

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Idiopathic pulmonary fibrosis (IPF) is characterized by the progressive accumulation of fibroblasts in the pulmonary parenchyma and interstitium, which causes irreversible fibrosis and the deterioration of lung function.12 Recurrent alveolar epithelial cell injury leading to dysregulated epithelial cell signal influences mesenchymal, immune, and endothelial cells, thereby activating fibroblasts and myofibroblasts.3 Additionally, innate immune mechanisms and various inflammatory cells (e.g., immune cells, macrophages, T cells, and innate lymphoid cells) have been implicated in IPF pathogenesis.3 Although neutrophils are not commonly observed in the lung tissue of IPF, they release profibrotic cytokines and cause extracellular matrix remodeling.45 Neutrophil elastase levels as well as neutrophil-derived matrix-degrading enzymes (e.g., matrix metalloproteinases) are elevated in patients with IPF. They are the primary tissue-destructive agents that drive fibroblast proliferation and myofibroblast differentiation.67 Furthermore, cytokeratin 19, an alveolar epithelial injury marker, is correlated with neutrophil infiltration in IPF.8 A recent study has revealed elevated levels of granulocyte-colony stimulating factor in bronchoalveolar lavage fluid (BALF) from IPF patients, which were associated with lower survival rates.910 Additionally, BALF neutrophilia is associated with early mortality in IPF patients.1112 However, the mechanism underlying the relationship between neutrophils and IPF remains unclear.
The mediator S100 calcium-binding protein A9 (S100A9) is a damage-associated molecular pattern protein released by neutrophils and macrophages under conditions of cellular stress.13 This mediator causes fibroblast proliferation; it upregulates collagen type III and α-smooth muscle actin (α-SMA) through expression of the receptor for advanced glycation end-products (RAGE).1415 Previous studies have demonstrated higher S100A9 levels in BALFs from IPF patients than in those from patients with other interstitial lung diseases (ILDs), such as sarcoidosis, non-specific interstitial pneumonia (NSIP), or pulmonary fibrosis associated with connective tissue diseases.1617 However, the previous studies had small sample sizes (< 50 patients) and provided insufficient information regarding clinical outcomes. Here, we measured BALF and serum S100A9 levels in a relatively large cohort of IPF patients to determine the association between S100A9 levels and IPF. Additionally, we investigated the association between S100A9 levels and long-term survival rates.
METHODS
Study subjects
All subjects were examined by physicians and underwent a chest X-ray, high-resolution chest computed tomography (HRCT), and pulmonary function tests including forced vital capacity (FVC) and diffusion capacity of lungs for carbon monoxide (DLco). BALFs from study subjects, including healthy controls (HCs), as well as patients with IPF, NSIP, hypersensitivity pneumonitis (HP), and sarcoidosis, and serums from study subjects, including HCs and IPF patients, were obtained from the biobank of Soonchunhyang University Hospital, Bucheon, Korea (Schbc-biobank-18101601-14-01 and schbc-biobank-2021-010-01). Bronchoscopy was performed after obtaining the informed consent for the procedure within the first 2 weeks of the initial examination. Regarding the status of the sampling, the ILD subjects donated their samples in a stable state, and none had any signs of infection and acute exacerbation at the initial examination. Remnant bronchoalveolar lavage (BAL) samples after diagnostic laboratory study have been kept for storage in the Biobank and donated to scientists after permission of local Institutional Review Board (IRB) in each institution. The samples for HCs were obtained from the medical students and hospital personnel, after approval by the hospital Ethics Committee (IRB No: SCHBC 2015-08-025-005). Regarding lung tissues, the IPF lung tissues were obtained for diagnosis using video assisted thoracoscopy surgery, and the control lung tissues were obtained from cancer free - normal lungs of pathologic specimens from patients who underwent surgery for stage I or II lung cancer. IPF was diagnosed by the presence of usual interstitial pneumonia patterns in the pathological specimens (surgical IPF) and/or after multidisciplinary discussion without lung biopsy (clinical IPF) on the basis of the 2011 and 2018 guidelines.1819 There was no evidence of any underlying collagen vascular diseases in IPF patients according to their laboratory results and clinical symptoms. The diagnostic criteria for NSIP, HP, and sarcoidosis were based on international consensus statements.202122 HCs exhibited no respiratory symptoms as determined by a screening questionnaire and had a predicted forced expiratory volume at 1 second (FEV1) and FVC > 80.0% and normal chest radiograms.
Enzyme-linked immunosorbent assay (ELISA) of S100A9 in BALF and serum
BAL was performed in lung segments with the greatest disease involvement on HRCT in cases of ILD, or in the right middle lobe of the controls, as described previously.23 The total cell count was measured using a hemocytometer. Cells were removed from the supernatant by centrifugation (500 g, 5 minutes), and supernatants were stored at –80°C. Differential cell counts were performed on 500 BALF cells placed on slides prepared using a cytocentrifuge and Diff-Quik stain. S100A9 protein level was measured using an ELISA kit (MyBioSource, San Diego, CA, USA) according to the manufacturer’s recommendations. The lower limit of detection was 0.1 ng/mL, and values below this limit were set to 0. The inter- and intra-assay coefficients of variation were below 15.0%.
Immunofluorescence stain of S100A9 in bronchial alveolar lavage fluid cells and lung tissues
Paraffin blocks of IPF and control lung tissues were cut into 4-μm-thick slices, deparaffinized, and rehydrated. The lung tissue and BALF cell slides were fixed with 0.4% cold paraformaldehyde for 30 minutes at room temperature. The sections were incubated for 1 hour in an Fc receptor blocking agent (FC blocker, Innovex Biosciences, Richmond, CA, USA) containing 5.0% bovine serum albumin to block non-specific binding. The sections were then incubated overnight at 4°C with monoclonal mouse anti-human S100A9 antibody (1:200 dilution; Novus Biological, Littleton, CA, USA) and polyclonal mouse anti-human α-SMA antibody (1:200 dilution; Abcam, Cambridge, MA, USA). Slides of BALF cells were incubated overnight with monoclonal goat anti-human CD163 antibody for macrophages (1:200 dilution, Hycult Biotech, Uden, PB, Netherlands) and monoclonal rabbit anti-human neutrophil elastase antibody (1:100 dilution; Abcam) for neutrophils. After washing three times with tris buffered saline (TBS), the slides were incubated for 1 hour at room temperature with the following fluorescent secondary antibodies: anti-rabbit IgG H&L (FITC) (1:1,000 dilution; Abcam), anti-mouse IgG H&L (PE) (1:1,000 dilution; Abcam), or anti-goat IgG H&L (PE) (1:1,000 dilution; Abcam). After washing in TBS, the slides were incubated for 3 minutes at room temperature with 4′,6-diamidino-2-phenylindole (DAPI) (Sigma-Aldrich, St. Louis, MO, USA) and confocal laser scanning was performed using a microscope (LSM 510 META, Zeiss, Jena, Germany) coupled to a CoolsnapPhotometrics HQ camera (Photometrics, Tucson, AZ, USA), and images were generated using the Zeiss LS M image browser.
Statistical analysis
The Kruskal–Wallis test and the post-hoc Mann–Whitney U test were used to compare the S100A9 levels between groups. Correlations between the S100A9 levels and other parameters were analyzed using Spearman’s correlation coefficient. The data are presented as median with 25.0% and 75.0% quartile for variables with a skewed distribution, or as a mean ± standard error of the mean for variables with a normal distribution. Receiver operating characteristic (ROC) analysis was performed, and the area under the ROC curve (AUC) and cutoff values were determined using MedCalc statistical software. Optimal cutoff levels of S100A9 and the neutrophil percentage were calculated using Cutoff Finder.24 Survival rates were estimated using the Kaplan–Meier method and compared using a log-rank test. The data were analyzed using SPSS software v. 20.0 (IBM Corp., Armonk, NY, USA). Values of P < 0.05 were considered statistically significant.
RESULTS
Demographic characteristics
In the present study, 127 IPF, 22 NSIP, 19 HP, 10 sarcoidosis patients, and 77 HCs were enrolled. Among them, we obtained BALF from patients with IPF (n = 87), NSIP (n = 22), HP (n = 19), and sarcoidosis (n = 10). Among IPF patients, 62 had undergone surgical lung biopsy before diagnosis, whereas 65 were diagnosed without lung biopsy. Additionally, BALF was obtained from 33 HCs. Serum was obtained from 90 patients with IPF and 40 normal controls. Among them, BALF and serum were matched in 50 patients with IPF, but not in the normal controls. Table 1 presents the clinical characteristics of the study patients, who underwent BAL procedure. The total cell count, comprising macrophages, neutrophils, lymphocytes, and eosinophils, was significantly higher in BALF from patients with IPF, NSIP, HP, and sarcoidosis than in BALF from HCs (P < 0.05). Moreover, all patients exhibited lower FVC and FEV1, compared with HCs (P < 0.05). Serum samples were collected from 90 IPF patients and 40 HCs. Clinical characteristics of the participants are summarized in Supplementary Table 1. The IPF patients had significantly lower values of FVC and FEV1 than the HCs (P < 0.05). Among them, BALF was concomitantly obtained from 50 of the IPF patients.
Table 1
Clinical characteristics of study participants who underwent bronchoalveolar lavage
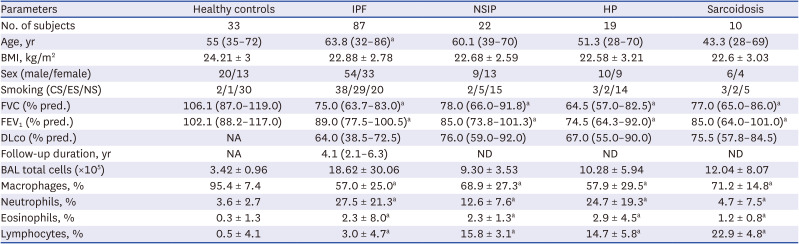
Data are presented as medians (inter-quartile range) or mean ± standard error of the mean. Groups among the normal controls and the IPF, NSIP, HP, and sarcoidosis patients were compared using a Kruskal–Wallis ANOVA with the Mann–Whitney U as the post-hoc test, or using a one-way ANOVA and Tukey’s honestly significant difference test as the post-hoc test among the five groups. Significance: compared with control, aP < 0.05.
IPF = idiopathic pulmonary fibrosis, NSIP = non-specific interstitial fibrosis, HP = hypersensitivity pneumonitis, BMI = body mass index, CS/ES/NS = current smoker/ex-smoker/never smoker, FVC = forced vital capacity, FEV1 = forced expiratory volume at 1 second, DLco = diffusing capacity of the lungs for carbon monoxide, BAL = bronchoalveolar lavage, ANOVA = analysis of variance.
Comparison of S100A9 levels in BALF of IPF with those of other ILDs and HCs
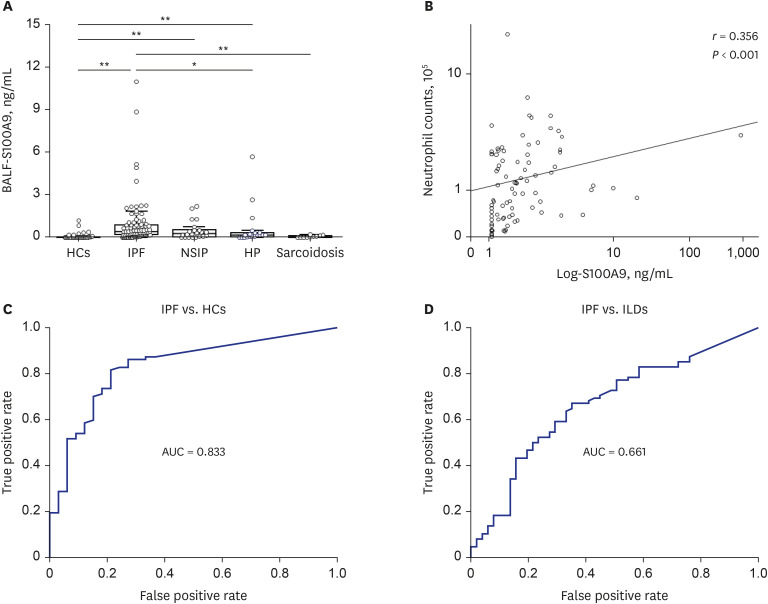
Compared with S100A9 levels (0 [0–0.5] ng/mL) in BALF from HCs, significantly higher S100A9 levels in BALF were observed in BALF from patients with IPF (0.4 [0.18–0.9] ng/mL, P < 0.001), NSIP (0.28 [0.07–0.52] ng/mL, P < 0.001), and HP (0.19 [0.07–0.33] ng/mL, P < 0.001). Moreover, S100A9 levels in BALF were significantly higher among IPF patients than among patients with HP (P = 0.043) or sarcoidosis (0.06 [0–0.11] ng/mL, P < 0.001). S100A9 levels in BALF were significantly correlated with neutrophil counts in BALF from IPF patients (n = 87, r = 0.356, P < 0.001) (Fig. 1B and Supplementary Table 2). The ROC curve showed a clear distinction between IPF patients and HCs (AUC = 0.833, Fig. 1C). The S100A9 in BALF cutoff level of 0.093 ng/mL, as determined by the ROC curve, had a specificity of 78.8% and a sensitivity of 81.6% for distinguishing IPF patients from HCs. Furthermore, the S100A9 in BALF cutoff level of 0.239 ng/mL exhibited a specificity of 64.7% and a sensitivity of 66.7% for distinguishing IPF patients from those with the other ILDs including NSIP, HP, and sarcoidosis (AUC = 0.661, Fig. 1D).
Fig. 1
S100A9 levels, correlation with neutrophil percentage in BALF, and ROC analysis. (A) S100A9 levels were detected in 12 of 33 HCs, 76 of 87 patients with IPF, 17 of 22 patients with NSIP, 15 of 19 patients with HP, and 6 of 10 patients with sarcoidosis. Data are presented as medians with interquartile ranges. (B) Correlation between S100A9 levels and neutrophil percentages in BALF (n = 87, r = 0.356, P = 0.007). (C) ROC curves for S100A9 levels in IPF patients and HCs. A cutoff value of 0.093 ng/mL had an AUC of 0.833, specificity of 78.8%, and sensitivity of 81.6% for distinguishing IPF patients from HCs. (D) A cutoff level of 0.239 ng/mL for S100A9 exhibited a specificity of 64.7% and a sensitivity of 66.7% for distinguishing between IPF patients and patients with other ILDs (AUC = 0.661).
BALF = bronchoalveolar lavage fluid, S100A9 = S100 calcium-binding protein A9, HC = healthy control, IPF = idiopathic pulmonary fibrosis, NSIP = non-specific interstitial fibrosis, HP = hypersensitivity pneumonitis, AUC = area under the ROC curve, ILD = interstitial lung disease, ROC = receiver operating characteristic.
*P < 0.05; **P < 0.001.
Associations of survival rates and clinical features with BALF S100A9 level and neutrophil count in IPF patients
In total, 84 IPF patients were followed up for 1–10 years. The cutoff values for S100A9 level in BALF and neutrophil percentage were determined as previously described in the methods section. The survival rate was significantly lower in patients with S100A9 levels in BALF > 0.553 ng/mL (n = 35) than in patients with S100A9 levels in BALF ≤ 0.553 ng/mL (n = 49; hazard ratio [HR], 3.62; 95.0% confidence interval [CI], 1.13–11.63; P = 0.021, Fig. 2A). In the IPF patients with S100A9 levels > 0.553 ng/mL, the total cell and neutrophil counts in BALF were significantly higher than the counts in those with S100A9 levels in BALF ≤ 0.553 ng/mL (P < 0.001, Supplementary Table 3). Similarly, the survival rate was significantly lower in patients with neutrophil percentages > 49.1% (n = 17) than in patients with neutrophil percentages ≤ 49.1% (n = 67; HR, 5.38; 95.0% CI, 2.07–13.98; P = 0.003, Fig. 2B). Moreover, patients with S100A9 levels in BALF > 0.553 ng/mL or neutrophil percentages > 49.1% (n = 43) had significantly lower survival rates, compared with patients who had S100A9 levels in BALF ≤ 0.553 ng/mL and neutrophil percentages ≤ 49.1% (n = 41; HR, 3.91; 95.0% CI, 1.62–9.39; P = 0.014, Fig. 2C). The patients with S100A9 levels in BALF ≤ 0.553 ng/mL and neutrophil percentages ≤ 49.1% had higher proportion of men (P = 0.02, Table 2) than those with S100A9 levels in BALF > 0.553 ng/mL or neutrophil percentages > 49.1%. However, the two groups displayed no significant differences in age, body mass index, smoking status, or lung function.
Fig. 2
Survival rates in relation to S100A9 levels and neutrophil percentages in bronchoalveolar lavage fluid from IPF patients. Kaplan–Meier analysis was used to analyze 84 IPF patients who were followed up for 1–10 years. (A) Comparison of survival rates between patients with S100A9 levels > 0.553 ng/mL (n = 35, dotted line) and patients with S100A9 levels ≤ 0.553 ng/mL (n = 49, solid line) (HR, 3.62; 95.0% CI, 1.13–11.63; P = 0.021). (B) Comparison of survival rates between patients with neutrophil percentages > 49.1% (n = 17, dotted line) and patients with neutrophil percentages ≤ 49.1% (n = 67, solid line) (HR, 5.38; 95.0% CI, 2.07–13.98; P = 0.003). (C) Comparison of survival rates between patients with S100A9 levels > 0.553 ng/mL or neutrophil percentages > 49.1% (n = 43, dotted line) and patients with S100A9 levels ≤ 0.553 ng/mL and neutrophil percentages ≤ 49.1% (n = 41, solid line) (HR, 3.91; 95.0% CI, 1.62–9.39; P = 0.014).
S100A9 = S100 calcium-binding protein A9, Neu = neutrophil, IPF = idiopathic pulmonary fibrosis, HR = hazard ratio, CI = confidence interval.
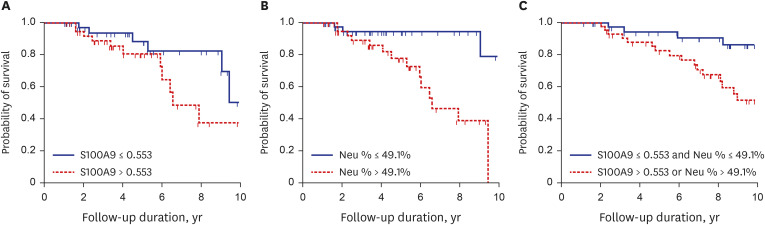
Table 2
Clinical characteristics of patients with idiopathic pulmonary fibrosis classified according to the levels of S100A9 and percentage of neutrophils in bronchoalveolar lavage fluid

Data are presented as medians (inter-quartile range) or mean ± standard error of the mean. Between group differences were compared using the Mann–Whitney U as the post-hoc test, or using Student’s t-test.
S100A9 = S100 calcium-binding protein A9, BMI = body mass index, CS/ES/NS = current smoker/ex-smoker/never smoker, FVC = forced vital capacity, FEV1 = forced expiratory volume at 1 second, DLco = diffusing capacity of the lungs for carbon monoxide, BAL = bronchoalveolar lavage.
Significance: compared with control, *P < 0.05.
Associations of survival rates and clinical features with serum S100A9 levels in IPF patients
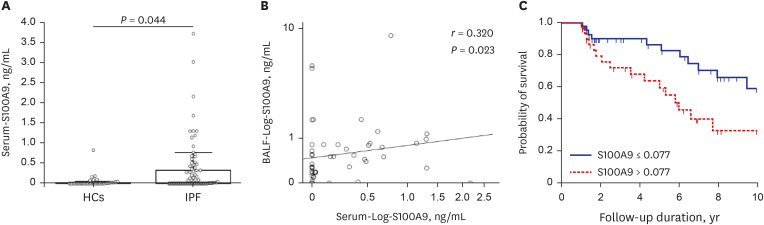
Significantly higher S100A9 levels in serum were observed in IPF patients (0.01 [0–0.32] ng/mL) than in HCs (0 [0–0.02] ng/mL, P = 0.044, Fig. 3A). A significant association was detected between S100A9 levels in serum and S100A9 levels in BALF from 50 IPF patients (P = 0.023, Fig. 3B). Kaplan–Meier survival analysis of 82 patients who were followed up for 1–10 years revealed a significantly lower survival rate among patients with S100A9 levels in serum > 0.077 ng/mL (n = 29) than among patients with S100A9 levels in serum ≤ 0.077 ng/mL (n = 53; HR, 2.52; 95.0% CI, 1.15–5.51; P = 0.013, Fig. 3C).
Fig. 3
S100A9 levels in serum from IPF patients and relationship with survival rates. (A) Serum S100A9 levels were detected in 19 pf 40 HCs and in 53 of 90 IPF patients. Data are expressed as medians with 25.0% and 75.0% quartiles, with statistical significance denoted as *P < 0.05 vs. HCs. (B) Correlation between S100A9 levels in serum and BALF (r = 0.320, P = 0.023). (C) Kaplan–Meier survival curves comparing survival rates between IPF patients with S100A9 levels > 0.077 ng/mL (n = 29, dotted line) and those with S100A9 levels ≤ 0.077 (n = 53, solid line) ng/mL (hazard ratio, 2.52; 95.0% confidence interval, 1.15–5.51; P = 0.013).
S100A9 = S100 calcium-binding protein A9, IPF = idiopathic pulmonary fibrosis, HC = healthy control, BALF = bronchoalveolar lavage fluid.
S100A9 immunofluorescence staining of lung tissues and BALF cells from IPF patients
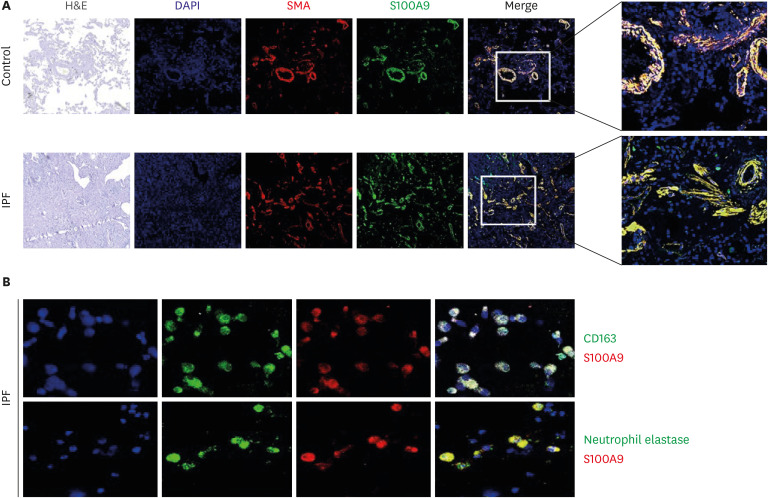
To confirm S100A9 expression in IPF patients, we performed double immunofluorescence staining of S100A9/α-SMA using lung tissues from 3 IPF patients and 3 controls. In lung tissues from controls, α-SMA and S100A9 staining was detected in perivascular and peribronchial areas. In lung tissues from IPF patients, interstitial fibroblasts expressed α-SMA; most of these fibroblasts also expressed S100A9 (Fig. 4A). To confirm S100A9 expression in BALF cells from IPF patients, we performed double immunofluorescence staining of S100A9 with CD163 and neutrophil elastase. Macrophages strongly expressed CD163; most of these cells also exhibited S100A9 expression (Fig. 4B). Moreover, we observed co-staining of neutrophil elastase and S100A9 in BALF cells from IPF patients.
Fig. 4
Immunofluorescence staining of S100A9 in lung tissues and BALF cells of IPF patients. (A) S100A9 (green) and α-SMA (red) were co-stained with PE-(red) or FITC-conjugated antibodies (green), respectively (200× magnification). (B) Images show colocalization of pan-macrophage marker CD163 (Alexa 488) (green) and S100A9 (Alexa 594) (red), along with DAPI-stained nuclei (blue) (400× magnification). Control: lung tissue obtained from normal lungs of the patients who underwent surgery for stage I or II lung cancer.
BALF = bronchoalveolar lavage fluid, IPF = idiopathic pulmonary fibrosis, S100A9 = S100 calcium-binding protein A9, SMA = smooth muscle actin, PE = phycoerythrin, FITC = fluorescein isothiocyanate, DAPI = 4′,6-diamidino-2-phenylindole, H&E = hematoxylin & eosin.
DISCUSSION
This study demonstrated that BALF S100A9 levels were significantly higher in IPF patients than in HCs and patients with other ILDs. High S100A9 levels in BALF had high sensitivity and specificity for diagnosis and differentiation of IPF from HCs as well as other ILDs. Moreover, a cutoff value of 0.553 ng/mL for S100A9 could separate IPF patients into short-term and long-term survival groups, with an HR of 3.62. Based on these findings, S100A9 levels in BALF could serve as a useful surrogate biomarker for prediction of survival in IPF patients.
In the past decade, multiple studies have revealed higher S100A9 levels in BALF from IPF patients, compared with patients who have other ILDs.16172526 The levels were inversely related to impairments in lung function, as indicated by reduced FVC and DLco.17 Moreover, S100A9 levels could distinguish IPF from NSIP and collagen vascular disease-related interstitial pneumonia.25 However, these reports were based on relatively small numbers of patients. Recently, Bennett et al.27 reported that higher S100A9 levels have been associated with more advanced IPF, lower lung function values, shorter walking distance in the 6-min walk test, and BALF neutrophilia in 30 IPF patients. Our study findings are consistent with the results of previous investigations. In addition, we have confirmed the utility of serum S100A9 levels as a biomarker for predicting survival rates in larger cohorts of IPF patients. To our knowledge, this is the first study to demonstrate the utility of serum S100A9 as a surrogate biomarker for predicting prognosis in patients who cannot provide BALF samples because of the invasive procedure involved.
S100A9 is a small calcium-binding protein released by cells undergoing necrosis in response to stress.13 S100A9 can exacerbate non-infectious inflammation by enhancing chemotaxis among neutrophils and macrophages, and by modulating the functions of these cells.2829 Considering the prevalence of neutrophilic inflammation in BALF from IPF patients,1130 S100A9 is suspected to participate in the pathogenesis of neutrophilic inflammation in IPF. Consistent with this hypothesis, we found a significant association between S100A9 levels in BALF and neutrophil percentages in BALF from IPF patients. In addition, when the S100A9 levels were adjusted with the neutrophil count in BALF, there were significant differences in the values of S100A9 between groups. The ratio of S100A9 to the number of neutrophils was higher in IPF, NSIP, and HP compared to HCs (Supplementary Table 4). Thus, neutrophils may have a greater potency to produce S100A9 in IPF compared to those in HCs. Furthermore, a cutoff value of 49.1% for neutrophil percentage in BALF samples could separate patients into short- and long-term survival groups, with an HR of 5.38. A combined analysis of S100A9 levels and neutrophil percentages showed that patients with S100A9 levels in BALF > 0.553 ng/mL or neutrophil percentages > 49.1% had a significantly lower survival rate, compared with patients who had S100A9 levels in BLAF ≤ 0.553 and neutrophil percentages ≤ 49.1%, with an HR of 3.91. These findings indicate that the combined effect of high S100A9 levels or high neutrophil percentages leads to a significantly higher mortality risk among IPF patients, compared with the effect of high S100A9 levels alone.
S100A9 and neutrophils are involved in the pathogenesis of inflammatory conditions, such as severe asthma and chronic obstructive pulmonary disease.31323334 In addition to its pro-inflammatory effects, S100A9 has fibrotic effects.33 S100A9 stimulates fibroblast proliferation and myofibroblast differentiation by inducing the expression of cellular communication network factor 2, promoting basal migratory motility in fibrocytes, and activating lung fibroblasts through the RAGE signaling pathway and activation of ERK1/2 MAPK and nuclear factor-κB.31535 In the present study, immunofluorescence revealed co-expression of S100A9 and the markers of macrophages and neutrophils, indicating the major sources of S100A9 from macrophages and neutrophils. Regarding co-localization of S100A9 on α-SMA in fibrotic loci, fibroblasts may uptake the S100A9 derived from macrophages and neutrophils when considering the expression of S100A9 is minimal on fibroblasts determined using single-cell next-generation sequencing.36 As S100A9 receptors, RAGE and Toll-like receptor 4 levels are also elevated in parenchymal fibroblasts and infiltrating cells within fibrotic loci.3738 Therefore, high S100A9 levels may induce neutrophil and monocyte inflammation, as well as fibroblast activation, leading to fibrosis progression.
Our study has several limitations. First, we did not measure other mediators released by neutrophils, such as neutrophil elastase and matrix metalloproteinases. The IPF-patients having low S100A9 levels with high neutrophil percentages were also associated with early mortality, suggesting that other neutrophil-derived mediators may contribute to the mortality implicated in IPF patients: neutrophil elastase is a potential candidate because it degrades various ECM components and promotes fibroblast proliferation and myofibroblast differentiation in a SMAD-dependent, but transforming growth factor (TGF)-β-independent, manner.67 An additional mediator is the neutrophil extracellular trap, which promotes fibrosis by inducing TGF-β1 production and subsequent myofibroblast activation.39 Therefore, future studies should evaluate the effects of these mediators on prognosis of IPF patients. Second, there was a small number of patients with other ILDs, including NSIP, and HP to evaluate the diagnostic significance. Finally, validation studies using other cohorts are required to improve the diagnostic utility of S100A9.
To investigate the role of S100A9 in neutrophilic inflammation associated with IPF, we measured S100A9 levels in BALF and serum. Our findings revealed significantly higher S100A9 levels in IPF patients than in HCs or patients with other ILDs. Moreover, S100A9 levels could distinguish IPF from other ILDs as well as HCs. IPF patients with increased S100A9 levels or neutrophil percentages demonstrated significantly lower survival rates, compared with patients who had reduced S100A9 levels and neutrophil percentages. These findings suggest that S100A9 plays a role in the development and progression of IPF; moreover, S100A9 levels in BALF and serum could serve as a surrogate biomarker for diagnosis and survival in patients with IPF, particularly when combined with neutrophil percentages.
 XML Download
XML Download