

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Renal cell carcinoma (RCC) accounts for 2–3% of all cancers. In 2020, approximately 431,288 new cases of RCC were diagnosed and 179,368 patients died of this disease.1
Over the past few decades, advances in diagnosis and treatment improved the survival rate of patients with RCC. Nevertheless, when recurrence or metastasis occurs in patients with localized RCC or locally advanced RCC, the 5-year survival rate decreases to less than 20–30%.23
Finding predictive factors associated with high recurrence rates in patients with localized RCC is very important. Identifying the patterns of patients at high risk for recurrence can allow us to timely administer further treatment to patients with recurrent RCC to delay or eliminate recurrence as much as possible. Additionally, patients with a low risk of recurrence can avoid the implement of unnecessary further treatment to prevent side effects. Previously, several clinical risk-prediction models have been identified for survival and risk of recurrence in patients RCC.456789 Nevertheless, predictive factors for early recurrence in patients with RCC have not yet been accurately identified, and previously mentioned predictors of recurrence of RCC are still controversial among studies.10
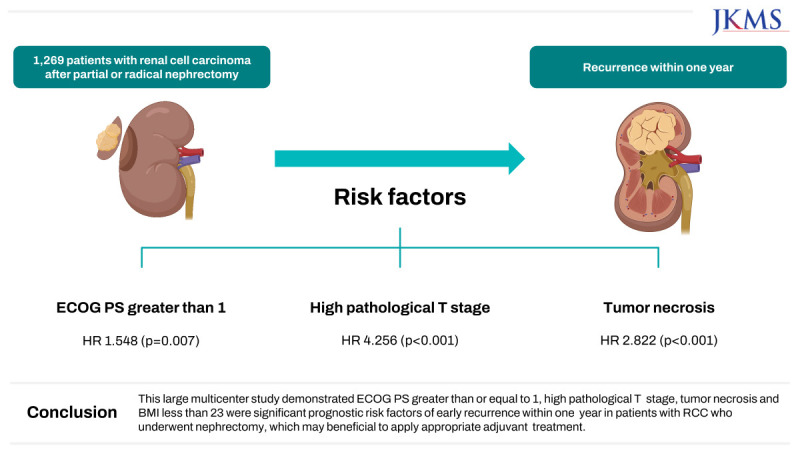
The purpose of this study was to identify prognostic risk factors of early recurrence within one year in patients with RCC after partial or radical nephrectomy for primary renal tumor. This has not been confirmed in studies to date and is expected to provide guidance on appropriate further treatment in patients with early recurrence of RCC.
METHODS
Patient population and data collection
Data of the 3,117 patients with RCC who diagnosed recurrence were obtained from Korean Renal Cancer Study Group (KRoCS) database from multiple Korean tertiary institutions. The RCC database included patients with RCC diagnosed with pT1-4NxM0 diagnosed with recurrence at eight tertiary hospitals in Korea (Seoul Saint Mary’s Hospital, Samsung Medical Center, Asan Medical Center, National Cancer Center, Korea University Medical Center, Chonnam National University Hwasun Hospital, Seoul National University Hospital and Seoul National University Bundang Hospital).
A total of 1,269 (40.7%) patients were selected for this study. All participants underwent partial or radical nephrectomy with or without lymphadenectomy between January 1991 and March 2017 and had a minimum follow-up period of 6 months until detection of local recurrence or distant metastasis. Exclusion criteria were age < 19 years (n = 6); without nephrectomy (n = 709); diagnosed metastasis before nephrectomy (n = 747); postoperative recurrence of RCC within 1–3 months to exclude obscured synchronous metastasis at the time of nephrectomy (n = 100); and insufficient medical records for at least 6 months, and history of previous cancers (n = 286).
The parameters analyzed in this study were baseline characteristics and laboratory information including comorbidities, age, gender, body mass index (BMI), Eastern Cooperative Oncology Group performance status (ECOG PS), hemoglobin, serum albumin, serum creatinine, modification of diet in renal disease (MDRD) study equation for estimation of glomerular filtration rate (eGFR) and pathology results including pTNM stage, histology, Fuhrman nuclear grade, sarcomatoid differentiation, lymphovascular invasion, tumor necrosis and capsule invasion.
The surgical procedures of partial nephrectomy and radical nephrectomy have been documented in previous published papers and because the data were collected retrospectively from a multicenter database, information regarding standardized protocols for surgical procedures was not included in the RCC database.11121314 Further, imaging intervals during the initial postoperative imaging follow-up period, i.e., 1- or 3-month intervals, were not standardized and based on the urologists' preference in relation to the postoperative surveillance protocol established at the time.
Statistical analysis
Continuous variables were analyzed with the t-test or Mann–Whitney U test, and categorical variables were analyzed with the Fisher’s exact test or Pearson’s χ2 test.
Recurrence-free survival (RFS), and overall survival (OS) were calculated using the Kaplan–Meier method, and statistical significance was tested by the log-rank test. Univariate and multivariate Cox regression analysis were performed to evaluate independent prognostic factors for recurrence and described as the hazard ratio (HR) and 95% confidence interval (CI). A two-sided P value < 0.05 was considered statistically significant. Statistical analysis was performed with IBM® SPSS® Statistics 27.
Ethics statement
Approval for this retrospective study using of KRoCS database was obtained from the Institutional Review Board of Dongtan Sacred Heart Hospital, Hallym University College of Medicine (approval number: 2021-10-006-002). A written informed patient consent was waived by the Institutional Review Board due to the retrospective nature of study. All study protocols were conducted in accordance with the ethical guidelines and regulations of the “World Medical Association Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects.”
RESULTS
Of the 1,227 patients, 971 (76.5%) were men and median patient age was 56 years (IQR 49-64) and median follow-up period was 67 months [interquartile range (IQR) 30-123].
There were 494 (38.9%) patients with BMI < 23, 719 (56.7%) patients with 23 ≤ BMI < 30 and 56 (4.4%) patients with BMI ≥ 30. The number of smoking patients was 420 (33.1%). Patients with DM and HTN were 242 (19.1%) and 541 (42.6%), respectively. The number of patients with CKD, CVA, and heart disease was 53 (4.2%), 25 (2.0%) and 33 (2.6%), respectively. Mean serum creatinine [± standard deviation (SD)] was 1.44 ± 1.24 and mean MDRD study equation for eGFR (± SD) was 59.01±19.26. ECOG PS was 0 for 926 patients (73.0%) and ≥ 1 for 343 patients (27.0). The operation technique was radical nephrectomy in 1182 patients (93.1%) and partial nephrectomy in 87 patients (6.9%). Pathological T stage distribution was 584 patients (46.0%) for pT1, 241 patients (19.0%) for pT2, 423 patients (33.3%) for pT3, and 21 patients (1.7%) for pT4. Tumor necrosis and sarcomatoid components were observed in 18.9% and 6.2%, respectively. Overall, histology distribution was 1,015 clear cell carcinoma (80.0%), 86 papillary cell carcinoma (6.8%) 30 chromophobe cell carcinoma (2.4%) and others 138 (10.9%) (Table 1).
Table 1
Patient demographics and clinicopathological factors
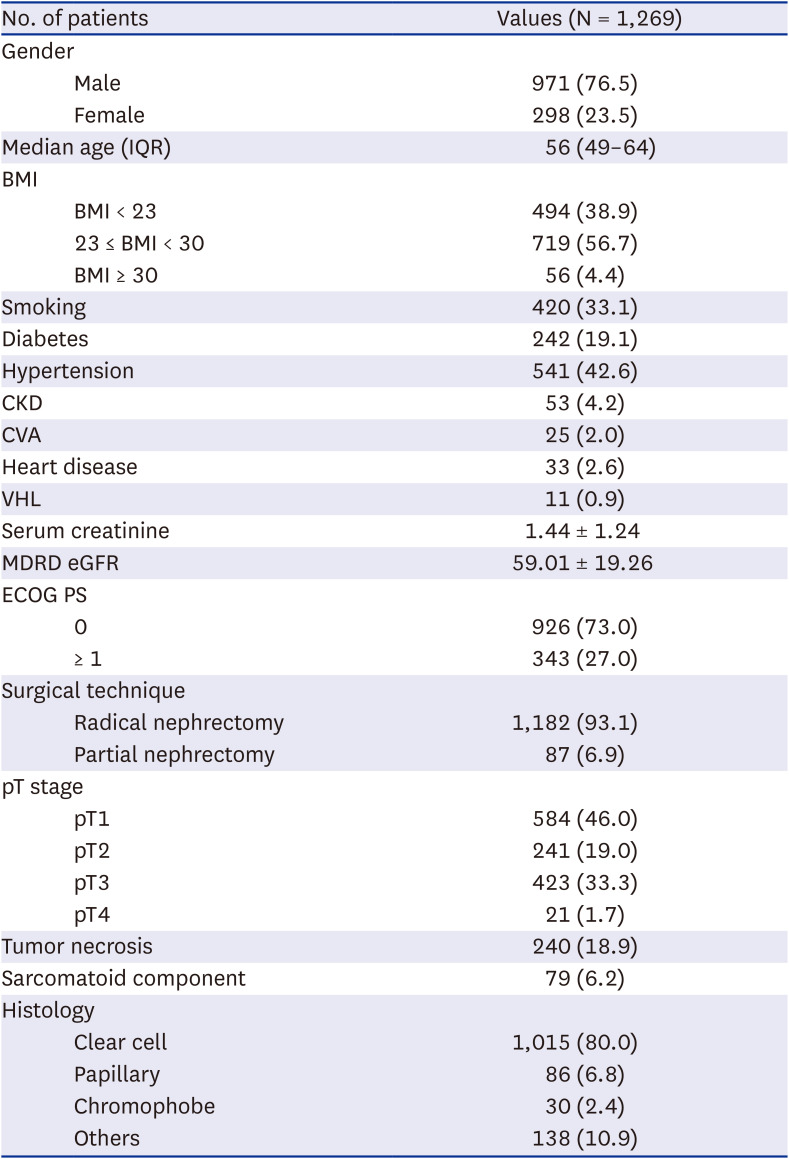
Values are presented as number (%) or mean ± standard deviation unless otherwise indicated.
IQR = interquartile range, BMI = body mass index, CKD = chronic kidney disease, CVA = cerebrovascular accident, VHL = von Hippel-Lindau, MDRD eGFR = modification of diet in renal disease study equation for estimation of glomerular filtration rate, ECOG PS = Eastern Cooperative Oncology Group performance status, pT = pathologic T.
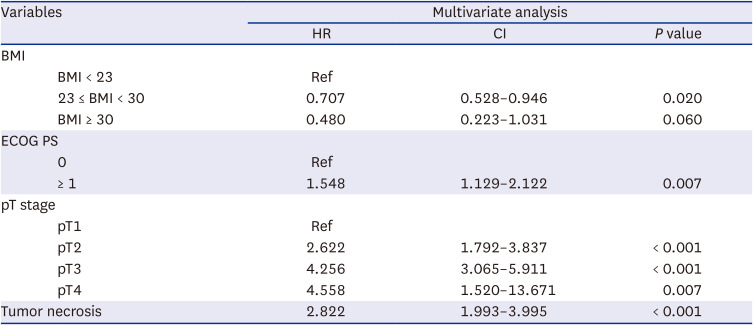
Results of univariate analysis of predictors of one year recurrence in patients with RCC after nephrectomy are shown in Table 2. Age, BMI, smoking, MDRD eGFR, ECOG PS, partial nephrectomy, other histology, pathological T stage and were significant predictive factors for one year recurrence of RCC. Moreover, multivariate analysis demonstrated that BMI greater than or equal to 23 and less than 30 [versus (vs.) BMI less than 23, hazard ratio (HR): 0.707, P = 0.020] reduced recurrence one year after surgery. ECOG PS greater than or equal to 1 (vs. ECOG PS 0, HR: 1.548, P = 0.007), high pathological T stage (pT2 vs. pT1, HR: 2.622, P < 0.001; pT3 vs. pT1, HR: 4.256, P < 0.001; pT4 vs. pT1, HR: 4.558, P < 0.001), and tumor necrosis (vs. no tumor necrosis, HR: 2.822, P < 0.001) were independent predictive factors for early recurrence within one year in patients with RCC (Table 3).
Table 2
Univariate analysis of prognostic risk factors of early recurrence of renal cell carcinoma within 1 year
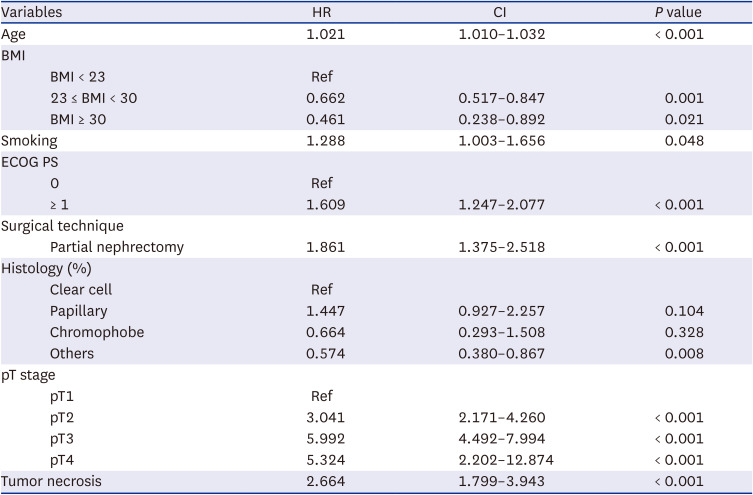
Table 3
Multivariate analysis of prognostic risk factors of early recurrence of renal cell carcinoma within 1 year
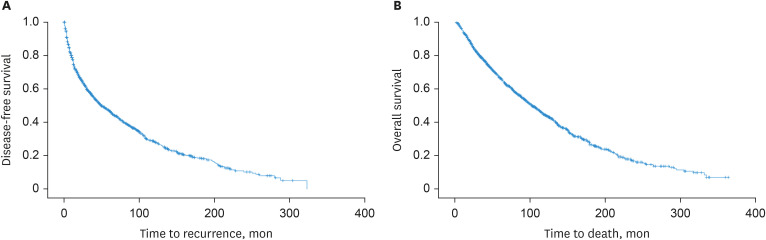
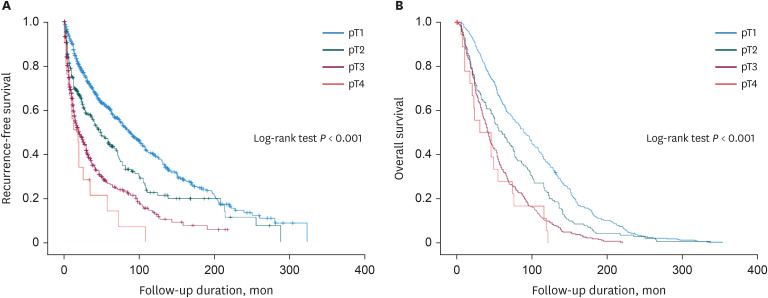
Furthermore, median time to recurrence was 44 months (IQR 8-67) and the number of recurrences within one year was 438 (34.5%) (Fig. 1). We analyzed differences in survival rates between pathological T stages. Statistically significant differences on RFS and OS were found among pathological T stages (pT2 vs. pT1; pT3 vs. pT1; pT4 vs. pT1, all P < 0.001) (Fig. 2).
DISCUSSION
Identifying the prognostic risk factors for early recurrence in patients with RCC after nephrectomy is closely related to the proper treatment of metastatic RCC, which has heterogeneous and polymorphic pathophysiology and for which diverse treatments have emerged as treatment guidelines change every year. For this reason, several large retrospective studies have been conducted to define patterns and predictors of recurrence after nephrectomy on localized RCC patients.456151617 However, no study has reported prognostic risk factors related to recurrence within one year in localized RCC patients. Current study included 1,269 post-nephrectomy localized RCC patients to find one year recurrence predictive factors which provide assistance in enrolling appropriate further treatment in patients at high risk of early metastasis.
Several clinical models have been developed to predict patient outcome using localized RCC models to assess recurrence risk. Zisman A et al reported a prospective cohort study using data from 1989 to 2000 that provided the University of California Los Angeles Unified Staging System (UISS) model to predict outcome in patients with RCC who underwent nephrectomy. As predictive factors to estimate postoperative 5-year OS, tumor-node-metastasis staging, tumor grade, and ECOG PS were included.4 Later, UISS model was generally applied as a predictor of survival for patients with localized RCC.5 Sorbellini et al.16 reported prognostic factors of Memorial Sloan-Kettering Cancer Center to predict the 5-year recurrence in post nephrectomy patients with clear cell RCC (ccRCC) consist of pathologic stage, Fuhrman grade, tumor size, necrosis, vascular invasion, and clinical presentation. Frank et al.17 announced cancer specific survival (CSS) outcome prediction model for ccRCC patients treated with radical nephrectomy between 1970 and 1998 using TNM stage, tumor size, nuclear grade and histological tumor necrosis. Leibovich et al.6 developed the predictive factors for metastasis specific survival for ccRCC patients underwent radical nephrectomy between 1970 and 2000 including tumor stage, regional lymph node status, tumor size, nuclear grade, and histologic tumor necrosis. The VEnous extension, NUclear grade, Size, Stage (VENUSS) prognostic model was developed and validated to predict the recurrence of papillary RCC patients who underwent curative surgery between 2000 and 2016.78 GRade, Age, Nodes and Tumor (GRANT) score were developed to predict outcome in RCC and applied to the Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ASSURE) trial population.9
Most of clinical models mentioned above included data from patients who underwent nephrectomy in the 1980s and 1990s and our study has the strength of using data from 1991 to 2017. In addition, current study supported the previous models which pathological stage, tumor necrosis and ECOG PS were found to be predictors of one year recurrence. These results are attributed to previously published clinical models and further introduce prognostic risk factors of early recurrence within one year after nephrectomy in patients with localized RCC. Furthermore, ECOG PS was only supported by UISS model as predictive factors previously and our study supported ECOG PS could be one of the predictors of recurrence. Therefore, the use of one year recurrence predictive factors is expected to benefit patient survival by allowing more appropriate use of further treatment for metastatic RCC patients than previously identified recurrence factors within 3 to 5 years.
Interestingly, the relation of BMI and survival of patients with RCC has been supported by multiple studies.181920 Choi et al.21 reported preoperative BMI is an independent prognostic indicator for OS, CSS, RFS in patients with RCC. Representatively, Sanchez et al.22 reported obesity paradox which obese patients with ccRCC had survival advantage because of clinical relevance of the ccRCC tumor and peritumoral adipose tissue microenvironment. Our study supported these previous studies which BMI as a prognostically beneficial to patients with RCC who underwent nephrectomy. Our result described patients with BMI greater than or equal to 23 and less than 30 had less recurrence than whom with BMI less than 23. Though there was no significant difference when compared to patients with BMI of 30 or more. In addition to the results of previous studies, our study suggested improved nutritional status might improve tumor resistance and reduce recurrence rates to localized RCC patients. These results may contribute to appropriate BMI to improve patient survival in patients with RCC who underwent nephrectomy, however further biological studies are needed to elucidate.
Current study has several limitations. First, this study used retrospective and multicenter data, which may lead to selection bias in the absence of a standardized surgical protocol and review of central pathology data. Second, the purpose of this study was to find one year recurrence risk factors, but the period to find the correlation with OS was not sufficient. Nevertheless, this study has the implications of the first large-scale multicenter study that presents prognostic risk factors for one year recurrence in RCC patients.
Early recurrence in patients with RCC may lead to worse prognosis and oncological outcomes. This large multicenter study demonstrated ECOG PS greater than or equal to 1, high pathological T stage, tumor necrosis and BMI less than 23 were significant prognostic risk factors of early recurrence within one year in patients with RCC who underwent nephrectomy, which may suggest the need for careful monitoring and further appropriate treatment.
 XML Download
XML Download