptom duration.
To date, studies on post-COVID-19 conditions have focused on inpatients with moderate to severe symptoms, while only a few studies have focused on outpatients. Subramanian et al.12 reported that young age (18–29 years), being female, ethnic minority, socioeconomic deprivation, smoking, obesity, and a wide range of comorbidities were risk factors for long COVID (> 12 weeks) among non-hospitalized patients in a retrospective cohort study (n = 486,149). Augustin et al.13 conducted a multivariable logistic analysis on 958 patients with COVID-19 visiting the outpatient clinic and showed that being female, number of symptoms, and 1.1 < severe acute respiratory syndrome coronavirus 2 immunoglobulin G level at baseline ≤ 4.0 were predictors for developing post-COVID syndrome (> 4 months). Stavem et al.,14 in a study of 451 non-hospitalized patients with COVID-19, reported that the number of comorbidities and number of symptoms during the acute COVID-19 phase were poor prognostic factors predicting persistent symptoms (> 1.5 months). Tenforde et al.19 found that age (≥ 50), number of comorbidities (≥ 3), obesity, and psychiatric condition were associated with not having returned to usual health within three weeks after diagnosis after conducting a multivariable logistic analysis adjusted by age, sex and race in 270 patients with COVID-19 visiting the OPD. However, these studies included only demographic factors or clinical symptoms of patients; they did not include laboratory data, PFT, or chest imaging data. To our knowledge, this is the first study to investigate the association between symptom duration and factors including laboratory tests, PFTs, and chest imaging in an outpatient setting.
Interestingly, this study showed that lower 25(OH)D3 levels were associated with development of the post-COVID-19 condition and longer symptom duration. So far, several studies have investigated the relationship between vitamin D levels and the mortality or severity of COVID-19.20212223 It has been hypothesized that vitamin D can reduce the infectivity and severity of COVID-19 through several mechanisms including strengthening the physical barrier junction of the respiratory tract, activating cellular innate immunity such as human cathelicidin and LL-37, and reducing cytokine storm symptoms.24 A recent meta-analysis of 23 studies reported that vitamin D deficiency (25(OH)D3 < 20 ng/mL) was significantly associated with severity (risk ratio [RR], 2.00; 95% confidence interval [CI], 1.47–2.71; P<0.001) and mortality (RR, 2.45; 95% CI, 1.24–4.84; P < 0.001) of COVID-19.20 Dror et al.,21 in 253 hospitalized COVID-19 patients, also showed that patients with pre-infection vitamin D deficiency (< 20 ng/mL) had increased severity (P < 0.001).
However, unlike mortality or severity, the prognostic role of vitamin D level on symptom duration is uncertain. For example, Townsend et al.25 showed that persistent fatigue and reduced exercise tolerance at a median of 79 days after COVID-19 illness was not related to vitamin D levels in a study of 149 hospitalized and non-hospitalized patients. Pizzini et al.26 also found that symptoms persisting for more than eight weeks after the initial COVID-19 diagnosis were not associated with vitamin D deficiency in a study of 109 hospitalized or non-hospitalized patients. This is contrary to our findings that vitamin D deficiency is related to persistent symptoms. These previous studies were conducted during the Delta or earlier COVID waves,2526 and the proportion of systemic symptoms such as fatigue was greater than in this study (57% vs. 26%).25 By contrast, all patients in this study presented with the omicron variant, with the majority of patients complaining of respiratory symptoms, similar to a previous study conducted on omicron patients in Korea.27 Although the mechanism is unclear, we can hypothesize that vitamin D might reduce the neuroinflammation or neuro-immune modulation induced by cytokines in the respiratory tract, which can cause respiratory symptoms.282930
In addition to vitamin D, this study demonstrated that not using antivirals during the acute phase of COVID-19 was also associated with persistent symptoms. Previous studies has shown that antivirals can reduce mortality in critically ill patients with COVID-19.3132 Recent studies have also indicated that early administration of antivirals can prevent the progression to severe COVID-19 in outpatient settings.3334 Hammond et al.34 showed that the incidence of COVID-related hospitalization or death by day 28 in patients receiving nirmatrelvir plus ritonavir was lower than in the placebo group by 6.32 percentage points in a phase 2–3 randomized controlled trial (n = 2,246). Additionally, the viral load was also lower in antiviral agent treatment group than in placebo group.34 However, there is currently no study that has specifically investigated the association between the duration of symptoms and the use of antiviral agents. In our study, patients who received antivirals, specifically nirmatrelvir plus ritonavir, experienced shorter duration of symptoms. These results led us to hypothesize that the potential preventive effects of nirmatrelvir plus ritonavir in mitigating the severity of COVID-19 and reducing viral load34 could contribute to a decrease in symptom duration.
The presence of dyspnea as a symptom of COVID was also a risk factor for post-COVID-19 condition. Dyspnea is a common symptom of post-COVID-19 condition, with a prevalence ranging from 10% to 40%.33536 In a retrospective study by Sudre et al.,37 they reported that the presence of dyspnea during the first week of infection was identified as a risk factor for persistent symptoms lasting more than 28 days (n = 558, odds ratio [OR], 2.36; 95% CI, 1.91–2.91). Fernández-de-Las-Peñas et al.38 also found an association between the presence of dyspnea during the acute phase and a higher number of post-COVID symptoms in hospitalized patients (n = 1,969, OR, 1.20; 95% CI, 1.01–1.41). The mechanisms underlying association between dyspnea and post-COVID-19 condition are not yet fully understood. However, it is believed that a variety of comprehensive factors, including physical factors such as subclinical pulmonary embolism or post-COVID pulmonary fibrosis, as well as emotional components, may contribute to this relationship.394041 In a multicenter prospective cohort study by Daines et al.41 (n = 1,226), socioeconomic deprivation (OR, 1.67), pre-existing depression/anxiety (OR, 1.58), female sex (OR, 1.56), and admission duration (OR, 1.01) were identified as risk factors for post-COVID-19 dyspnea, regardless of pre-existing respiratory condition.
Meanwhile, contrary to previous studies showing that obesity (body mass index [BMI] ≥ 30.0 kg/m2) was a poor predictor for COVID-19 or the post-COVID-19 condition,4243 we could not establish a statistical association between BMI and the onset of post-COVID-19 condition or symptom duration. Rather, with an adjusted odds ratio of 0.989, it appeared that a lower BMI was associated with a higher occurrence of post-COVID-19 condition in this study. This may be because of the difference in the prevalence of obesity between the cohorts of previous studies and this current study (24–48% vs. 5.4%). One study in China, conducted on COVID-19 patients, 8.29% of whom were obese, showed that being underweight (BMI < 18.5 kg/m2) was a poor prognostic factor for secondary infection and acute lung injury.44
Moreover, previous studies have reported that various factors that were identified as poor prognostic factors for post-COVID-19 condition in our study— higher WBC count,454647 lower FVC,4849 and anxiety/depression symptoms5051—were related to poor outcomes of COVID-19 or the post-COVID-19 condition, supporting our findings.
There are some limitations to this study. First, this study was a single-center study conducted on exclusive Asian patients, making our findings difficult to extrapolate worldwide. Nevertheless, our study can suggest various risk factors for persistent symptoms, which could be the basis for conducting future large-scale studies. Second, because of the nature of conducting a retrospective study in an outpatient setting, there were some missing data including test results, and the exact time of symptom resolution was often unclear. However, when comparing the incidence of post-COVID-19 condition (symptoms lasting > 12 weeks) between those who did not have any laboratory tests or PFT (n = 65) and those who underwent at least one of these tests (n = 192), there was no significant difference (44.4% vs. 42.2%, P = 0.876). Moreover, as patients visited the clinic relatively frequently until their symptoms resolved, we were able to minimize potential errors regarding symptom duration. Additionally, despite dyspnea at the time of first visit being an unfavorable prognostic factor for the development of post-COVID-19 condition, the retrospective nature of our record analysis made it difficult to ascertain the objective severity of the symptoms. These issues should be investigated in future prospective studies. Third, our study cohort only comprised acute/subacute COVID-19 patients who visited the health care center after mandatory isolation, so we could not analyze risk factors in all COVID-19-infected patients, meaning that selection bias is possible. Nevertheless, we reduced potential bias by using multivariable analysis adjusted by demographic factors including respiratory comorbidities, and it is thought that this study reflected actual clinical practice during the omicron wave when symptoms are becoming progressively milder and only a few patients need to use healthcare service. Finally, this study only analyzed patients with the omicron variant. Since the characteristics of coronavirus continue to change, research on prognostic factors should be conducted on any future COVID-19 variants.
In conclusion, our study found that in patients with COVID-19 who visited the OPD after the mandatory isolation period the poor prognostic factors for post-COVID-19 condition were not using antiviral agents, lower 25(OH)D3 levels, leukocytosis (WBC > 10,000/µL), FVC < 90% of the predicted value, and having dyspnea and anxiety/depression symptoms. Vitamin D deficiency (< 20 ng/mL) and not using antivirals during the acute phase were particularly useful prognostic factors, predicting both the development of post-COVID-19 condition (> 12 weeks) and longer symptom duration. We suggest that the use of antiviral agents during the acute phase and vitamin D supplements might help reduce the duration of COVID-19 symptoms in outpatient settings.
 XML Download
XML Download