

 PDF
PDF Citation
Citation Print
Print



A 76-year-old woman was admitted to our clinic with exertional chest pain for 2 weeks.
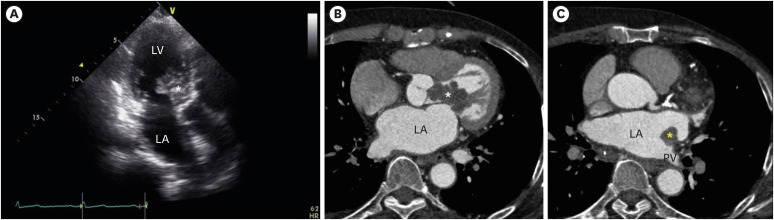
Transthoracic echocardiography revealed a multi-lobulated hypoechoic mass occupying the left ventricular (LV) outflow tract with dynamic systolic protrusion into the aortic root (Fig. 1A; Supplementary Videos 1 and 2). The about 4 cm sized mass was attached to the anterior leaflet of the mitral valve on the LV side. The mass occupied the LV outflow tract, leading to an increased mean pressure gradient of 42 mmHg. Owing to the mass effect, the anterior leaflet of the mitral valve partially closed during diastole, leading to an obstruction of the mitral inflow with a mean pressure gradient of 5 mmHg.
Cardiac computed tomography (CT) showed that the LV mass exhibited enhancement on early post-contrast image (Fig. 1B). An additional small mass, measuring 1.5 cm, was observed on the left atrial wall at the opening of the pulmonary vein (Fig. 1C).
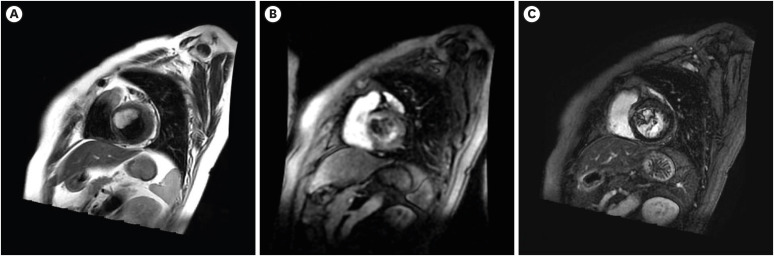
Cardiac magnetic resonance imaging revealed high signal intensity of the masses on T2-weighted imaging (Fig. 2A). During dynamic post-contrast examination, the LV mass showed heterogenous enhancement (Fig. 2B). During the delayed phase, the LV mass showed late gadolinium enhancement (Fig. 2C).
With positron emission tomography CT, other primary malignancies were excluded. The maximum standardized uptake value of the mass was 3.7.
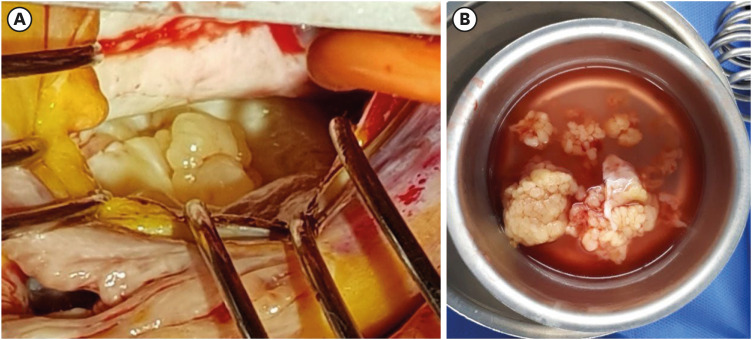
Based on multimodal imaging, the mass was suspected to be primary cardiac sarcoma. The patient underwent surgery for removal of all the cardiac masses (Fig. 3A and B). Histopathologic examination revealed all the cardiac masses as cardiac sarcoma with marked myxoid change. Immunohistochemical staining was positive for CD34, myogenic differentiation 1 and transducer-like enhancer of split 1. Due to extensive myxoid change, the subtype of cardiac sarcoma could not be specified.

 XML Download
XML Download