

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Sequential Organ Failure Assessment (SOFA) score was created in 1994 at a Consensus Conference of the Working Group of the European Society of Intensive Care Medicine.1 The primary objective of the SOFA score was to describe objectively and grade organ dysfunction of the six essential organ systems—respiratory, coagulation, hepatic, cardiovascular (CV), renal, and central nervous system function.23 It was originally designed to be easy to use with a minimal number of variables and to assess the change in the degree of organ failure. Now it is one of the most widely used scoring systems in clinical practice and in research on adult critical care.3456789
In 2016, the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) proposed clinical criteria using the SOFA score as a main measurement of organ dysfunction reflecting the sepsis definition of a life-threatening organ dysfunction caused by a dysregulated host response to infection.10 Since then, the SOFA score has been adopted as a means of identifying sepsis among patients with suspected infection with the criteria of an acute change in total SOFA score of two points or more consequent to the infection; the metric was derived by mortality-based analyses in multiple large cohorts.7 Regarding septic shock, a lactate criterion of > 2 mmol/L despite adequate volume resuscitation was introduced to reflect circulatory dysfunction and cellular metabolic abnormality with persisting hypotension requiring vasopressors to maintain mean arterial pressure (MAP) ≥ 65 mmHg.11
Despite the widespread use and advantages of the SOFA score, there is a need to update the SOFA score to reflect the current practice particularly in sepsis because management strategies have evolved since the SOFA score was developed.2 Among the components of the SOFA, the CV SOFA has a critical limitation.12 The Surviving Sepsis Campaign (SSC) guidelines currently recommend using norepinephrine as the first-line vasopressor instead of dopamine and have done so since 2008, and other vasopressors including vasopressin and epinephrine have been commonly used as second-line vasopressors.13 Therefore, recent studies showed that there were few cases with CV SOFA score of 2 depending on the use of dopamine or dobutamine and the mortality rate of each CV SOFA score did not show incremental tendency.6912141516 In addition, considering the diagnostic importance of lactate level in sepsis patients and the current septic shock definition, lactate criteria can be incorporated but has not been fully evaluated.213171819
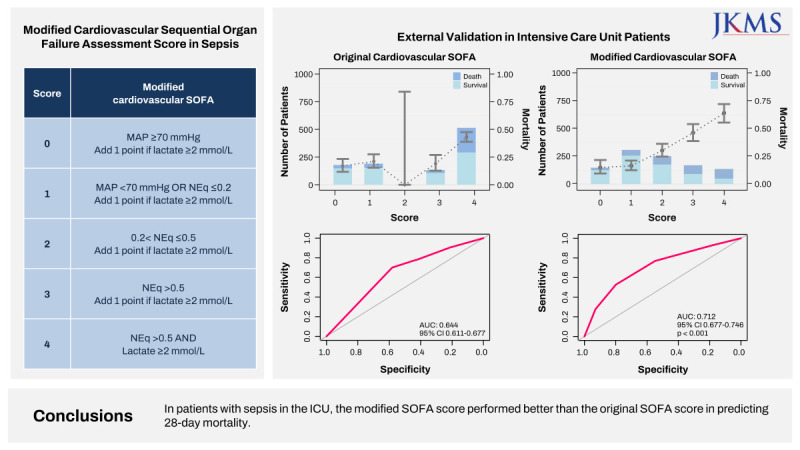
With this background, we proposed the modified CV SOFA score using MAP, norepinephrine equivalent (NEq) dose (Supplementary Table 1), and lactate in the previous multi-center, emergency department (ED) based study using suspected infection, sepsis, and septic shock cohorts.20 We found that the modified CV/total SOFA score had better discrimination for 28-day mortality than the SOFA score and identified more patients at risk of septic mortality. In the present study, we externally validated the modified CV SOFA score in multi-center intensive care unit (ICU) patients with sepsis.
METHODS
Study design, setting, and population
This was a multi-center, retrospective, observational study of ICU patients from six hospitals in Korea. We included adult patients (age ≥ 18 years) with sepsis who were admitted to medical or surgical ICUs. Sepsis cases were defined as cases with suspected infection and an acute change in total SOFA score of two points or more according to the sepsis-3 definition.10 The study period varied by location and occurred over the range of years from 2015 to 2021.
Data collection and outcome
The data were retrospectively collected by board-certified emergency medicine physicians or trained research coordinators of participating hospitals. We extracted data from the hospitals’ clinical data warehouses and reviewed the electronic medical record. We collected general patient characteristics, including age, gender, comorbidities, vital signs, infection focus on final diagnosis, laboratory tests, therapeutic interventions including vasopressor, mechanical ventilation use and renal replacement therapy, and survival data from the hospital database. The SOFA score was calculated as described in the previous study using the worst value obtained during the 24 hours after ICU admission.20 If variables were missing, including lactate and SOFA components, we imputed a normal value. The primary outcome was 28-day mortality after ICU admission. The secondary outcomes were in-hospital mortality and ICU mortality.
Modified cardiovascular SOFA score
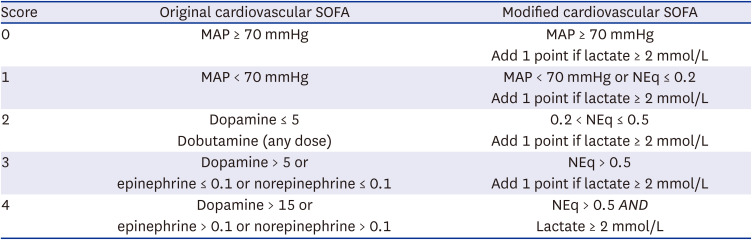
The modified CV SOFA scores in our previous study and the original CV SOFA scores are shown in Table 1. The modified CV SOFA score was developed and validated by testing multiple candidate models combining hypotension (MAP < 70 mmHg), dose of vasopressor, and lactate levels in the ED cohorts of suspected infection, sepsis, and septic shock (Supplementary Table 2). We used a NEq dose converted from each dose of vasopressor (dopamine, epinephrine, and vasopressin) and peak equivalent doses administered for at least one hour during the 24-hour period from ICU admission.3 In cases with MAP < 70 mmHg or use of low NEq dose (< 0.2 µg/kg/min), the modified CV SOFA score is 1 point, corresponding to MAP < 70 mmHg in the original CV SOFA. Modified cut-offs (0.2 and 0.5 µg/kg/min) of vasopressor dose were incorporated from score 1 to 4. If the serum lactate level is above 2 mmol/L in cases of CV SOFA score of 0 to 3 points, one point is added to the modified CV SOFA.
Table 1
Original and modified cardiovascular SOFA scores
Statistics
Continuous data are presented as mean (standard deviation, SD) or median (interquartile range, IQR) values, as appropriate. Categorical data are presented as numbers with percentages. For comparison, continuous variables were analyzed using Student’s t-test, while categorical variables were analyzed using χ2 tests. We compared predictive accuracy with the area under the receiver operating characteristic curves (AUROCs) of the original CV/total SOFA and the modified CV/total SOFA score using a non-parametric approach. We evaluated calibration plots of predicted and observed probability. Predicted mortality in calibration and 95% confidence interval (CI) were estimated by the bootstrap method.
We performed sensitivity analysis using a dataset with the last observation carried forward (LOCF) imputation and a complete data set without missing values. If there are missing values by the LOCF method, we imputed each mean value of 28-day survivors and non-survivors. A two-tailed P value < 0.05 was considered statistically significant. All analyses were performed using the R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria) and STATA version 17.0 (STATA Corporation, College Station, TX, USA).
Ethics statement
This study was approved by the Institutional Review Boards (IRB) of the six hospitals (Seoul Metropolitan Government–Seoul National University Boramae Medical Center [No. 30-2021-139], Asan Medical Center [No.2022-0203], Gangnam Severance Hospital [No. 3-2021-0506], Hanyang University Medical Center [No. 2022-01-019], Anyang Sam Hospital [No. 2022007], and CHA Bundang Medical Center [No.2022-07-070]). Informed consent was waived or obtained depending on cohort or hospital requirements.
RESULTS
Study population and characteristics of cohorts
We analyzed 1,015 ICU patients with sepsis. In overall patients, the 28-day mortality was 31.2% (n = 317) (Supplementary Fig. 1, Table 2). The mean age was 70.9 years, and the number of males was 582 (57.3%). Among included patients, 832 (82.0%) patients were admitted to the medical ICU and 208 (65.6%) patients were admitted to the ICU through the ED. The proportion of a lung source of infection in non-survivors was significantly higher than in survivors (47.6% vs. 40.3%, P = 0.028). The mean levels of lactate among survivors and non-survivors were 2.8 and 5.8 mmol/L (P < 0.001), respectively. The mean value of the SOFA score of the non-survivors was significantly higher than that of the survivors (11.0 vs. 7.7, P < 0.001). Other baseline characteristics of the study population are summarized in Table 2. The characteristics of the patients from the six hospitals participating in the study are described in Supplementary Table 3. The 28-day mortality rate by hospital varied from 23.5% to 59.4% (Hospital D). Number of cases used in analysis and missing values are outlined in Supplementary Table 4.
Table 2
Baseline characteristics
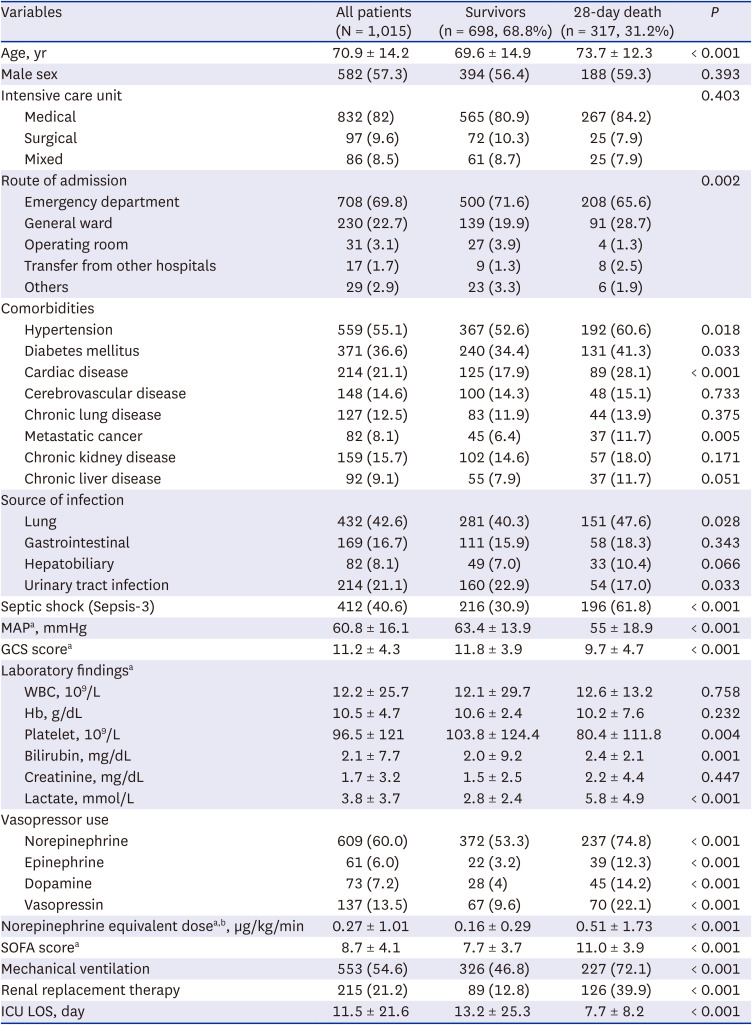
Values are presented as mean ± standard deviation or number (%).
MAP = mean arterial pressure, GCS = Glasgow Coma Scale, WBC = white blood cell, Hb = hemoglobin, SOFA = Sequential Organ Failure Assessment, ICU = intensive care unit, LOS = length of stay.
aThe worst value and intervention on the first day of intensive care unit admission were extracted.
bNorepinephrine equivalent doses are given as µg/kg/min at least 1 hour.
Incidence and 28-day mortality of original vs. modified CV SOFA score
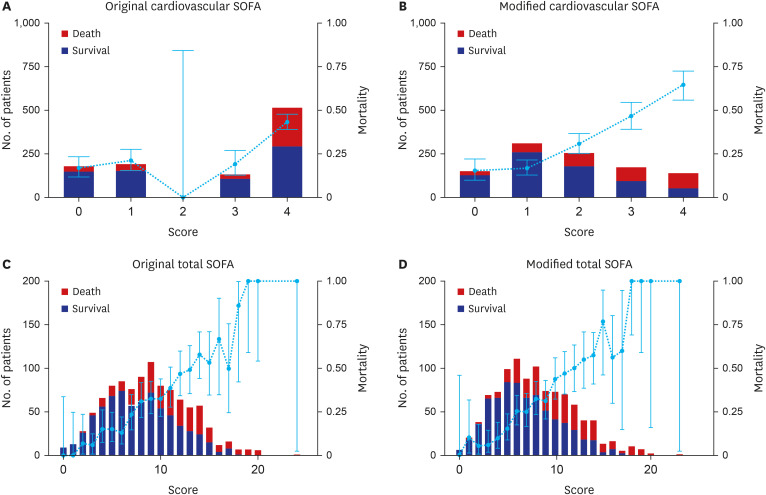
We analyzed the 28-day mortality of the original CV SOFA score and modified CV SOFA score (Fig. 1, Supplementary Table 5). There were only 2 patients with an original CV SOFA score of 2, and the 28-day mortality of patients with a CV SOFA score of 2 was lower than that of patients with an original CV SOFA score of 0 or 1 (16.9%, 21.5%, and 0.0% respectively in 0, 1, and 2 original CV SOFA score). The 28-day mortality increased as the modified CV SOFA score increased (15.0%, 16.6%, and 30.4% respectively in 0, 1, and 2 modified CV SOFA score). The incidence and 28-day mortality of the original total SOFA score and modified total SOFA score were shown in Fig. 1. The 28-day mortality tended to increase as either the original total SOFA score or the modified total SOFA score increased.
The discrimination and calibration of original vs. modified CV SOFA score
The AUROC of the original CV SOFA for predicting 28-day mortality was 0.644 (95% CI, 0.611–0.677; Fig. 2). The AUROC of the modified CV SOFA (AUROC, 0.712; 95% CI, 0.677–0.746; P < 0.001) was significantly higher than that of the original CV SOFA.
Fig. 2
Receiver operating characteristic curves for predicting 28-day mortality in the original and modified cardiovascular/total SOFA.
SOFA = Sequential Organ Failure Assessment, AUC = area under the curve, CI = confidence interval.
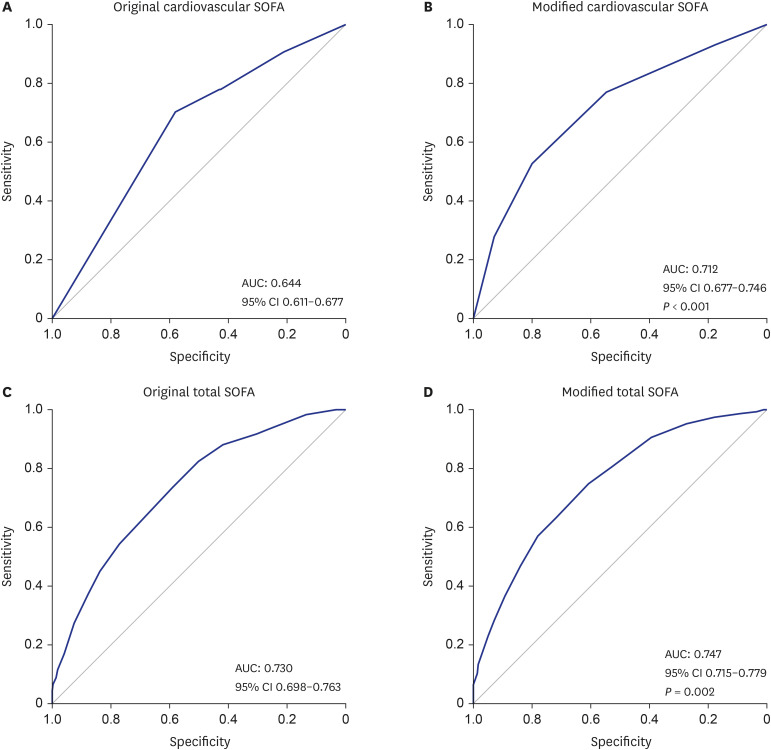
The predictive validity of modified total SOFA score for 28-day mortality was significantly higher than that of the original total SOFA (AUROC, 0.747 vs. 0.730; 95% CI, 0.715–0.779; P = 0.002) (Fig. 2).
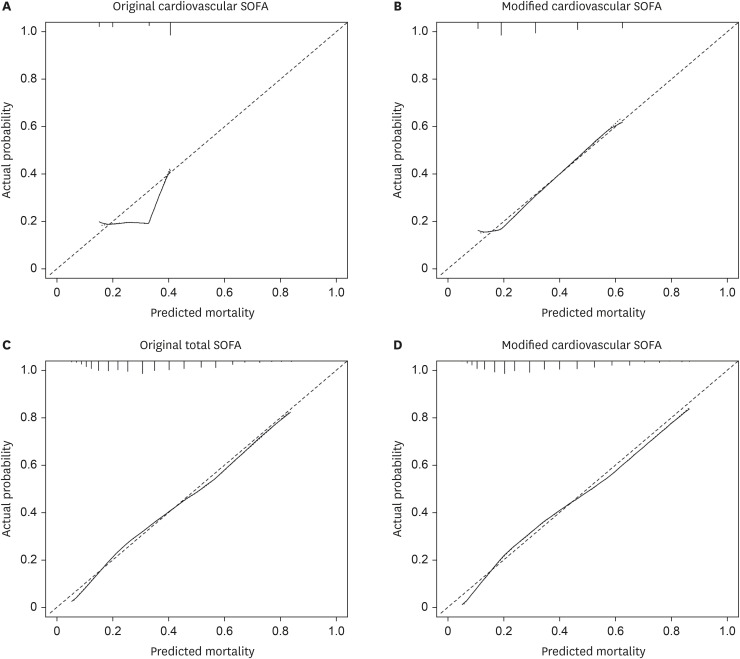
Calibration was evaluated with calibration plots of predicted and observed probability. The calibration curve of the original CV SOFA for 28-day mortality showed poor calibration (Fig. 3). In contrast, the calibration curve of the modified CV SOFA for 28-day mortality showed good calibration. The calibration curve of the original total SOFA and modified total SOFA for 28-day mortality showed good calibration.
Fig. 3
Calibration plots for 28-day mortality between the original and modified cardiovascular/total SOFA.
SOFA = Sequential Organ Failure Assessment.
AUROC for predicting 28-day mortality of the original CV/total SOFA and all candidate models are presented in Supplementary Table 6. Calibration plots for 28-day mortality of the candidate CV/total SOFA models are presented in Supplementary Fig. 2. AUROC for predicting in-hospital mortality in the original and modified CV SOFA were 0.643 and 0.702, respectively (P < 0.001) (Supplementary Table 7). AUROC of modified total SOFA was significantly higher than that of the original total SOFA (0.748 vs. 0.731; P = 0.002). AUROC for predicting ICU mortality of modified total CV/original total SOFA were also significantly higher than that of the original CV/total SOFA.
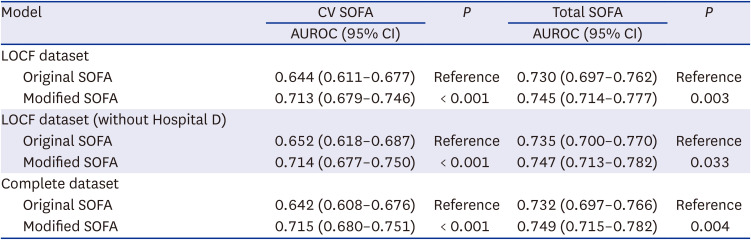
In the LOCF dataset, the AUROC of the modified CV SOFA (AUROC, 0.713; 95% CI, 0.679–0.746; P < 0.001) and the modified total SOFA score (AUROC, 0.745; 95% CI, 0.714–0.777; P = 0.003) for predicting 28-day mortality was significantly higher than that of the original SOFA (Table 3). AUROC of modified CV/total SOFA using the LOCF dataset without Hospital D which had the highest mortality and the complete data set were also higher than that of the original CV/total SOFA. Further results of the sensitivity analyses for in-hospital and ICU mortality are shown in Supplementary Table 8.
Table 3
Sensitivity analysis of AUROC for predicting 28-day mortality in the original and modified CV/total SOFA
DISCUSSION
In the previous study, we demonstrated that newly developed modified CV/total SOFA score had higher predictive validity and calibration in ED patients with suspected infection, sepsis, and septic shock.20 In this study, the same concept was applied to ICU patients, and the prognostic performance of modified CV/total SOFA score is better than that of the original scoring system, consistent with previous study.
When developing and validating a scoring system, the generalizability issue is important. To make accommodation for this issue, we used a multi-institution/mixed type ICU cohort. The baseline characteristics such as age, gender, shock status, the dose of vasopressor used, SOFA score, and mortality rate were different in the different participating ICUs. We proved the better performance of modified SOFA scoring system in sepsis under these various cases, which is the merit of this study. As in previous ED study, we also used multiple and various cohorts for the external validation, implying the modest generalizability of this modified SOFA score. However, a more extensive study to include multiple nationalities and more varied ICU type/ward/ED data should be performed to update the SOFA score.
The SOFA score has been widely used since it was developed by Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine in 1996.1 The SOFA score was adopted as sepsis definition in Sepsis-3 definition.10 However, it needs updating since the clinical practice has changed with the times. Recently, multinational groups started to develop the SOFA 2.0 score, which would definitely be helpful for the management of sepsis patients.2 We think our findings might be referenced with SOFA 2.0.
In this study, patients with an original CV SOFA score of 2 were rare, and the 28-day mortality rate among them was lower than among patients with original CV SOFA scores of 0 and 1. These findings support the need for modified SOFA score, and with the modified CV/total SOFA score, such problems were solved.
Sepsis is managed at the emergency department, ICU, and sub-ICU/ward.1021 We validated the modified SOFA score in ED and ICU; data from other types of ICU, sub-ICUs or other wards might be needed for more extensive validation.
There are several limitations with this study. First, the data of this study drew from ICUs at 6 different centers, but all from within a single country. It needs multi-national validation. Hospital D had a little different baseline characteristic, but sensitivity analysis excluding Hospital D showed similar performance. Therefore, heterogeneity of baseline characteristics of participating hospitals could be an advantage of this study. Second, because this is a retrospective analysis, there are concerns about data completeness and missing values. There are a few missing variables to calculate the SOFA score. We used normal imputation and last observation carried forward approach.22 The results of two imputation methods are similar. In addition, the results of complete analysis drawn from patients without missing data were nearly identical to those with some missing variables, implying minimal effects of missing data on the primary analysis. However, the missing lactate values are one of limitations of this study. Third, the SOFA score has not been developed to predict mortality. Many prior studies have, however, evaluated the performance of the SOFA score to predict mortality, and in the definition of Sepsis-3, the SOFA score’s discriminatory power was evaluated to predict in-hospital mortality.515232425 Lastly, the predictive validity of the modified SOFA score may differ depending on the route of admission to the ICU; however, additional analysis according to the route of admission (general ward, other location) was not performed.
In patients with sepsis in the ICU, the modified SOFA score performed better than the original SOFA score in predicting 28-day mortality.
 XML Download
XML Download